Page 1 of 9
AS2.1-2 | Basic and Advanced Life Support Across Age Groups — SDL Guide
CLINICAL SCENARIO
A 45-year-old man collapses in the hospital corridor outside the operating theatre. He is unresponsive and not breathing normally. You are the first clinician to arrive. Within sixty seconds your actions — or their absence — will determine whether this man survives neurologically intact. Cardiac arrest kills more people worldwide than any single disease, yet the majority of cardiac arrests that occur in witnessed, shockable rhythms are potentially reversible with timely, well-executed resuscitation. The chain of survival exists precisely because every link — early recognition, early CPR, early defibrillation, and post-resuscitation care — is interdependent. A lag of even two minutes between collapse and first compression halves survival probability. This SDL equips you to act without hesitation at every link, across every age group from the neonate in the delivery room to the elderly adult in the ward.
WHY THIS MATTERS
As an anaesthetist you will encounter cardiac arrest in settings where you are the most qualified clinician present: the operating theatre, the recovery room, the pre-operative ward, and occasionally the delivery suite. The NMC 2024 competency framework (AS2.1, AS2.2) requires you to enumerate indications, describe the steps, and demonstrate both Basic Life Support (BLS) and Advanced Life Support (ALS) in a simulated environment. Beyond examination, these skills are never theoretical: a trainee anaesthetist who freezes during an intraoperative arrest, unsure whether to defibrillate VF or give adrenaline first, is a liability to the patient. Fluency in the full resuscitation algorithm — from the initial 30:2 compressions-to-ventilations ratio through to the post-ROSC (return of spontaneous circulation) bundle — is the minimum standard the specialty demands. (References: Morgan & Mikhail's Clinical Anesthesiology, 7th ed.; Ajay Yadav's Short Textbook of Anaesthesia; ERC/Resuscitation Council UK Guidelines 2021.)
RECALL
Before engaging with this SDL, test your baseline knowledge. What is the difference between primary cardiac arrest and respiratory arrest as a cause of cardiac arrest? Which two rhythms are shockable? What does the mnemonic 'DR ABC' represent? If you cannot answer these confidently, revisit the physiology of cardiopulmonary failure before proceeding. You should also recall that the cardiac output depends on heart rate and stroke volume, and that global ischaemia begins within seconds of arrest — the brain sustains irreversible damage within four to six minutes without perfusion. This urgency underpins every time target in the resuscitation guidelines.
