Page 2 of 17
AS11.1-2 | Oxygen Delivery Devices and Oxygen Therapy Principles — SDL Guide (Part 2)
Venturi Mask: Fixed-Performance, Precision Oxygen Delivery
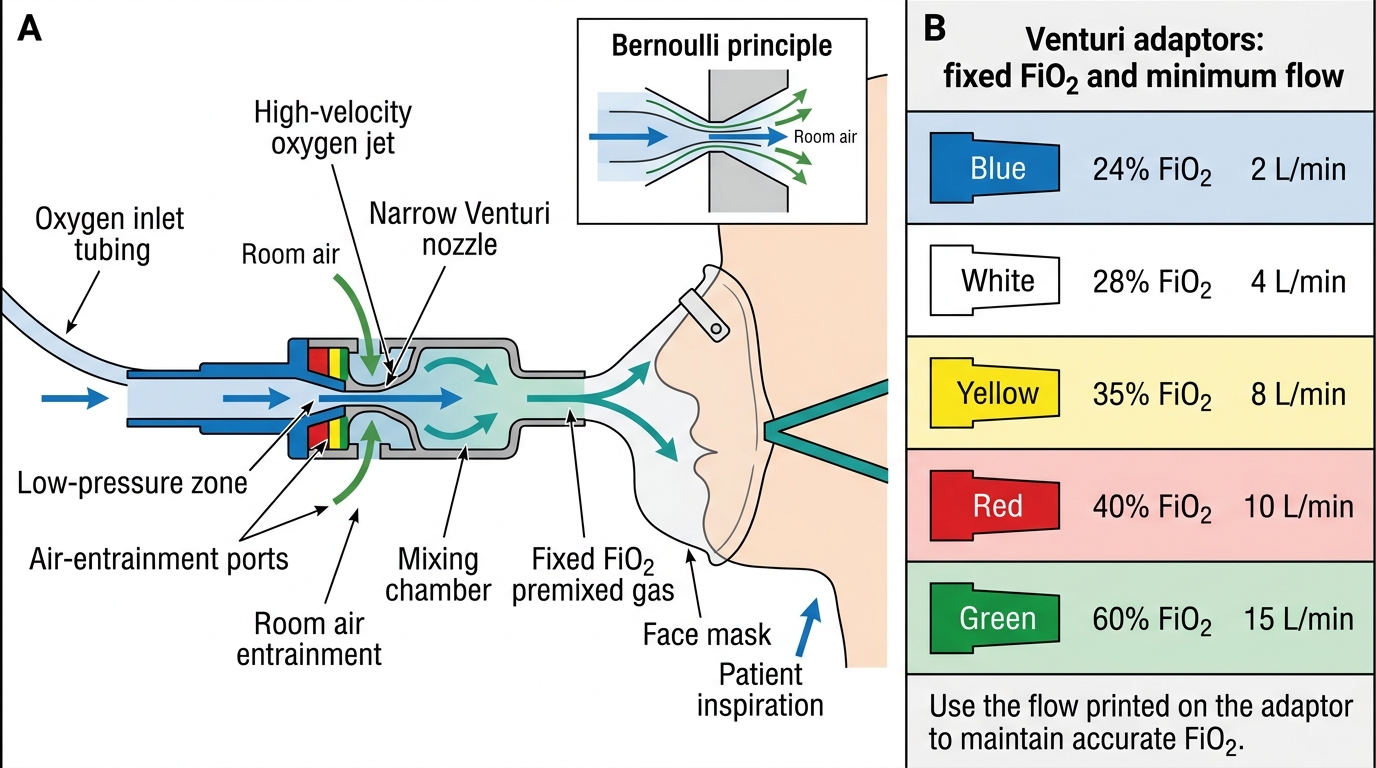
The Venturi mask (Ventimask) is the paradigmatic fixed-performance oxygen delivery device. It operates on the Bernoulli principle: oxygen is forced through a narrow jet (constriction) in the Venturi adaptor, creating a high-velocity stream that entrains room air through side holes in a precise fixed ratio. Because the total gas delivered (oxygen plus entrained air) always arrives at a high flow rate that exceeds the patient's peak inspiratory flow, the patient inhales only the premixed gas from the adaptor — no additional room air is entrained at the mask. This makes the FiO₂ independent of the patient's respiratory pattern, which is the defining clinical advantage.
