Page 2 of 9
AS2.1-2 | Basic and Advanced Life Support Across Age Groups — SDL Guide (Part 2)
Advanced Life Support: The Algorithm, Drugs, and Defibrillation
Advanced Life Support (ALS) builds on BLS by adding rhythm analysis, defibrillation, airway adjuncts, and pharmacological therapy. The central organising principle of ALS is the identification of the cardiac arrest rhythm into one of two categories: shockable (ventricular fibrillation and pulseless ventricular tachycardia — VF/pVT) and non-shockable (asystole and pulseless electrical activity — PEA). This distinction is not merely academic; it determines whether defibrillation is indicated. Defibrillation delivers a synchronised depolarisation of the myocardium to terminate the disorganised electrical activity of VF or pVT, allowing the natural pacemaker to resume. Defibrillation of asystole or PEA provides no benefit and must be avoided.
The adult ALS algorithm proceeds as follows. Once a cardiac arrest is confirmed and BLS is underway, attach the defibrillator as soon as it arrives. Pause CPR only long enough to analyse the rhythm (2–3 seconds with an automated external defibrillator; manual analysis by the team leader). If VF or pVT is identified, deliver one shock (biphasic: 150–200 J for the first shock, 150–360 J for subsequent shocks; monophasic: 360 J). Immediately resume CPR for two minutes without waiting to check the rhythm — post-shock CPR is critical because even if defibrillation terminates VF the heart may not generate adequate output immediately. After two minutes, pause, check the rhythm, and shock again if VF/pVT persists. Give adrenaline (epinephrine) 1 mg IV after the third shock (i.e. during the second two-minute CPR loop) and every 3–5 minutes thereafter. Give amiodarone 300 mg IV after the third shock for refractory VF/pVT; a second dose of 150 mg may be given after the fifth shock. If asystole or PEA is identified, continue CPR for two minutes without shocking, give adrenaline 1 mg IV immediately, reassess the rhythm at two minutes, and search for reversible causes (the 4Hs and 4Ts).
The 4Hs and 4Ts mnemonic captures reversible causes of cardiac arrest: Hypoxia, Hypovolaemia, Hypo/hyperkalaemia and metabolic disorders, Hypothermia (the 4Hs); and Tension pneumothorax, Tamponade (cardiac), Toxins/drugs, Thromboembolism (the 4Ts). Systematic review of these reversible causes must run in parallel with each two-minute CPR cycle, because no drug or electrical therapy corrects an underlying hypovolaemia or tamponade.
Airway management during ALS proceeds stepwise. Initial ventilation uses a bag-valve-mask (BVM) by two providers — one maintaining the mask seal with two hands while the second squeezes the bag. Early insertion of a supraglottic airway device (laryngeal mask airway or i-gel) avoids the interruption required for endotracheal intubation and is acceptable as a primary airway in most adults. Tracheal intubation remains the gold standard where the skill exists and can be achieved without prolonged interruption to CPR; video laryngoscopy is preferred when available. Once intubated, ventilate at ten breaths per minute asynchronously while compressions continue uninterrupted.
Vascular access during CPR should be established as quickly as possible without interrupting chest compressions. Peripheral IV access (antecubital or external jugular) is first-line. If peripheral access fails after two attempts, use intraosseous (IO) access — the tibial head is the most common site in adults and all paediatric age groups. Drug pharmacokinetics via the IO route are equivalent to IV. Endotracheal drug administration is no longer recommended in modern ALS guidelines.
For children, the paediatric ALS algorithm mirrors the adult algorithm in structure but applies age-appropriate energy doses: 4 J/kg for each defibrillation shock (both first and subsequent shocks). Adrenaline dose in children is 10 mcg/kg (0.1 mL/kg of 1:10,000 solution). Amiodarone dose is 5 mg/kg IV for the third shock, same dose again for the fifth shock. IO access is used early if IV access fails, and the tibial head is the standard site from infancy.