Clinical Indications and Relevance of CPR Across Age Groups
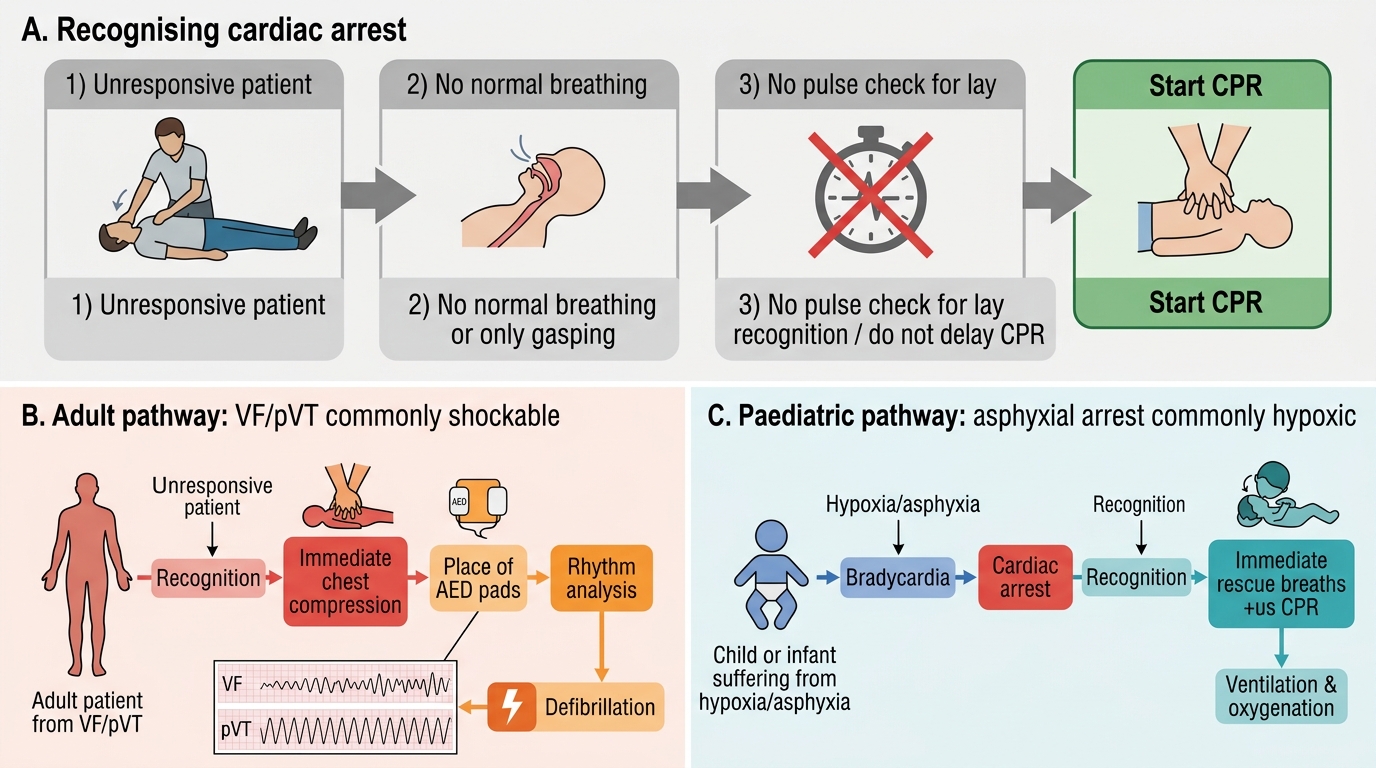
Cardiopulmonary resuscitation (CPR) is indicated whenever a patient is unresponsive and not breathing normally (gasping does not constitute normal breathing). The pathway to arrest differs systematically by age, and recognising this determines which algorithm you apply. In adults, the predominant cause of sudden cardiac arrest is primary cardiac disease — ventricular fibrillation (VF) or pulseless ventricular tachycardia (pVT) from acute myocardial ischaemia. Because the initiating insult is cardiac, early defibrillation is the decisive intervention: every minute without defibrillation reduces survival from VF by approximately ten percent. In children beyond the neonatal period, the predominant pathway is asphyxial arrest — respiratory failure precedes and causes cardiac arrest. The resulting rhythm is usually bradycardia progressing to asystole or pulseless electrical activity (PEA), not a shockable rhythm. Consequently, oxygenation and ventilation take priority, and the ratio adjustments in paediatric BLS reflect this: for a lone rescuer giving paediatric CPR, begin with five rescue breaths before compressions. In neonates at birth, the priority is identical — apnoea from birth asphyxia leads to bradycardia, and lung inflation is the single most effective resuscitation manoeuvre. Understanding these age-specific pathophysiological differences prevents the critical error of treating a child with an asphyxial arrest solely as if the primary event were cardiac.
Clinical recognition of arrest requires three integrated observations: (1) the patient is unresponsive to stimuli (shake and call), (2) there are no normal breaths — absence of breathing or only agonal gasps — after a ten-second check, and (3) in the healthcare setting, absence of a palpable pulse (checked simultaneously over a maximum of ten seconds; do not delay CPR seeking an uncertain pulse). Agonal breathing — irregular, laboured, noisy gasps — is a brainstem reflex that persists for seconds to minutes after cardiac arrest and must not be mistaken for normal breathing. This recognition error is one of the most common causes of delayed CPR initiation.
Indications for initiating CPR are therefore: any patient who is unresponsive with absent or abnormal breathing, regardless of whether a definitive rhythm is yet known. CPR is not indicated in a patient who is conscious and breathing, or in a patient with a valid Do-Not-Resuscitate (DNR) order documented and accessible.
