Page 5 of 11
AS10.3-4 | Communication, Medical Errors and Medication Errors in Anaesthesia — SDL Guide (Part 2)
Prevention Strategies for Communication Failures and Medication Errors
Error prevention in anaesthesia operates simultaneously at the individual, team, and system levels. The most effective interventions are those that make the safe action the default — that design the environment and process so that a healthcare worker has to actively override the safe pathway to cause harm, rather than requiring active vigilance to prevent it. This is the principle of forcing functions and error-proof design, borrowed from human-factors engineering. A hierarchy of controls exists — from the most reliable (system redesign) to the least reliable (individual vigilance) — and any safety strategy that relies primarily on individual vigilance will eventually fail because human attention and memory are finite and unpredictable resources.
System-level medication-safety strategies (the most reliable and durable tier):
- Standardised drug labelling: colour-coded syringe labels by drug class (e.g., blue for muscle relaxants, red for vasopressors, green for antibiotics) as recommended by the International Organization for Standardization (ISO 26825) and the AAGBI (Association of Anaesthetists, Great Britain and Ireland) guidelines. The same visual coding system across all theatres in a hospital reduces the cognitive load of working in an unfamiliar environment.
- Physical separation of LASA drugs: potassium chloride concentrated injection is stored separately from sodium chloride (the most lethal LASA pair in ward medicine); adrenaline 1:1000 is stored in a separate tray from adrenaline 1:10,000; oxytocin is kept in a labelled, dedicated section away from other vasoactive drugs.
- Smart infusion pumps with dose-error reduction software (DERS): programmable pumps that contain a drug library with concentration limits and alert the user when a programmed dose is outside the safe range for the drug-weight combination. DERS catches dose errors that have already been entered before the infusion starts.
- Pre-drawn, pharmacy-prepared syringes: drugs drawn and labelled by pharmacy under controlled conditions, with standardised concentrations, reduce preparation errors in the theatre environment. Where pharmacy preparation is not available, standardised preparation protocols and double-check procedures provide an intermediate layer.
- Tall-man lettering: capitalising the distinguishing letters of LASA drug names on labels — vecuRONIUM vs vasoprESSIN — is an evidence-based, low-cost intervention that reduces visual confusion. The ISMP and WHO both recommend its use.
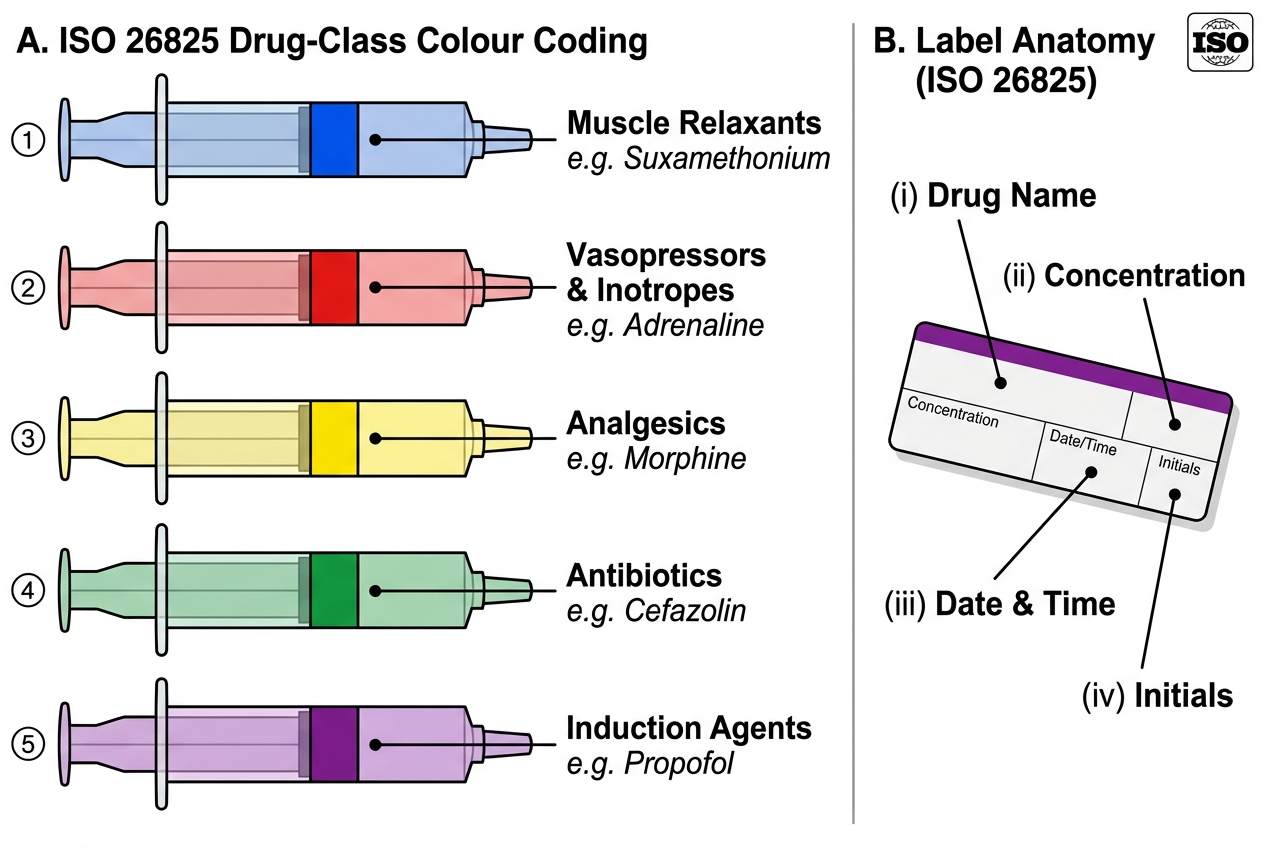
ISO 26825 Colour-Coded Syringe Labelling in Anaesthesia
Individual-level medication-safety habits:
Every anaesthesiologist — regardless of experience — should apply these five habits at every anaesthetic:
- Read the label three times: when removing the ampoule from storage, when drawing up the drug, and when injecting it. Vocalise the drug name and dose (even if working alone) — auditory confirmation adds a second channel.
