Page 7 of 20
AS4.2 | Airway Anatomy Relevant to General Anaesthesia — SDL Guide (Part 3)
Paediatric Airway Anatomy and Differences from Adults
The paediatric airway differs from the adult airway in several anatomically important ways that directly influence anaesthetic technique, equipment selection, and the management of intraoperative complications. These differences are not trivial variations — in some cases they represent complete reversals of the adult paradigm, and failure to account for them is a common source of preventable paediatric anaesthesia mishaps. The most consequential differences relate to the size and position of the larynx, the shape and consistency of the epiglottis, the narrowest fixed point of the airway, the length of the trachea, and the physiological reserve for apnoea. A clinician who understands these differences will instinctively select the appropriate laryngoscope blade, choose the correct tube size, position the patient correctly, and respond rapidly to the far faster desaturation that characterises paediatric airway emergencies.
Key anatomical differences in children:
- Larger head relative to body: neonates have a proportionally large occiput, which naturally flexes the neck when supine; this means the sniffing position may be achieved without a head pillow, or even with a shoulder roll to avoid excess neck flexion
- Tongue is proportionally larger and the larynx is higher (C3–C4 level in neonates vs C5–C6 in adults) and more anteriorly positioned — making the laryngoscopic view more difficult; an anterior view of the glottis is the rule in infants
- Epiglottis is longer, stiffer (omega-shaped), and angled more posteriorly — the Miller (straight) blade is often preferred in neonates and young infants because it can directly lift the floppy, omega-shaped epiglottis more effectively than the curved Macintosh
- Narrowest point is the subglottis (cricoid ring), not the glottis — in children under approximately 8–10 years, the cricoid is the most restrictive point; uncuffed tubes were traditionally used to avoid subglottic mucosal trauma from cuff pressure; modern microcuff tubes with very low-pressure cuffs positioned below the cords are now widely used in paediatric anaesthesia