Venturi masks use colour-coded adaptors, each specifying a fixed FiO₂ and the required oxygen input flow rate:
| Adaptor colour | FiO₂ delivered | O₂ flow required |
|---|---|---|
| Blue | 24% | 2 L/min |
| White | 28% | 4 L/min |
| Yellow | 35% | 8 L/min |
| Red | 40% | 10 L/min |
| Green | 60% | 15 L/min |
Note that the FiO₂ values available are fixed discrete steps — 24%, 28%, 31% (some systems), 35%, 40%, and 60% — not a continuous range. The Venturi mask is the device of choice for patients with COPD and chronic CO₂ retention, where the clinical goal is to raise SpO₂ to 88–92% (not the standard ≥94%) using a controlled, low FiO₂ that does not suppress hypoxic respiratory drive. This target range must be explicitly prescribed.
The Venturi mask is also the device of choice when the clinical team wants to know the precise FiO₂ being administered — for example, when interpreting an arterial blood gas result in context, or when titrating FiO₂ in a complex respiratory patient.
Venturi Mask: Bernoulli Principle and Fixed FiO2 Adaptors
Non-Rebreather Mask and Bag-Valve-Mask
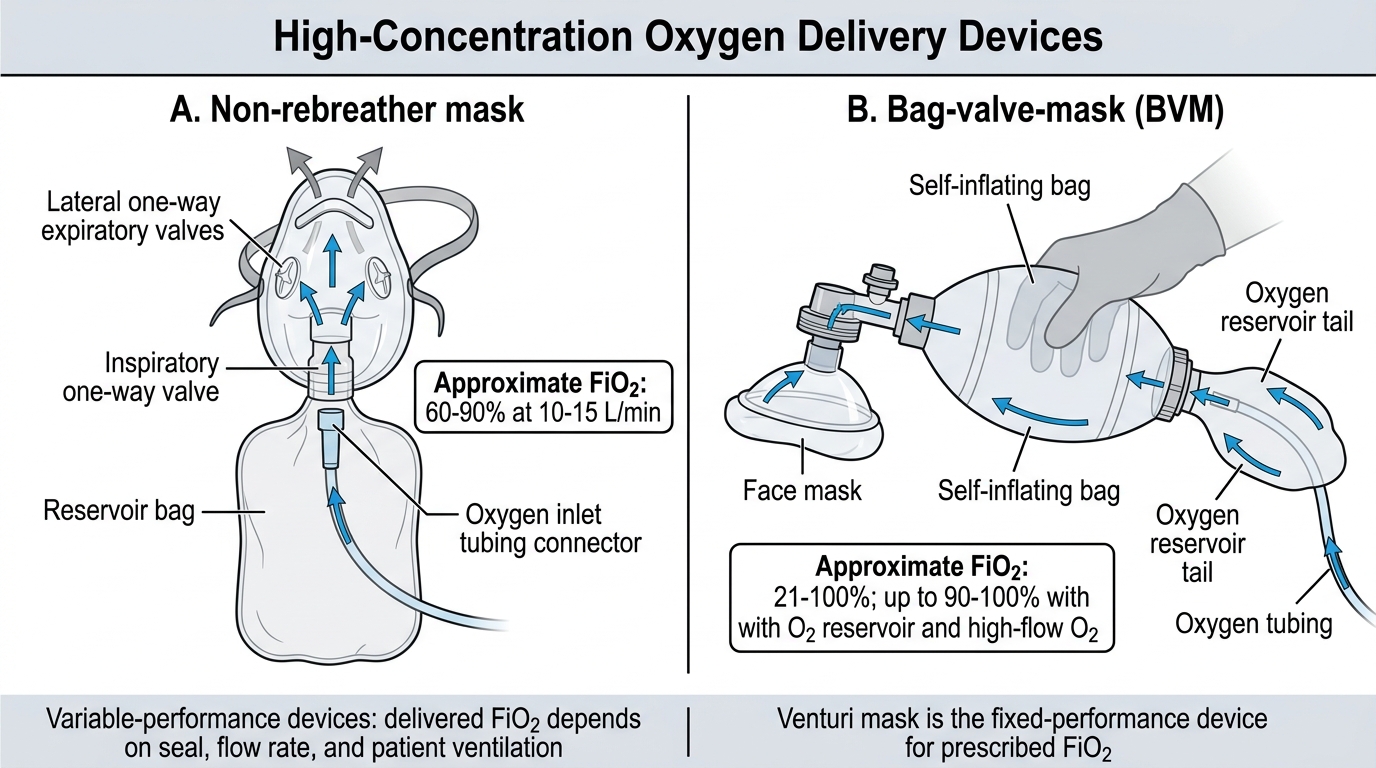
The non-rebreather mask (NRM) is a simple face mask with an attached large reservoir bag (approximately 600–1000 mL) and a set of one-way valves. Oxygen fills the reservoir bag continuously during exhalation; on inspiration the patient draws from the reservoir, getting a high-concentration oxygen bolus. One-way valves on the side ports prevent room air from being entrained during inspiration, and a valve between the mask and reservoir prevents exhaled gas from re-entering the reservoir. At high oxygen flow rates (10–15 L/min), the NRM can deliver an FiO₂ of approximately 60–90%, making it the highest-performing device that can be used in a spontaneously breathing patient.