Clinical Recognition of Cardiac Arrest
Anatomy and Governing Physiological Principles
Effective chest compressions generate cardiac output by two complementary mechanisms: direct cardiac compression and the thoracic pump. In direct cardiac compression, external pressure squeezes the heart between the sternum anteriorly and the thoracic spine posteriorly, displacing blood from the ventricles into the aorta and pulmonary artery. In the thoracic pump mechanism, the rise in intrathoracic pressure during compression propels blood out of the chest, while the fall in pressure during recoil draws venous blood back into the right heart. Both mechanisms depend critically on chest wall compliance and complete chest recoil: if the rescuer leans on the chest between compressions, intrathoracic pressure remains elevated, venous return is impaired, and coronary perfusion pressure — the arterial-minus-right-atrial pressure gradient that drives coronary flow — collapses. This is why full chest recoil is a quality metric equivalent in importance to compression depth and rate.
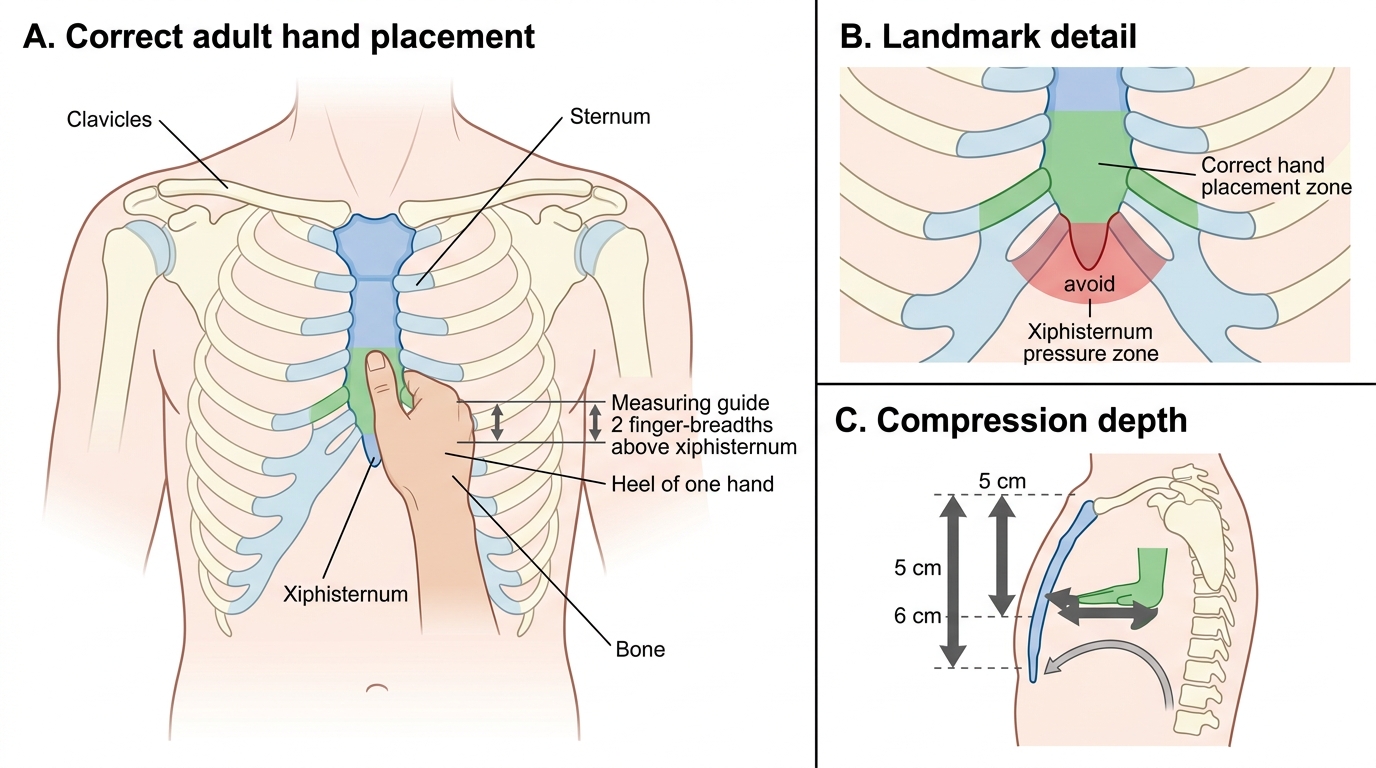
The landmark for adult chest compressions is the lower half of the sternum, placing the heel of one hand over the sternum two finger-breadths above the xiphisternum. The correct depth in adults is 5–6 centimetres (not deeper, as rib fractures and aortic laceration become significant risks beyond 6 cm, and not shallower, as coronary perfusion pressure is inadequate). The rate is 100–120 compressions per minute — below 100/min reduces output, and above 120/min shortens diastolic filling time and also reduces output. Interruptions to compressions must be minimised; each pause causes coronary and cerebral perfusion to fall precipitously and requires several compressions to re-establish.