- Short trachea (only 4 cm in a neonate) — right main bronchus intubation occurs with very small tube displacements; vigilance for unilateral chest movement and bilateral auscultation is mandatory
- Higher oxygen consumption per kg and smaller functional residual capacity — desaturation occurs far more rapidly during apnoea in infants and children than in adults
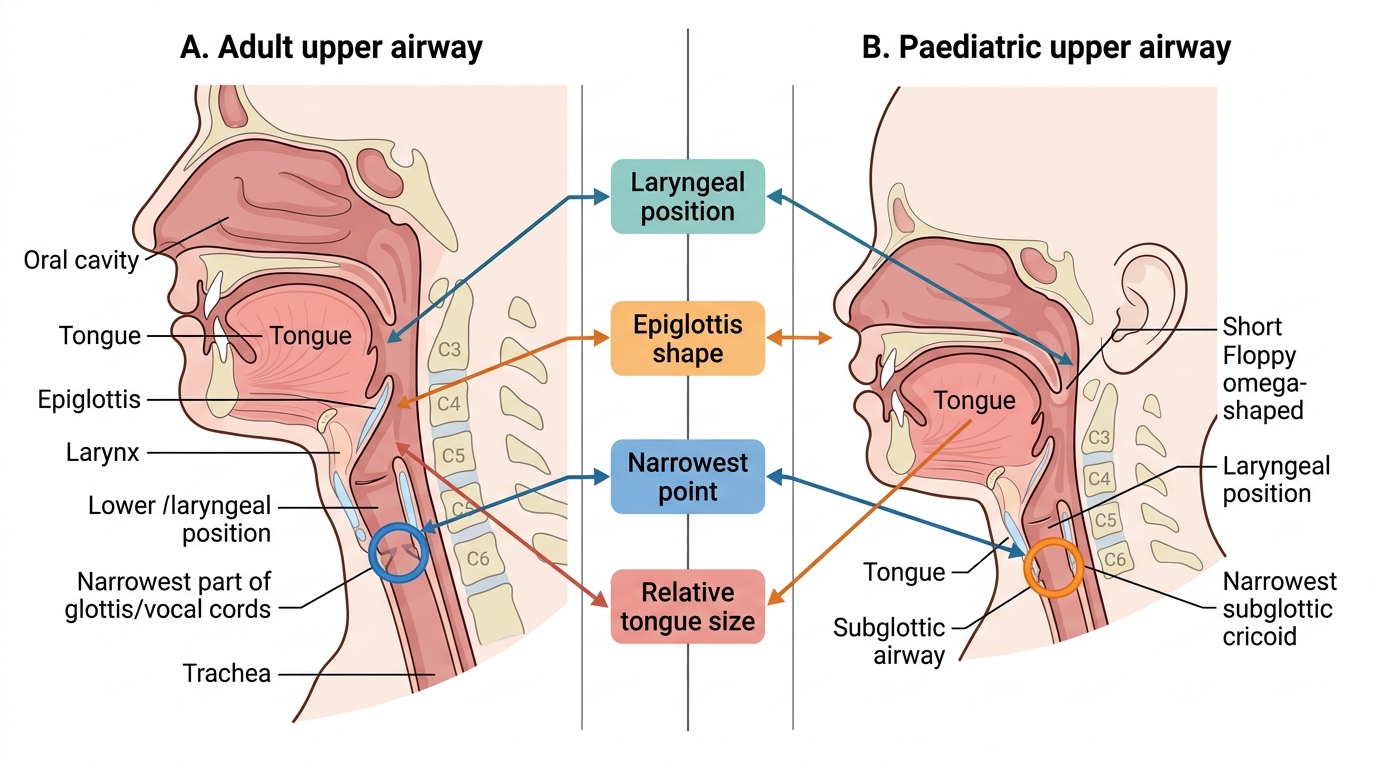
Adult vs Paediatric Upper Airway Anatomy
Clinical and Applied Significance: Predicting and Managing the Difficult Airway
Knowledge of airway anatomy underlies every component of difficult airway prediction and management. A difficult airway is defined as one in which a conventionally trained anaesthesiologist experiences difficulty with mask ventilation, supraglottic airway placement, laryngoscopy, intubation, or tracheostomy. Since death from failed airway management is catastrophic and preventable, every anaesthetic begins with a structured preoperative airway assessment using anatomical criteria. This assessment does not merely predict difficulty in the abstract — it directly determines the anaesthesiologist's choice of technique (awake versus asleep intubation), device (direct laryngoscopy versus video laryngoscopy versus fibreoptic bronchoscope), plan (primary, first backup, second backup, and rescue), and staffing (whether senior assistance and a surgeon for surgical airway must be present at induction). No single anatomical predictor is perfectly sensitive or specific; airway prediction relies on combining multiple factors into an overall risk assessment, with the decision rule being: when doubt exists, treat as difficult and plan accordingly.
The standard airway assessment examines:
1. Mouth opening (inter-incisor distance): <3 cm = restricted laryngoscope blade insertion
2. Mallampati class (I–IV): Class III–IV predicts reduced laryngoscopic view
