Page 1 of 17
AS11.1-2 | Oxygen Delivery Devices and Oxygen Therapy Principles — SDL Guide
CLINICAL SCENARIO
A 68-year-old man with known COPD arrives in the emergency department breathless and confused. His SpO₂ is 82% on room air. The nurse reaches for a high-flow non-rebreather mask. You hesitate — this patient has chronic CO₂ retention, and flooding him with uncontrolled high-flow oxygen risks suppressing his hypoxic respiratory drive, worsening hypercapnia, and precipitating respiratory arrest. The right device matters. Choosing between a nasal cannula, a Venturi mask, a simple face mask, and a non-rebreather mask is not a mechanical afterthought — it is a clinical decision with immediate physiological consequences.
WHY THIS MATTERS
Oxygen therapy is arguably the most frequently prescribed treatment in any hospital setting, yet it remains among the most commonly misused. Surveys from multiple countries have found that over 50% of oxygen prescriptions are written without specifying the target SpO₂ range or the appropriate flow rate. In anaesthesia, pre-oxygenation before induction is a non-negotiable life-saving step — its effectiveness depends entirely on selecting the right device and verifying the seal. Across intensive care, emergency medicine, and the ward, the ability to match a patient's physiological need to the correct delivery device — nasal cannula for mild hypoxaemia, Venturi for precise FiO₂ in obstructive lung disease, non-rebreather for acute severe hypoxaemia, BVM for apnoea — is a core competency expected of every clinical graduate. Errors in oxygen prescribing cause preventable harm; competence in this domain is not optional.
RECALL
Before proceeding, activate your knowledge of respiratory physiology from your Year-1 Physiology course. Recall that atmospheric air contains approximately 21% oxygen (FiO₂ 0.21). The fraction of inspired oxygen (FiO₂) determines the partial pressure of oxygen in the alveoli (PAO₂) via the alveolar gas equation. Recall that haemoglobin saturation (SpO₂) is measured by pulse oximetry and reflects arterial oxygen saturation (SaO₂). Recall the normal SpO₂ range (≥94%) and the signs of hypoxaemia: tachycardia, cyanosis, confusion, and reduced oxygen delivery to tissues. Also recall the basic anatomy of the upper airway — nasal passages, oropharynx, nasopharynx — as these determine where different devices interface with the patient. This background makes the device-FiO₂ relationships logical rather than memorised.