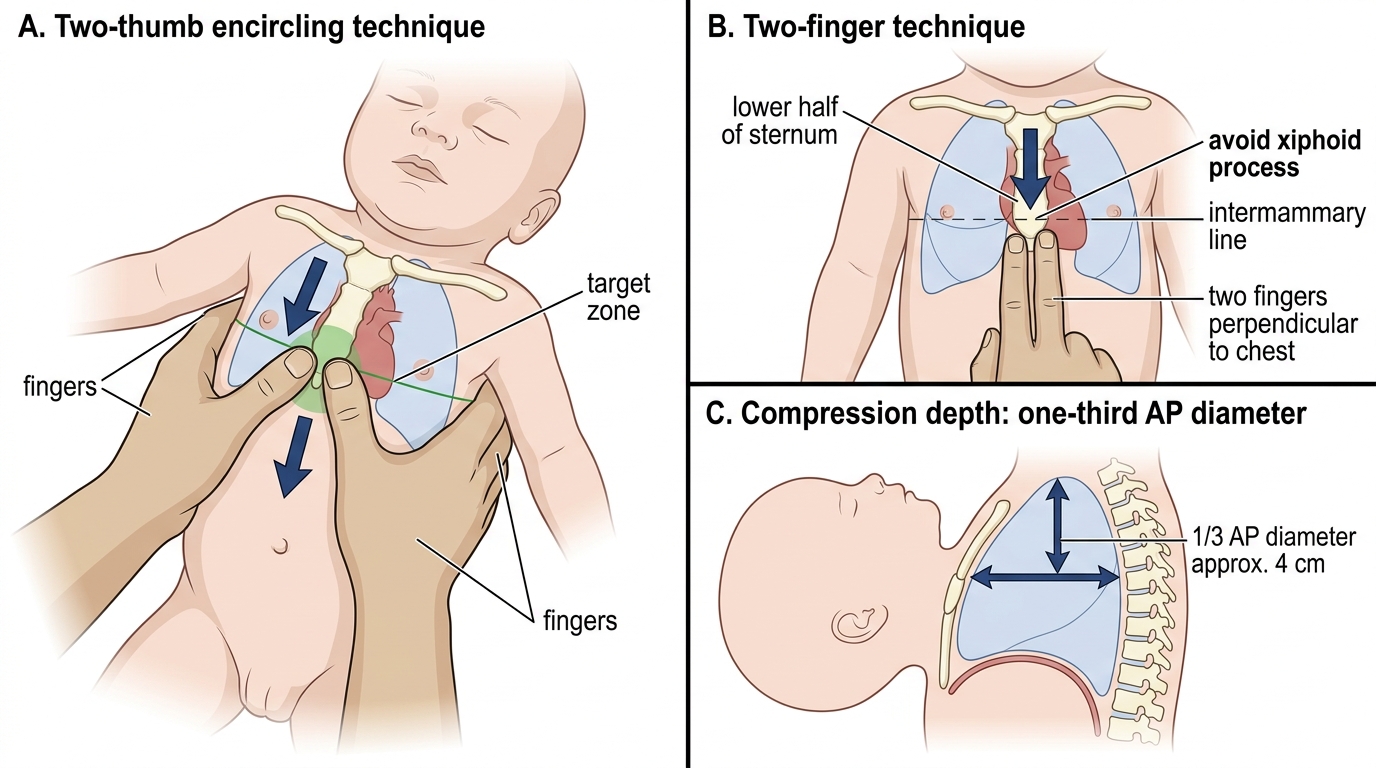
For children (one to eight years, or pre-pubescent), the landmark is the same (lower sternum) but depth is one-third of the anteroposterior chest diameter — approximately 5 cm in children and 4 cm in infants. Two fingers suffice for infants in the single-rescuer setting; the two-thumb encircling technique is preferred for two healthcare-provider rescuers because it generates higher coronary perfusion pressures. For neonates, the same two-thumb encircling technique is used, with a target depth of one-third the AP chest diameter (approximately 1.5–2 cm).