3. Thyromental distance (chin to thyroid notch, head extended): <6 cm indicates an anterior larynx (difficult to visualise)
4. Neck mobility: full atlanto-occipital extension required for sniffing position alignment
5. Neck anatomy: short muscular neck, obesity, previous neck surgery or radiation, large thyroid goitre — all reduce access and visualise-ability
6. Dentition: prominent upper incisors (prognathic upper jaw), loose or capped teeth
7. Sternomental distance: <12.5 cm associated with difficult laryngoscopy
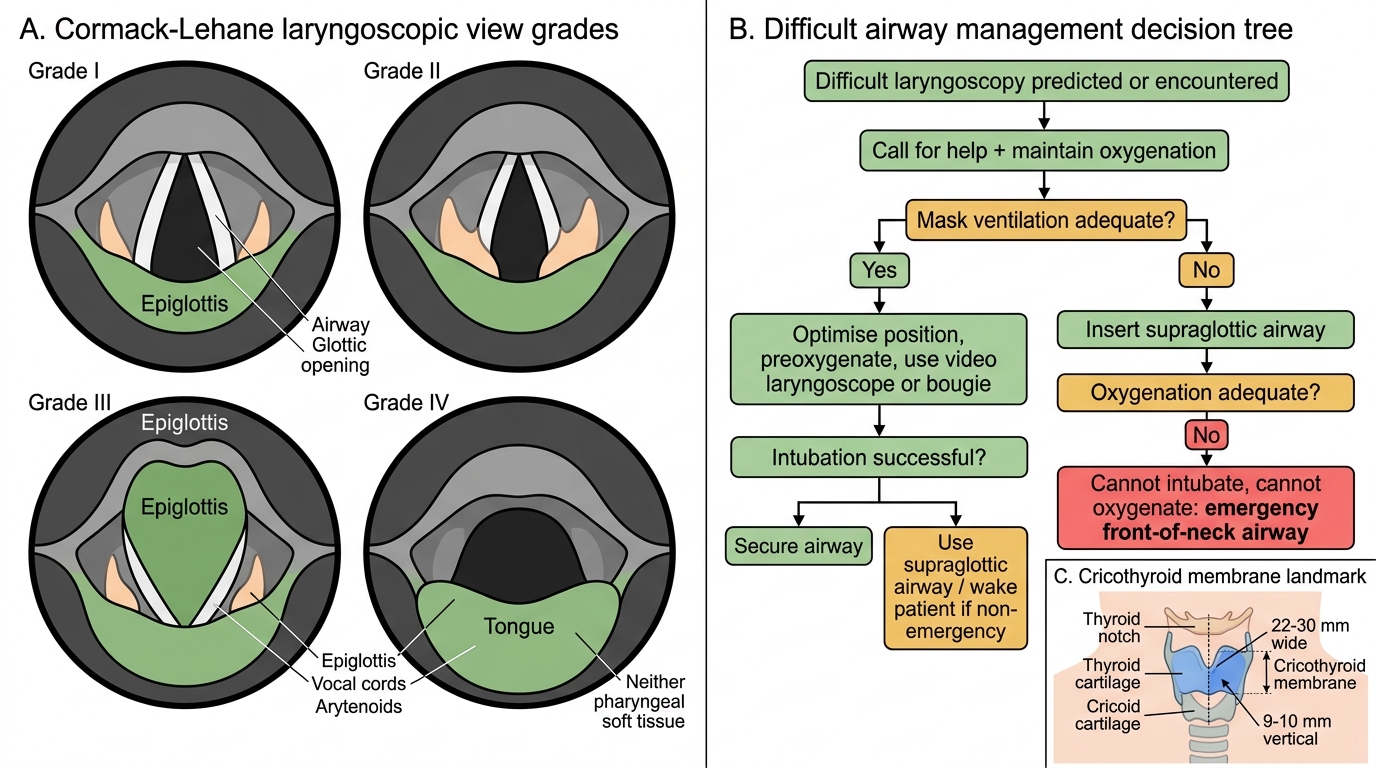
The Cormack–Lehane grading system describes the laryngoscopic view:
- Grade I: entire glottis visible
- Grade II: only posterior commissure (arytenoids) visible
- Grade III: only epiglottis visible (no glottic structures)
- Grade IV: neither epiglottis nor glottis visible
Grade III–IV views predict difficult or failed intubation with direct laryngoscopy. For such patients, strategies include: video laryngoscopy (provides an improved view of an anterior larynx), fibreoptic bronchoscope-guided intubation (especially for awake procedures in patients with predicted severe difficulty), supraglottic airways (LMA, i-gel) as rescue devices for ventilation, and surgical airway (needle or surgical cricothyrotomy through the cricothyroid membrane) in cannot-intubate-cannot-oxygenate emergencies.
Cormack-Lehane Grades and Difficult Airway Pathway
The anatomical landmark for emergency cricothyrotomy — the cricothyroid membrane — must be identifiable by palpation even in obese or anatomically aberrant necks. It lies in the midline, approximately 2–3 cm below the thyroid notch, between the lower border of the thyroid cartilage superiorly and the upper border of the cricoid arch inferiorly. Its average dimensions are 22–30 mm wide by 9–10 mm vertically. A vertical skin incision followed by a horizontal incision through the membrane (Seldinger or scalpel-finger-bougie technique) provides the fastest surgical airway — the only lifesaving option when all other airway interventions have failed.
