Page 3 of 9
AS2.1-2 | Basic and Advanced Life Support Across Age Groups — SDL Guide (Part 3)
Applied and Supervised Practice: Simulation Scenarios
The NMC mandate for AS2.1 and AS2.2 explicitly requires demonstration in a simulated environment. Simulation-based CPR training is the educational gold standard for resuscitation because it allows deliberate practice with real-time feedback without risk to patients, and has been shown to improve skill acquisition, retention, and real-world performance. During your supervised simulation sessions, you will be assessed against the following performance benchmarks derived from the Resuscitation Council guidelines.
For BLS, examiners will assess: recognition of cardiac arrest (response, airway check, breathing check) in under thirty seconds; correct landmark and hand placement; compression depth of 5–6 cm on a manikin feedback device; rate 100–120/min; full chest recoil; two adequate rescue breaths (visible chest rise on the manikin) with minimal pause; continuous 30:2 cycling without interruption. Common errors to practise against include: leaning on the chest (inhibiting recoil), incorrect positioning (lateral rather than directly above), inadequate depth (the commonest error among first-attempt trainees), and pausing compressions for breathing assessment rather than working in pairs.
For ALS, examiners will assess: application of pads and interpretation of rhythm in a simulated two-minute pause; selection of the correct energy (150–200 J biphasic for adults; 4 J/kg for paediatric); safe defibrillation practice (clear call — 'Stand clear', visual check of contacts, delivery of shock); immediate resumption of CPR post-shock without waiting for rhythm recheck; timely administration of adrenaline and amiodarone at the correct points in the algorithm; articulation of the 4Hs and 4Ts; and communication of team roles.
For paediatric scenarios, you must demonstrate the five initial rescue breaths before compressions, apply the 15:2 ratio when a second rescuer joins, and calculate weight-based drug doses (adrenaline 10 mcg/kg, amiodarone 5 mg/kg). For neonatal scenarios, you must demonstrate the neutral airway position, five sustained inflation breaths, and the 3:1 ratio with the two-thumb encircling technique.
Between formal simulation sessions, use every intubation list or ICU ward round as an opportunity to rehearse recognition, confirm your team's defibrillator location, and review the crash trolley. The AHA/ERC recommends retraining in BLS skills every twelve months and ALS skills every two years to counteract the known skill decay that occurs with disuse.
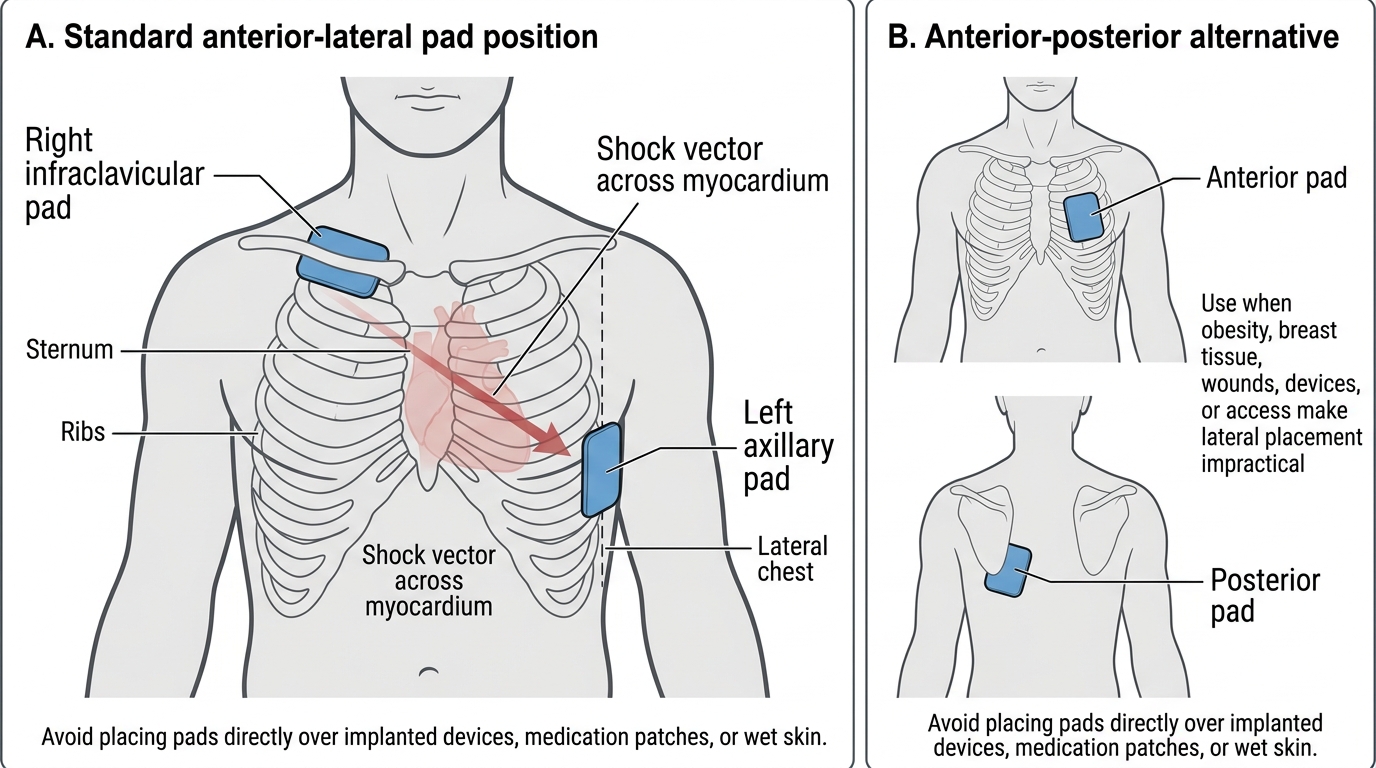
Adult Defibrillator Pad Placement
Self-Assessment: Checking Your Resuscitation Knowledge