The ratio of compressions to ventilations determines the balance between circulation and oxygenation. In adults, the ratio is 30:2 for both single and two-rescuer BLS: thirty compressions followed by two ventilations, minimising the cumulative pause from ventilation. Once an advanced airway is secured (supraglottic airway or tracheal tube), asynchronous ventilation at 10 breaths per minute is given while compressions continue uninterrupted. In children with a lone rescuer, the ratio is 30:2 (matching adult BLS for practicality), but with two healthcare rescuers the paediatric ratio reverts to 15:2 to provide proportionally more ventilation to the asphyxia-predominant aetiology. In neonates, the ratio is 3:1 — three compressions for every one ventilation — again prioritising ventilation.
Adult Chest Compression Hand Placement
BLS Technique: Adult, Paediatric, and Neonatal
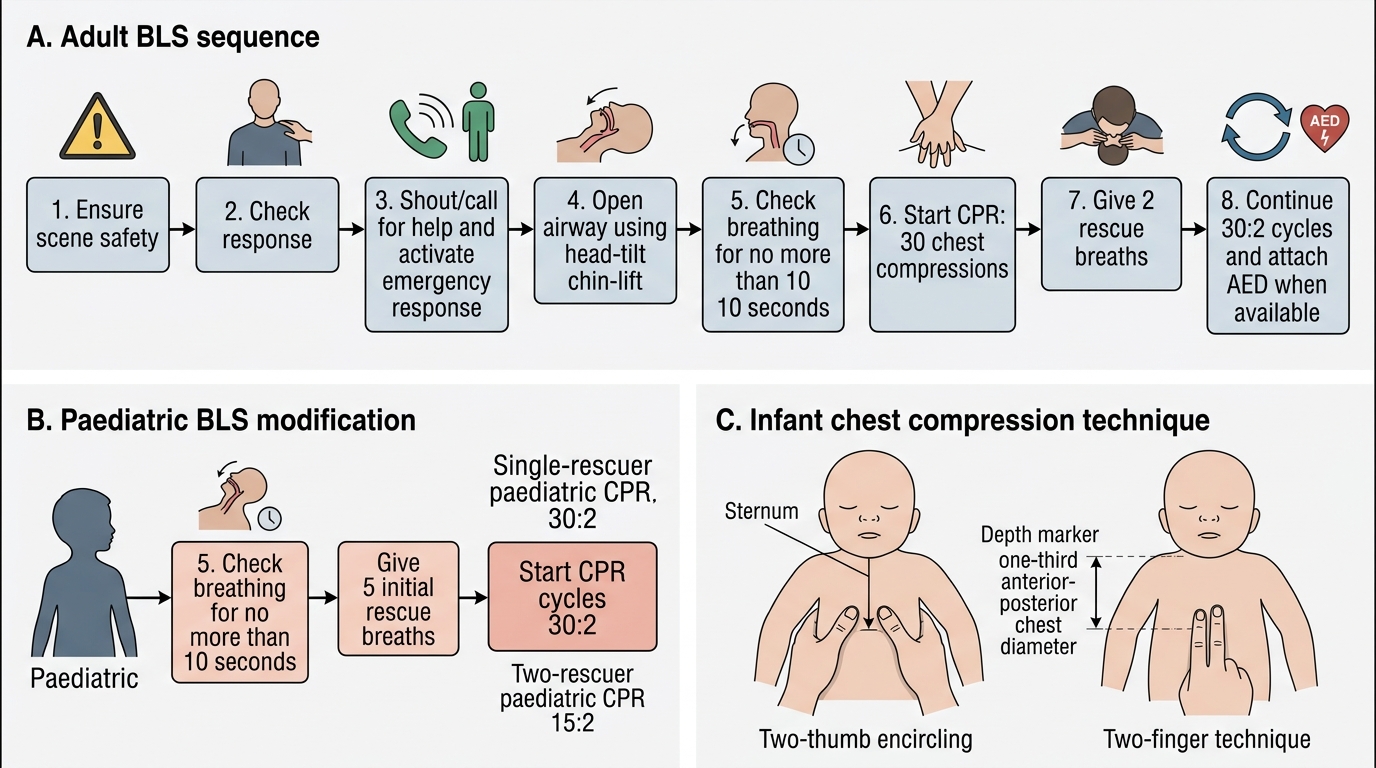
Basic Life Support is the foundation of resuscitation — it buys time for defibrillation and ALS. The adult BLS sequence begins with personal safety (approach only when the scene is safe), then assessment: shake the shoulders and call loudly ('Are you all right?'). If no response, shout for help and dial the emergency number. Open the airway using the head-tilt–chin-lift (or jaw thrust alone if cervical injury is suspected). Look, listen, and feel for no more than ten seconds for normal breathing. If absent, deliver two rescue breaths (each over one second, enough to cause visible chest rise), then immediately begin thirty chest compressions.
Compressions are performed with the rescuer kneeling beside the patient, arms straight and locked, shoulders directly above the hands on the sternum. The depth is 5–6 cm in an adult, rate 100–120 per minute, with full chest recoil between compressions. After thirty compressions, two further breaths are given. This 30:2 cycle continues without interruption until the defibrillator