The NRM is the first-line device for acute, severe hypoxaemia — for example, acute respiratory distress syndrome (ARDS), pulmonary embolism, severe pneumonia, anaphylaxis with bronchospasm, or carbon monoxide poisoning. A critical point: the reservoir bag must be visibly inflated before and during use; if the bag collapses, the patient is rebreathing CO₂ from the exhaled gas. Flow must be sufficient to keep the bag inflated (typically ≥10 L/min).
The bag-valve-mask (BVM) is a self-inflating resuscitation bag connected to a face mask and an oxygen source. It is used for patients who are apnoeic or have inadequate spontaneous ventilation — it can deliver assisted or controlled ventilation. With a reservoir bag attached and oxygen flow at 15 L/min, the BVM can achieve FiO₂ approaching 1.0 (close to 100%). Effective BVM use requires a proper two-person technique for mask seal and bag compression, as single-operator use often results in mask leak and inadequate tidal volumes.
High-flow nasal cannula (HFNC) is a newer modality that delivers heated, humidified gas at flows of 20–70 L/min via wide-bore nasal prongs, achieving FiO₂ up to 1.0 and providing modest CPAP effect (low end-expiratory pressure) through high-flow flushing of the nasopharynx. HFNC has largely replaced NRM in many ICU settings for severe hypoxaemia in spontaneously breathing patients, but requires specialist equipment and careful monitoring.
Non-Rebreather Mask and Bag-Valve-Mask FiO2 Comparison
Principles of Oxygen Therapy: FiO₂, Flow Rate, and Monitoring
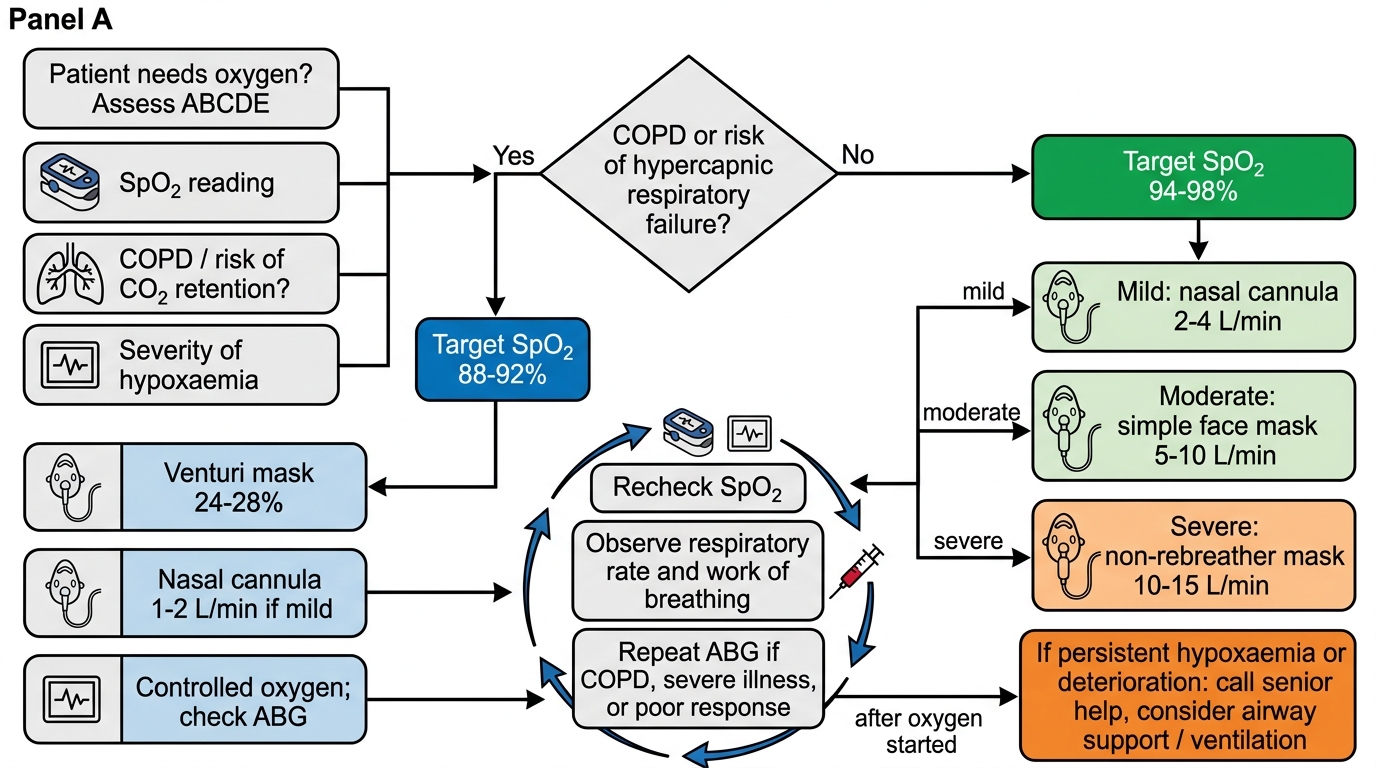
Oxygen therapy involves the supplemental administration of oxygen above atmospheric levels to correct or prevent hypoxaemia. The fundamental principle is that supplemental oxygen raises the alveolar partial pressure of oxygen (PAO₂), which in turn increases arterial partial pressure (PaO₂) and haemoglobin saturation (SpO₂), improving oxygen delivery to tissues (DO₂ = CO × CaO₂). However, oxygen is a drug and must be prescribed with a specific indication, target SpO₂, and device — administering oxygen empirically at an arbitrary flow rate is poor clinical practice.