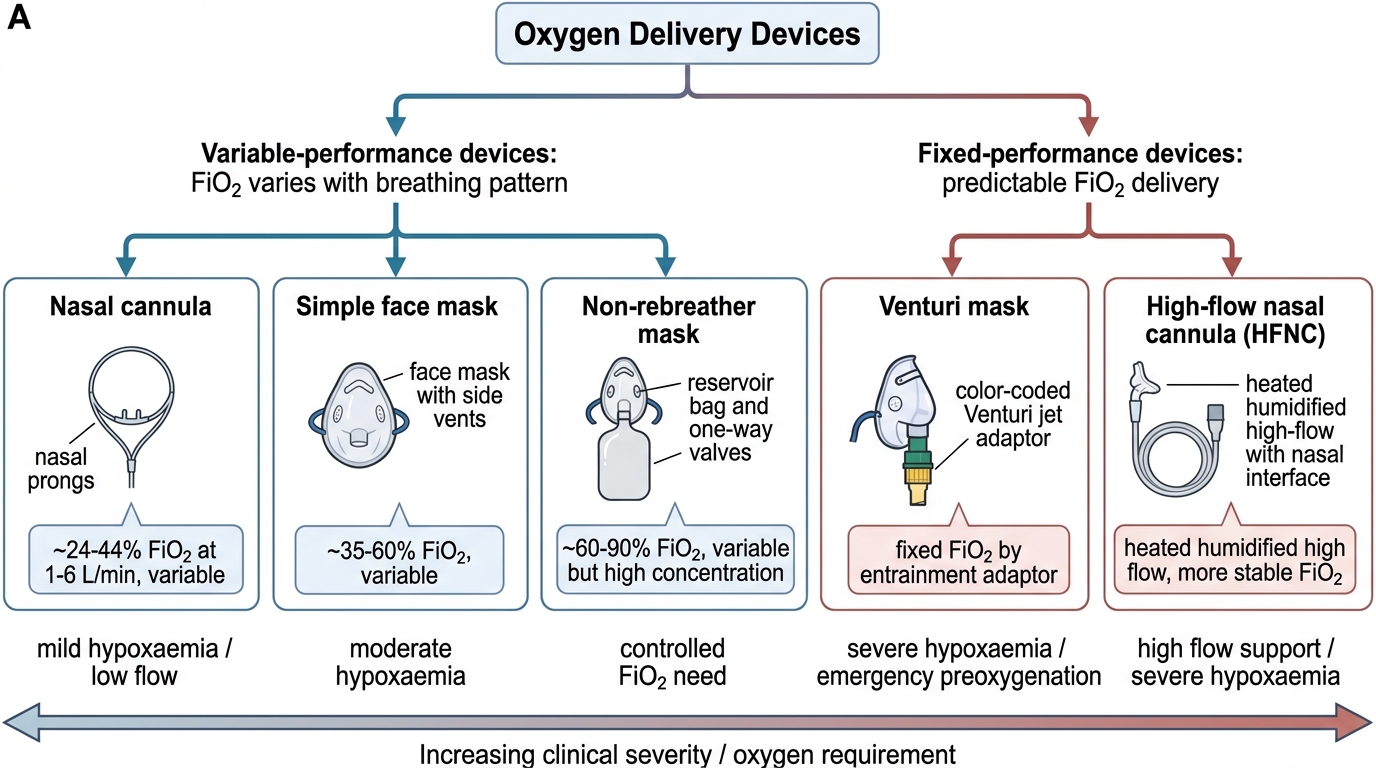
Oxygen Delivery Devices: Classification and Overview
Oxygen delivery devices are broadly classified into two categories based on whether the delivered FiO₂ is controlled and predictable: fixed-performance devices (or high-flow devices), which deliver a precise, predetermined FiO₂ regardless of the patient's breathing pattern, and variable-performance devices (or low-flow devices), in which the FiO₂ delivered depends on the patient's minute ventilation and inspiratory flow rate. This distinction is clinically critical — a patient with COPD and CO₂ retention requires a fixed-performance device so that the inspired oxygen fraction is controlled precisely and the risk of suppressing hypoxic drive is minimised.
Fixed-performance devices entrain room air in a specific ratio using the Venturi (Bernoulli) principle, so that the total gas delivered to the patient always contains the intended FiO₂. Variable-performance devices add a flow of pure oxygen to the inspired gas, but because the patient's inspiratory flow may transiently exceed the device's output, room air is also entrained unpredictably, diluting the FiO₂.
The main devices in clinical use are:
• Nasal cannula — low-flow, variable performance; prongs sit in the nares
• Simple face mask — low-flow, variable performance; covers nose and mouth
• Venturi mask — high-flow, fixed performance; uses colour-coded adapters
• Non-rebreather mask (NRM) — high-flow, variable-to-high performance; with reservoir bag
• Bag-valve-mask (BVM) — manual, for apnoeic or inadequately breathing patients
• High-flow nasal cannula (HFNC) — delivers heated, humidified oxygen up to 60–70 L/min
Each device occupies a specific clinical niche, and selection depends on the severity of hypoxaemia, the need for FiO₂ precision, and the patient's ability to breathe spontaneously.
Classification and Clinical Niche of Oxygen Delivery Devices