Resuscitation competency requires both technical precision and confident recall under extreme pressure. Unlike most areas of clinical medicine where an approximate answer can be refined through consultation or a textbook, cardiac arrest leaves no margin for imprecision: a compression rate of eighty per minute reduces coronary perfusion substantially compared to one hundred, a defibrillation energy selected for a child instead of an adult can deliver a fatally high joule-per-kilogram dose, and a drug administered for asystole instead of VF wastes irreplaceable seconds. The self-assessment framework below is designed to test the numerical precision and procedural sequence that the NMC competency AS2.1 and AS2.2 demands. Resuscitation skills also decay more rapidly than most clinical knowledge without deliberate rehearsal — studies show significant degradation in compression quality within three to six months of training. Work through each prompt without referring to the text above; only then confirm your answers against the reference values. Gaps in your recall at this stage should direct a targeted re-read of the specific section, followed by a second attempt without notes. Aim for zero hesitation on every numerical value before your simulation session.
Technical precision checks — answer without looking:
- Adult compression rate: __/min (answer: 100–120/min)
- Adult compression depth: __ cm (answer: 5–6 cm)
- Adult BLS ratio: __ (answer: 30:2)
- Paediatric BLS ratio with two healthcare rescuers: __ (answer: 15:2)
- Neonatal compression:ventilation ratio: __ (answer: 3:1)
- First defibrillation energy in an adult (biphasic): __ J (answer: 150–200 J)
- Defibrillation energy in a child: __ J/kg (answer: 4 J/kg)
- Shockable rhythms (name both): __ (answer: VF and pulseless VT)
- Adrenaline dose in adult ALS (first dose, when given): 1 mg IV, after third shock in shockable; immediately in non-shockable
- Adrenaline dose in paediatric ALS: __ mcg/kg (answer: 10 mcg/kg)
- Amiodarone dose in adult ALS (first dose): __ mg IV, given after __ shock (answer: 300 mg, third shock)
Scenario prompt — talk through aloud:
A 7-year-old collapses in the outpatient waiting area. You find the child unresponsive and not breathing. Describe your complete response sequence (recognition → call for help → five breaths → 30 compressions or 15:2 with two rescuers → AED/rhythm check → drugs).
If you hesitated on any numerical value above, re-read the relevant section. Competence in resuscitation depends on instant, accurate recall — approximations cost lives in the arrest room.
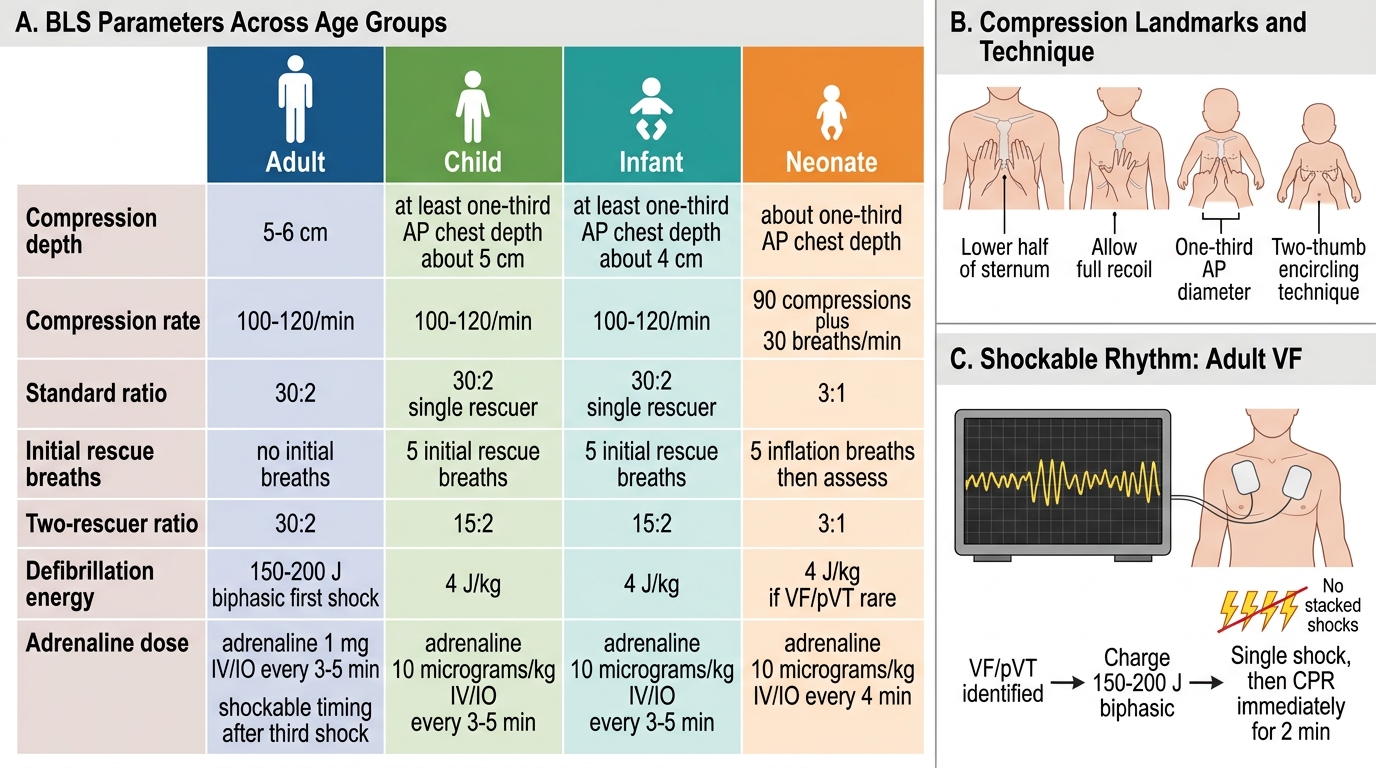
BLS Parameters Across Age Groups
SELF-CHECK
A 58-year-old man in the pre-operative assessment clinic collapses. You confirm cardiac arrest and attach the defibrillator — it shows a rapid, irregular broad-complex rhythm with no discernible QRS morphology. After immediately resuming CPR, what is the correct next step?