SELF-CHECK
During preoperative airway assessment of a 52-year-old male, you note a Mallampati Class III view, thyromental distance of 5 cm, and limited neck extension. What is the clinical significance of these findings, and how does the thyromental distance relate to airway anatomy?
A. These findings indicate severe systemic disease (ASA Class III) and predict a high anaesthetic risk unrelated to intubation
B. These findings predict a potentially difficult laryngoscopy; a short thyromental distance indicates an anteriorly placed larynx, making glottic visualisation harder by direct laryngoscopy
C. A Mallampati Class III view is reassuring; combined with limited neck extension, it predicts only mild difficulty with mask ventilation
D. The thyromental distance is a measure of tongue size — a short distance means a small tongue and easy intubation
Reveal Answer
Answer: B. These findings predict a potentially difficult laryngoscopy; a short thyromental distance indicates an anteriorly placed larynx, making glottic visualisation harder by direct laryngoscopy
The combination of Mallampati Class III (limited oropharyngeal view), thyromental distance <6 cm (indicating an anteriorly placed larynx — the glottis is far anterior relative to the mouth, shortening the distance between mandible and larynx), and limited neck extension (impairs sniffing position alignment of the three axes) together strongly predict a potentially difficult direct laryngoscopy. A full preoperative plan including backup devices (video laryngoscope, fibreoptic bronchoscope, supraglottic airway) should be prepared. Option A confuses Mallampati with ASA classification — these are entirely different scales. Option C incorrectly reassures. Option D misunderstands the anatomical meaning of thyromental distance.
Self-Assessment: Airway Anatomy in Clinical Context
To consolidate your understanding of airway anatomy, attempt the following self-check exercises that link anatomical knowledge to clinical reasoning — the level expected in AS4.2.
First, trace the route of an endotracheal tube from the lips to the carina, naming every structure it passes through or alongside in sequence. For each structure, state one clinically relevant fact: why does it matter in anaesthesia? Specifically — what happens at the level of the epiglottis during normal swallowing, and what does this imply about aspiration risk under general anaesthesia?
Second, a patient cannot be intubated using a standard Macintosh blade (Grade III Cormack-Lehane view). Describe what 'Grade III' means anatomically — which structures are visible and which are hidden? Why does a short thyromental distance cause an anterior larynx, and how does this anatomically produce a Grade III view? What alternative strategies would you consider, and which one allows the patient to breathe spontaneously while their airway is secured?
Third, explain why the subglottis (not the glottis) is the narrowest fixed point in a 2-year-old child's airway, and what clinical consequence follows from this when selecting an endotracheal tube size. What formula would you use to estimate appropriate tube size (internal diameter = [age/4] + 4 mm for uncuffed, [age/4] + 3.5 mm for cuffed)?
Finally, locate the cricothyroid membrane by palpation on your own neck (or a model): start at the thyroid notch, move inferiorly to the lower border of the thyroid cartilage — the space immediately below it (before the cricoid ring) is the cricothyroid membrane. Practise identifying it; in a cannot-intubate-cannot-oxygenate emergency, your ability to find this landmark rapidly is what saves the patient's life.
CLINICAL PEARL
Mallampati ≠ ASA: Two different scales, two different purposes. Mallampati (I–IV) grades the oropharyngeal view as a predictor of laryngoscopic difficulty — a purely anatomical assessment performed at the bedside with the patient awake, mouth open, tongue protruded. ASA Physical Status (I–VI) grades the severity of systemic co-morbidity. A Mallampati IV patient may be ASA I (young healthy person with a small mouth and large tongue — physically fit but anatomically difficult to intubate). A Mallampati I patient may be ASA IV (excellent airway anatomy in a patient with severe cardiac failure). Confusing these scales in documentation, examination answers, or clinical handover is a serious error.