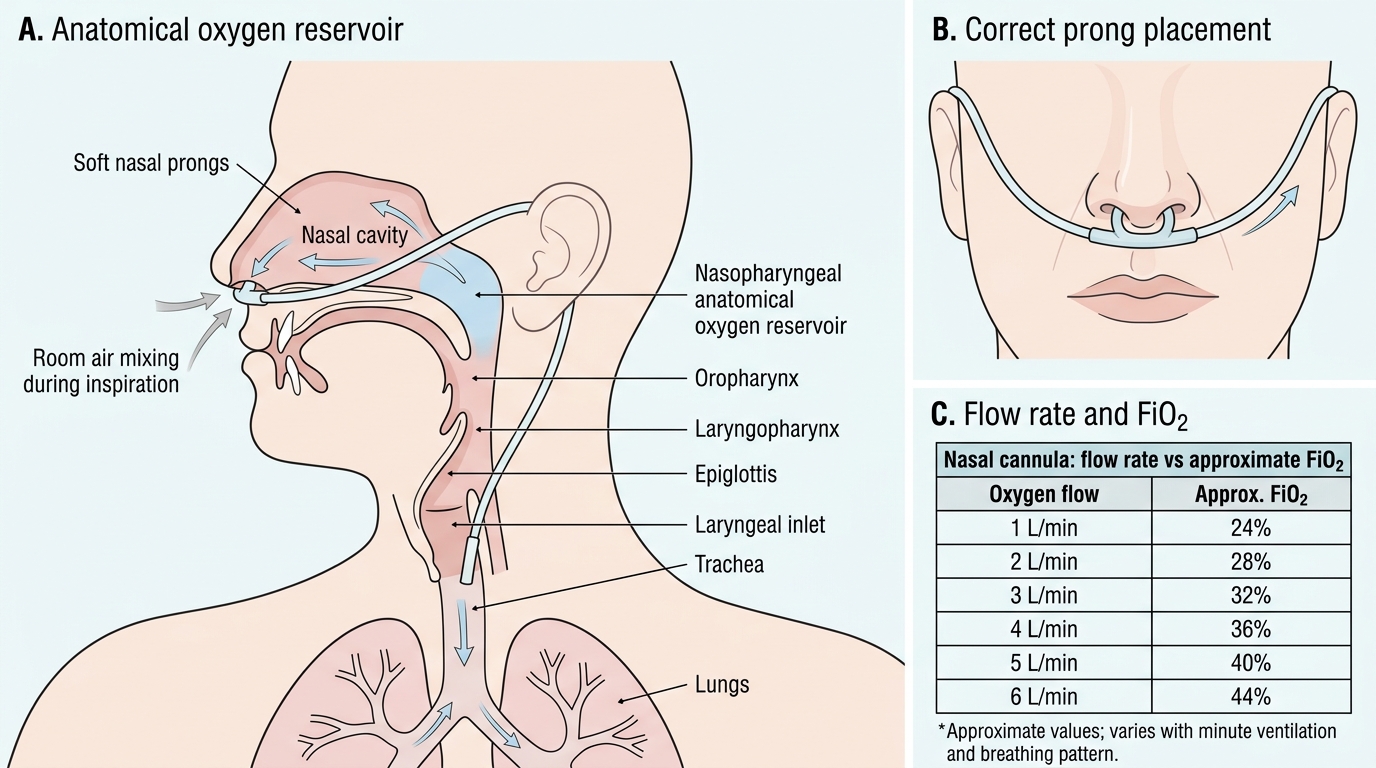
Nasal Cannula: Low-Flow Variable-Performance Device
The nasal cannula (nasal prongs) is the most commonly used oxygen delivery device in clinical practice. It consists of a bifurcated soft plastic tube with two short prongs that sit just inside the nostrils, connected by tubing to a flow meter. Because the nasopharynx acts as an anatomical oxygen reservoir (approximately 50 mL), the inspired FiO₂ is a function of both the supplemental flow rate and the patient's ventilatory pattern.
At a flow rate of 1 L/min, the nasal cannula delivers approximately 24% FiO₂ — effectively 4% above room air's 21% for each litre per minute of flow added. As a rule of thumb widely referenced in clinical anaesthesia texts including Ajay Yadav and Morgan & Mikhail, each additional 1 L/min increases FiO₂ by approximately 3–4%, giving the following approximate ranges:
• 1 L/min → ~24% FiO₂
• 2 L/min → ~28% FiO₂
• 3 L/min → ~32% FiO₂
• 4 L/min → ~36% FiO₂
• 5 L/min → ~40% FiO₂
• 6 L/min → ~44% FiO₂
Flow rates above 6 L/min are generally avoided because they cause nasal mucosal drying and discomfort. The key limitation is that FiO₂ varies with the patient's breathing pattern — a patient with rapid shallow breathing entrains more room air, reducing the effective FiO₂, while a slow deep breather achieves a higher FiO₂ at the same flow rate. This unpredictability makes the nasal cannula unsuitable when precise FiO₂ control is required.
Clinical advantages include patient comfort, the ability to eat and speak during therapy, and suitability for long-term use. The nasal cannula is appropriate for mild hypoxaemia (SpO₂ 90–94% on room air) in spontaneously breathing patients who do not require tight FiO₂ control.
Nasal Cannula Oxygen Delivery
Simple Face Mask: Moderate-Flow Variable-Performance Device
The simple face mask is a clear plastic mask covering the nose and mouth that contains small exhalation ports on the sides. The mask body itself acts as an oxygen reservoir with a volume of approximately 100–200 mL. Oxygen flows continuously into the mask, and during inspiration the patient inhales a mixture of the reservoir gas and room air entrained through the side ports.