The relationship between the device's oxygen input flow and the patient's actual FiO₂ is determined by the type of device (fixed vs variable performance), the patient's minute ventilation, and the degree of mask seal. As described in the device sections, the Venturi mask alone guarantees the prescribed FiO₂; all variable-performance devices provide only an approximation.
Target SpO₂ ranges differ by population and clinical context:
• Most adults: target SpO₂ ≥94% (upper limit acceptable — hyperoxia causes vasoconstriction and reactive oxygen species generation)
• COPD with chronic CO₂ retention: target SpO₂ 88–92% — higher targets risk hypercapnia from suppression of hypoxic drive and Haldane effect (shift in CO₂ dissociation curve)
• Acute myocardial infarction without hypoxaemia: oxygen not indicated (normoxaemia is the goal; hyperoxia is harmful)
• Preterm neonates: strictly controlled targets (SpO₂ 90–95%) to prevent retinopathy of prematurity
Monitoring during oxygen therapy includes:
1. Continuous pulse oximetry (SpO₂) — the primary non-invasive monitor; note that SpO₂ can be falsely normal in carbon monoxide poisoning (carboxyhaemoglobin reads as oxyhemoglobin)
2. Arterial blood gas (ABG) — essential in COPD patients and whenever hypercapnia is suspected; monitors PaO₂, PaCO₂, and pH simultaneously
3. Clinical assessment — respiratory rate, work of breathing, level of consciousness, capillary refill, skin colour
4. Device check — confirm correct adaptor (Venturi), bag inflation (NRM), prong position (nasal cannula), and flow rate setting
Oxygen Therapy Prescription Decision Flow