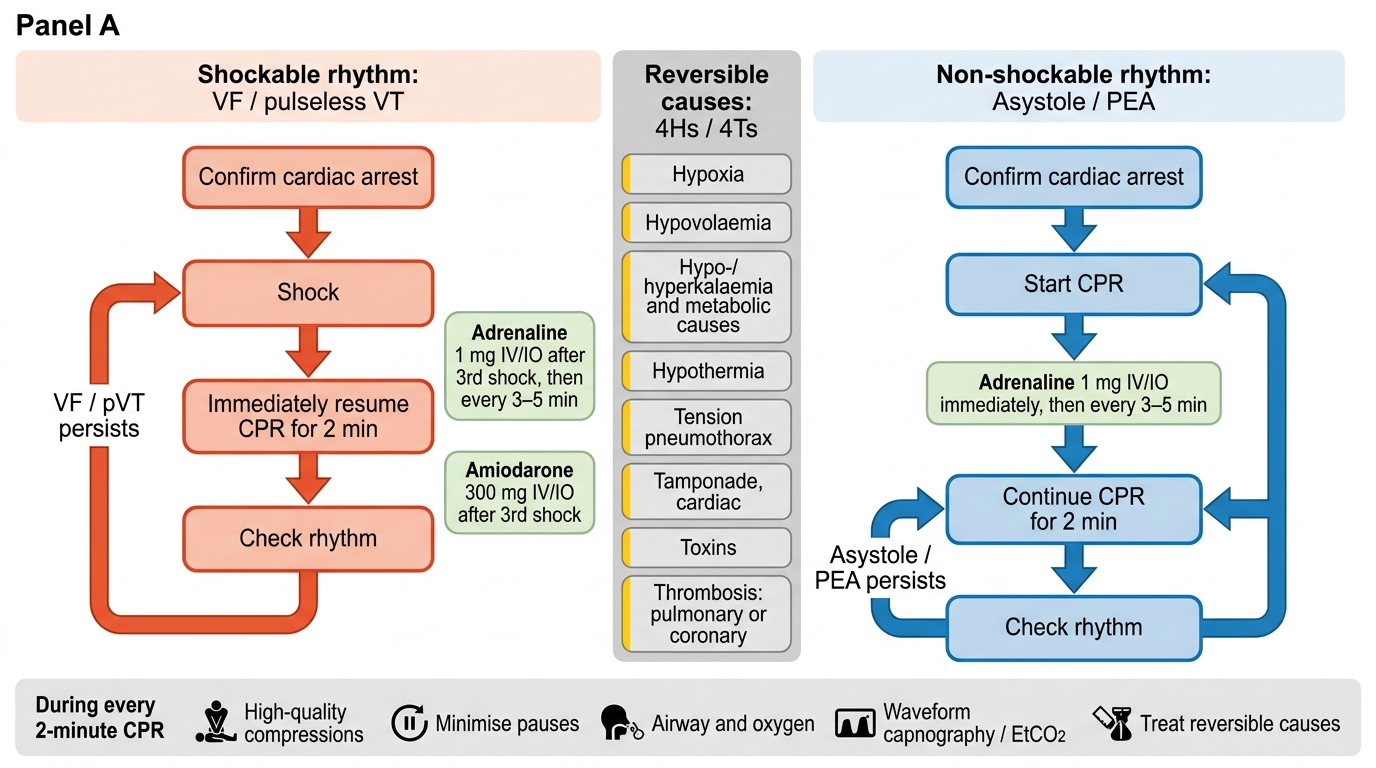
Adult ALS Cardiac Arrest Algorithm
Monitoring During CPR and Indicators of Quality
High-quality CPR is the single most modifiable determinant of outcome in cardiac arrest, and monitoring during resuscitation provides real-time feedback to guide technique and detect return of spontaneous circulation (ROSC). Several monitoring modalities are available during an ALS resuscitation and each provides distinct information about the adequacy of effort and the state of the circulation.
End-tidal CO₂ (EtCO₂) is the most clinically valuable non-invasive monitor during CPR. EtCO₂ reflects pulmonary blood flow, which during CPR is a direct surrogate for cardiac output generated by chest compressions. A consistently low EtCO₂ (less than 10 mmHg) despite ventilation indicates inadequate cardiac output from compressions, prompting review of rate, depth, and recoil. A sudden sustained rise in EtCO₂ to above 35–40 mmHg — without a change in ventilation rate — is one of the most reliable indicators of ROSC, often preceding a palpable pulse. EtCO₂ also serves as a prognostic marker: persistently very low values (<10 mmHg) after 20 minutes of well-executed ALS are associated with very poor outcome and may inform the decision to cease resuscitation.
Cardiac rhythm monitoring via defibrillator electrodes or adhesive pads provides the rhythm diagnosis at the two-minute checkpoint. The team leader interprets the rhythm, decides on shock or no-shock, and ensures the pause for analysis is as brief as possible (target <5 seconds pre-shock). Hands-free adhesive pads are preferred over manual paddles as they allow continuous monitoring and reduce contact time.
Arterial line waveform (where an arterial catheter is already in situ, as is common in an intraoperative arrest) provides a direct and continuous measure of perfusion pressure during CPR. A target diastolic blood pressure above 25 mmHg is associated with improved coronary perfusion and better likelihood of ROSC; if arterial diastolic pressure is consistently below this threshold, compression depth and rate should be adjusted.
Pulse oximetry (SpO₂) is unreliable during CPR due to absent pulsatile flow, and values should not be used to guide ventilation during arrest. It becomes useful post-ROSC, when oxygen saturations should be maintained at 94–98% (avoid hyperoxia, which worsens post-arrest neurological injury).