arrives, the patient shows signs of life, or rescuers are exhausted. If the rescuer is unwilling or unable to provide mouth-to-mouth, continuous chest compressions without ventilations are acceptable as an interim measure for adult bystander CPR (compression-only CPR); for healthcare providers, full CPR including ventilations is the standard.
For children aged one year to puberty, the sequence begins with five initial rescue breaths (not two), reflecting the asphyxial mechanism. Head-tilt is more cautious — the prominent occiput in young children can cause flexion rather than extension; a neutral or gently extended position maintains the airway. Compressions are delivered with one or two hands depending on the child's size, at one-third AP chest diameter depth (~5 cm), at the same rate of 100–120/min. The ratio is 30:2 for a lone rescuer or 15:2 for two healthcare providers.
For infants under one year, the same five initial rescue breaths apply. The airway is held in a neutral position (excessive extension obstructs the trachea in an infant). The mouth-and-nose technique provides breaths. The two-finger technique (single rescuer) or two-thumb encircling technique (two rescuers) delivers compressions at one-third AP depth (~4 cm), 100–120/min, ratio 30:2 (lone) or 15:2 (two healthcare providers).
For neonates at birth, the Newborn Life Support (NLS) algorithm applies. If the infant is not breathing at birth, dry and stimulate, assess tone and heart rate. If heart rate less than 100/min, inflate the lungs — five sustained inflation breaths of two to three seconds each using an appropriate mask and inflation pressure. If the heart rate falls below 60/min despite adequate ventilation, begin compressions at the 3:1 ratio (three compressions then one ventilation), coordinated with ventilation, using the two-thumb encircling technique.
Adult and Paediatric Basic Life Support Algorithm
Infant Chest Compression Techniques