The simple face mask delivers an FiO₂ in the range of approximately 40–60% at flow rates of 5–10 L/min. A minimum flow of 5 L/min is required to flush the exhaled CO₂ out of the mask; flow rates below 5 L/min allow CO₂ re-breathing, which is clinically unacceptable. At 5–6 L/min the delivered FiO₂ is approximately 40%; at 10 L/min it approaches 60%, though this is highly variable depending on the patient's minute ventilation and the mask seal.
The simple face mask is appropriate for patients requiring a moderate increase in FiO₂ who do not need precise control — for example, postoperative patients with moderate hypoxaemia, or patients with pneumonia who are not at risk of CO₂ retention. Its limitations include:
• Variable and unpredictable FiO₂ (less reliable than Venturi)
• Uncomfortable to wear for extended periods
• Blocks the face, impeding communication and eating
• Minimum 5 L/min mandatory to prevent CO₂ re-breathing
Simple face masks should not be used when a fixed, controlled FiO₂ is required, as in COPD with chronic hypercapnia.
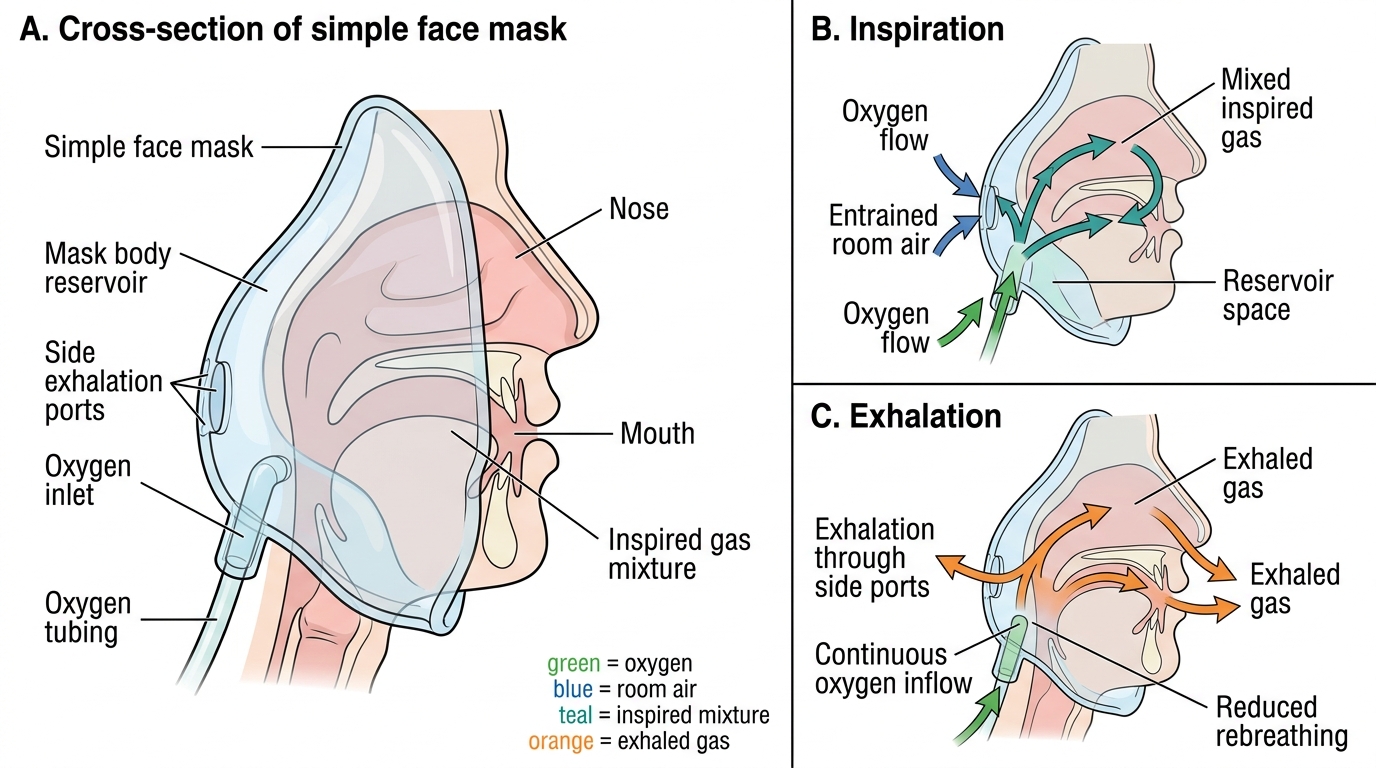
Simple Face Mask Gas Flow During Breathing