CPR quality feedback devices — accelerometers embedded in defibrillator pads or standalone puck devices — provide real-time audio and visual feedback on compression rate, depth, and recoil, and have been shown to improve adherence to guideline targets during training and clinical resuscitation. Their use is encouraged whenever available.
Recognising ROSC requires stopping compressions and checking for signs: a palpable pulse (carotid or femoral), return of normal cardiac rhythm on monitor, and patient movement or breathing. After confirming ROSC, the post-ROSC care bundle begins immediately.
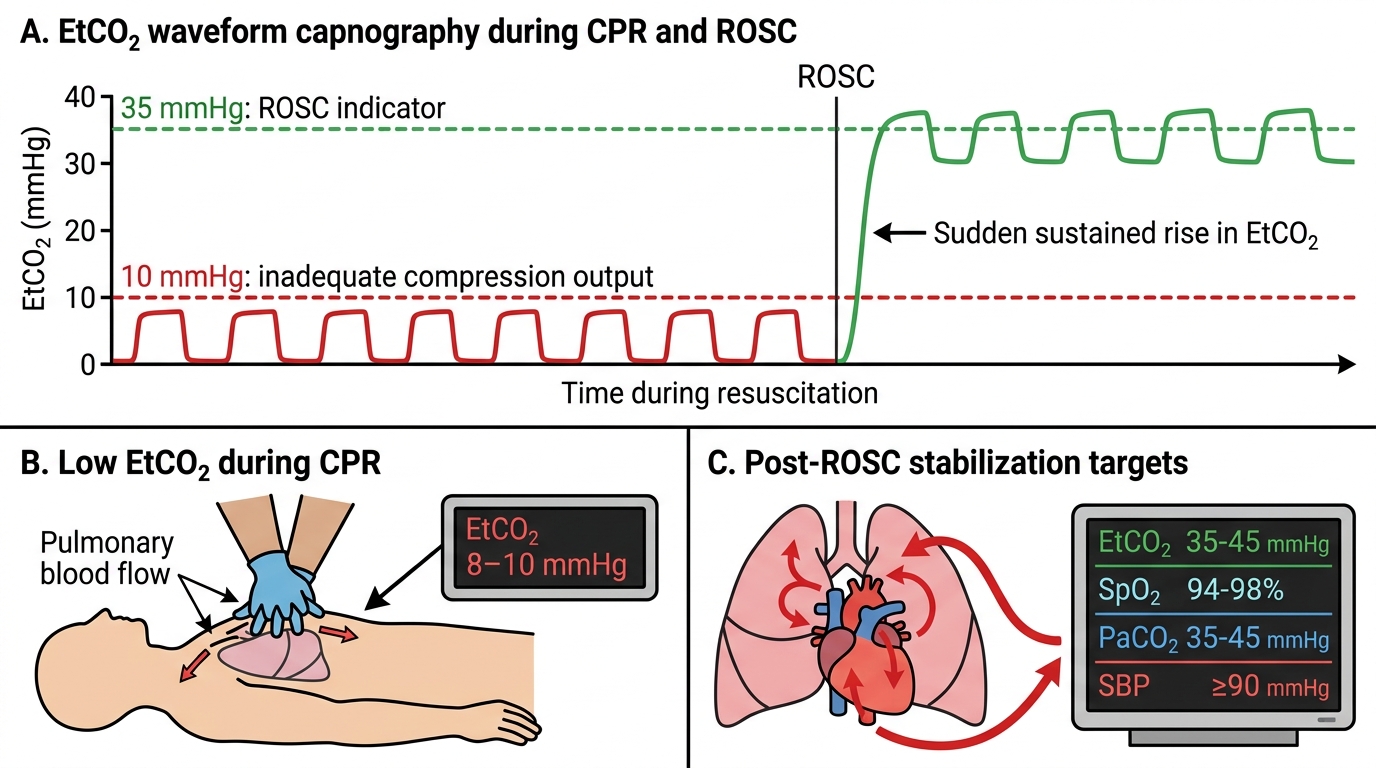
EtCO2 Rise as an Indicator of ROSC During CPR
Post-Resuscitation Care and Team Roles
The immediate post-ROSC period carries a high risk of secondary deterioration from the 'post-cardiac arrest syndrome' — a systemic inflammatory response combining myocardial dysfunction, neurological injury, systemic ischaemia-reperfusion injury, and the precipitating pathology. Structured post-ROSC care addresses each component and has been shown to double neurologically favourable survival compared with unstructured care.