A. Give adrenaline 1 mg IV immediately and continue CPR for 2 minutes
B. Charge the defibrillator to 150–200 J (biphasic) and deliver one shock, then resume CPR immediately
C. Deliver three stacked shocks in quick succession before resuming CPR
D. Continue CPR for 2 minutes before the first rhythm check and shock
Reveal Answer
Answer: B. Charge the defibrillator to 150–200 J (biphasic) and deliver one shock, then resume CPR immediately
The rhythm described — rapid, chaotic, broad-complex with no recognisable QRS — is ventricular fibrillation (VF), a shockable rhythm. Current ALS guidelines (Resuscitation Council UK / ERC) specify one shock (150–200 J biphasic for adults) followed by immediate resumption of 2 minutes of CPR without waiting to assess the rhythm post-shock. Option A describes the correct adrenaline timing for non-shockable rhythms (asystole/PEA). Option C (stacked shocks) was abandoned after biphasic defibrillators were introduced; the energy wasted on stacked shocks delays return to CPR. Option D delays the first shock, reducing the probability of successful defibrillation.
SELF-CHECK
During resuscitation of a 6-year-old, a second healthcare provider joins you. The child's primary rhythm is asystole. Which compression:ventilation ratio should you now use?
A. 30:2 — the same as adult BLS
B. 15:2 — two-rescuer paediatric CPR ratio
C. 3:1 — neonatal ratio applied to all children
D. Asynchronous compressions at 100/min with ventilation at 10/min
Reveal Answer
Answer: B. 15:2 — two-rescuer paediatric CPR ratio
With two healthcare providers performing paediatric CPR, the ratio is 15:2, not 30:2. The paediatric guideline uses a higher ventilation proportion (15:2 vs 30:2) to address the predominant asphyxial mechanism of arrest in children. A lone rescuer reverts to 30:2 for practicality. The 3:1 ratio applies exclusively to neonates at birth. Asynchronous ventilation is used only after an advanced airway is secured in intubated patients.
CLINICAL PEARL
Agonal breathing will kill your patient if you mistake it for normal breathing. Agonal respirations — irregular, noisy, laboured gasps — can persist for minutes after cardiac arrest and look deceptively like effortful breathing. The key differentiator is regularity and adequacy: normal breathing is regular, effortless, and moves sufficient air. Any doubt should be resolved in favour of treating as cardiac arrest: starting CPR on a patient who is not in arrest carries negligible risk; failing to start CPR on a patient who is in arrest is fatal. Train yourself to spend no more than ten seconds on the breathing check and to default to starting CPR if you are unsure.