- Never draw up without labelling immediately: a syringe without a label, even for one minute, is a syringe that can be confused with another.
- Verbal read-back for every verbal drug order: the receiver repeats back the drug name, dose, and route before acting. Confirmation by the sender closes the loop.
- Independent check for high-risk drugs: concentrated electrolytes, neuromuscular blocking agents, insulin, and anticoagulants should be checked by a second person (anaesthesiologist-nurse or anaesthesiologist-anaesthesiologist) before administration. This is the most reliably protective intervention for high-risk drug categories.
- Incident reporting after every near miss: near-miss reporting is a professional obligation and a system-learning tool. A non-punitive just-culture environment is the institutional prerequisite; individual courage to report is the individual requirement.
Communication-safety interventions at the bedside:
- SBAR at every handover — at end of case, use a structured SBAR format to pass care to recovery room staff: Situation (patient, operation done, anaesthetic technique), Background (comorbidities, blood loss, intraoperative events), Assessment (current status — airway, haemodynamics, pain, nausea), Recommendation (oxygen, analgesia, nausea prophylaxis, monitoring requirements, when to escalate).
- Debrief after every adverse event or near miss — even a brief 10-minute structured conversation using the WHO/AHRQ debrief framework: what happened, what went well, what could be improved, what change will be made before the next case.
- Speaking-up training — junior team members require explicit training and institutional permission to challenge perceived errors. Simulation-based crew-resource-management courses provide a safe environment to practise assertive communication against a hierarchy gradient.
Self-Assessment: Error Prevention in Practice
Applying the frameworks of communication failure and medication-error prevention requires not only recall of taxonomy but integration of that knowledge into clinical decision-making — the judgment to recognise a high-risk situation before an error occurs and to intervene effectively once a near miss has happened. The following scenarios and structured questions help consolidate this applied understanding, which is precisely what the AS10.3 and AS10.4 competencies demand at the Knowledge + Skills level.
Scenario A: During an emergency list at 03:00, a fatigued anaesthetic registrar correctly draws up thiopentone 500 mg for induction of a rapid-sequence intubation. In the adjacent syringe position sits a syringe of suxamethonium 100 mg/mL, unlabelled. She reaches for what she believes is the suxamethonium syringe to facilitate intubation. Apply the Swiss Cheese Model: identify three system-level (latent) failures and two individual-level (active) failures that contributed to this near-miss.
Model answer:
Latent failures: (1) unlabelled syringe permitted in the theatre environment (no immediate-labelling policy); (2) two drugs prepared simultaneously in adjacent positions in the same tray without physical separation; (3) night-roster staffing without a mandatory second-check policy for NMBAS in emergency RSI. Active failures: (1) registrar prepared both drugs simultaneously without sequential labelling; (2) registrar reached for a syringe without reading any label under time pressure.
Scenario B: A post-operative patient in recovery becomes acutely agitated. The recovery nurse pages the duty anaesthetic resident and says: "Your patient is agitated." The resident arrives four minutes later to find the patient hypoxic (SpO2 72%) from partial airway obstruction secondary to incomplete reversal. How should this communication failure be analysed, and how should it be prevented?
Model answer: The nurse's message lacked SBAR structure — it named a symptom (agitation) without the vital signs, assessment, or urgency. The resident had no basis to escalate response speed. Prevention: mandatory SBAR structure for all clinical escalation calls; simulation training for recovery nurses to present agitation as a potential airway emergency until proven otherwise; explicit threshold for the ISBAR 'I' (Identify and Importance: "I am calling about a life-threatening situation — please come immediately").
Key exam-recall points:
- Medical error definition: failure of planned action to be completed as intended (execution error) OR wrong plan chosen (planning error).
- Active error (sharp end): committed by the direct caregiver; latent error (blunt end): system deficiency that created the conditions.
- Swiss Cheese Model (James Reason): harm occurs when holes in multiple defensive layers align simultaneously.
- Medication error categories: wrong drug, dose, route, patient, time, concentration — know an example and a prevention for each.
- Communication-failure interventions: closed-loop communication, SBAR handover, two-challenge rule, CRM, debrief.
- LASA drugs: look-alike/sound-alike pairs — tall-man lettering and physical separation are the key system-level mitigations.
- Just culture: accountability without punishment for honest errors — the prerequisite for near-miss reporting and organisational learning.
CLINICAL PEARL
The most reliable predictor of a medication error in the operating theatre is a syringe that was prepared more than a few seconds ago and is not labelled. The labelling-delay is the single, brief, modifiable window in which a safe practice (label immediately after drawing up) becomes a latent error. Develop a personal rule: your hand does not leave the syringe until the label is on it. This takes four seconds. In a 500-case anaesthetic career, this four-second habit prevents more harm than years of formal safety training alone. The companion rule: when someone passes you a syringe, read the label before you touch the plunger, every time, regardless of time pressure. These two habits alone address the root cause of the majority of serious intraoperative drug-swap events.