Key elements of the post-ROSC bundle include: (1) Airway: if not already intubated, consider tracheal intubation in unconscious patients to protect the airway and allow controlled ventilation. (2) Oxygenation: titrate FiO₂ to maintain SpO₂ 94–98%; avoid hyperoxia (PaO₂ >300 mmHg is associated with worse neurological outcomes). (3) Ventilation: target normocapnia (PaCO₂ 35–45 mmHg); avoid hyperventilation, which causes cerebral vasoconstriction. (4) Circulation: treat hypotension (systolic <90 mmHg) aggressively with IV fluids and vasopressors (noradrenaline or adrenaline infusion); obtain 12-lead ECG and urgent coronary angiography if ST-elevation MI (STEMI) is the likely cause. (5) Targeted temperature management (TTM): for unconscious survivors of out-of-hospital cardiac arrest, targeted temperature management at 36°C (or 32–36°C as per current evidence) for 24 hours reduces cerebral metabolic demand and improves neurological recovery; fever (>37.7°C) must be actively prevented. (6) Neurological monitoring: clinical assessment, EEG monitoring, and CT brain as clinically indicated.
Effective resuscitation depends as much on team dynamics as on technical skill. The team leader maintains situational awareness, directs tasks, calls the rhythm, decides on shocks, reviews the 4Hs/4Ts, and documents timing. Compressors rotate every two minutes to prevent fatigue-related quality degradation. An airway provider manages the mask and device. A drug nurse/provider prepares and administers medications, noting dose and time. A documenter records all events with timestamps. Closed-loop communication — where an instruction is repeated back and confirmed — prevents errors during the high-stress, fast-paced arrest environment.
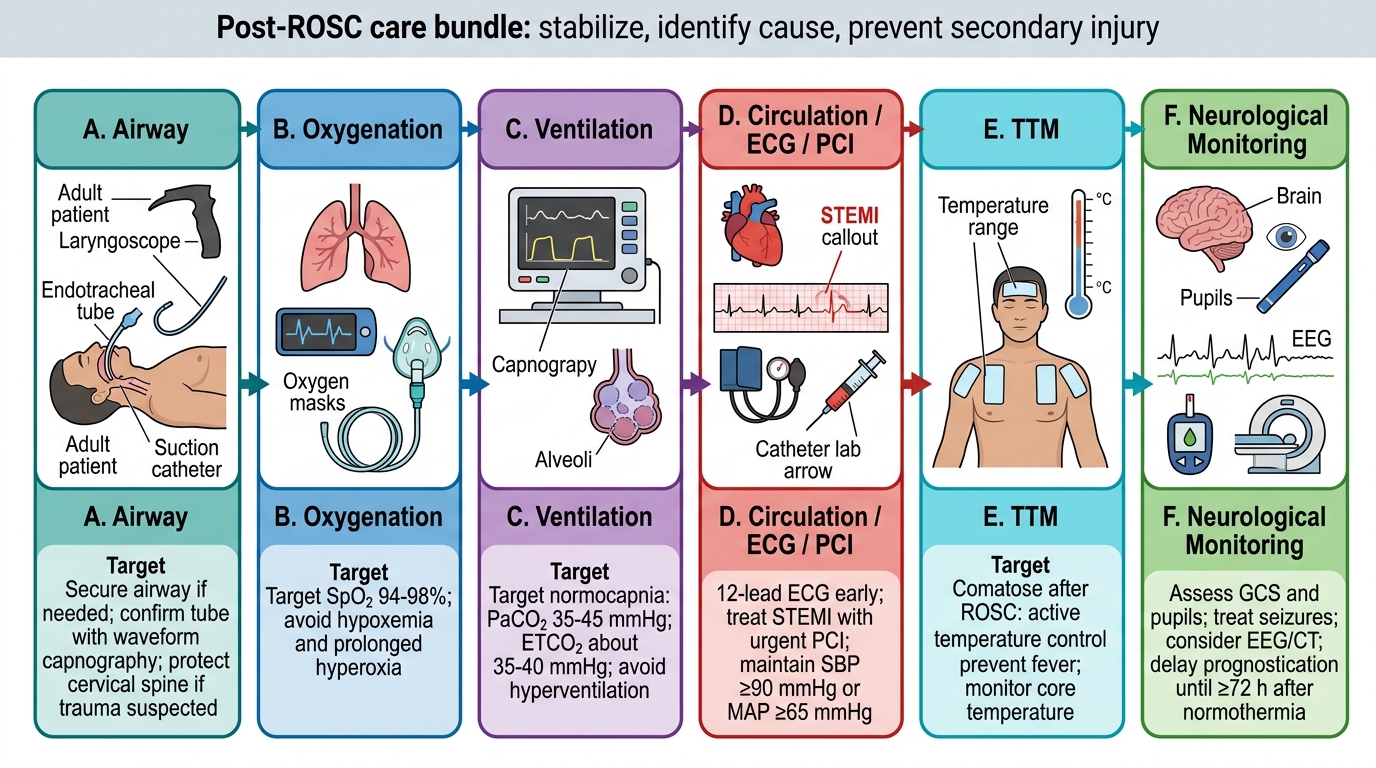
Post-ROSC Care Bundle