Page 6 of 20
AS4.2 | Airway Anatomy Relevant to General Anaesthesia — SDL Guide (Part 2)
Hypopharynx, Epiglottis, and the Laryngopharynx
Below the oropharynx, the airway passes into the hypopharynx (laryngopharynx), which lies posterior to the larynx. Two anatomical recesses here — the piriform fossae (one on each side of the larynx, between the thyroid cartilage and the lateral wall of the hypopharynx) — are important in clinical practice: a laryngoscope blade that passes too laterally enters a piriform fossa rather than lifting the epiglottis; and airway foreign bodies frequently lodge here. The piriform fossae also contain branches of the internal laryngeal nerve — a landmark exploited during nerve block techniques for awake intubation.
The epiglottis is a leaf-shaped elastic cartilage attached at its base to the inner surface of the thyroid cartilage (via the thyroepiglottic ligament) and connected to the base of the tongue (via the median and lateral glossoepiglottic folds). The space between the base of the tongue and the epiglottis — the vallecula — is the critical landmark in direct laryngoscopy: a curved (Macintosh) laryngoscope blade is positioned in the vallecula and then lifted anteriorly (in the direction of the blade handle, i.e., at 45° upward and forward — NOT levered backward over the upper teeth) to indirectly elevate the epiglottis and expose the glottic opening. A straight (Miller) blade, by contrast, is passed posterior to the epiglottis and directly lifts it.
The epiglottis functions as a biological valve — during swallowing it deflects posteriorly to cover the glottic inlet, directing food into the oesophagus. Under anaesthesia, this reflex is obtunded, which is why laryngeal protection against aspiration is lost during general anaesthesia — the physiological basis for fasting requirements and the use of rapid-sequence induction in patients at aspiration risk.
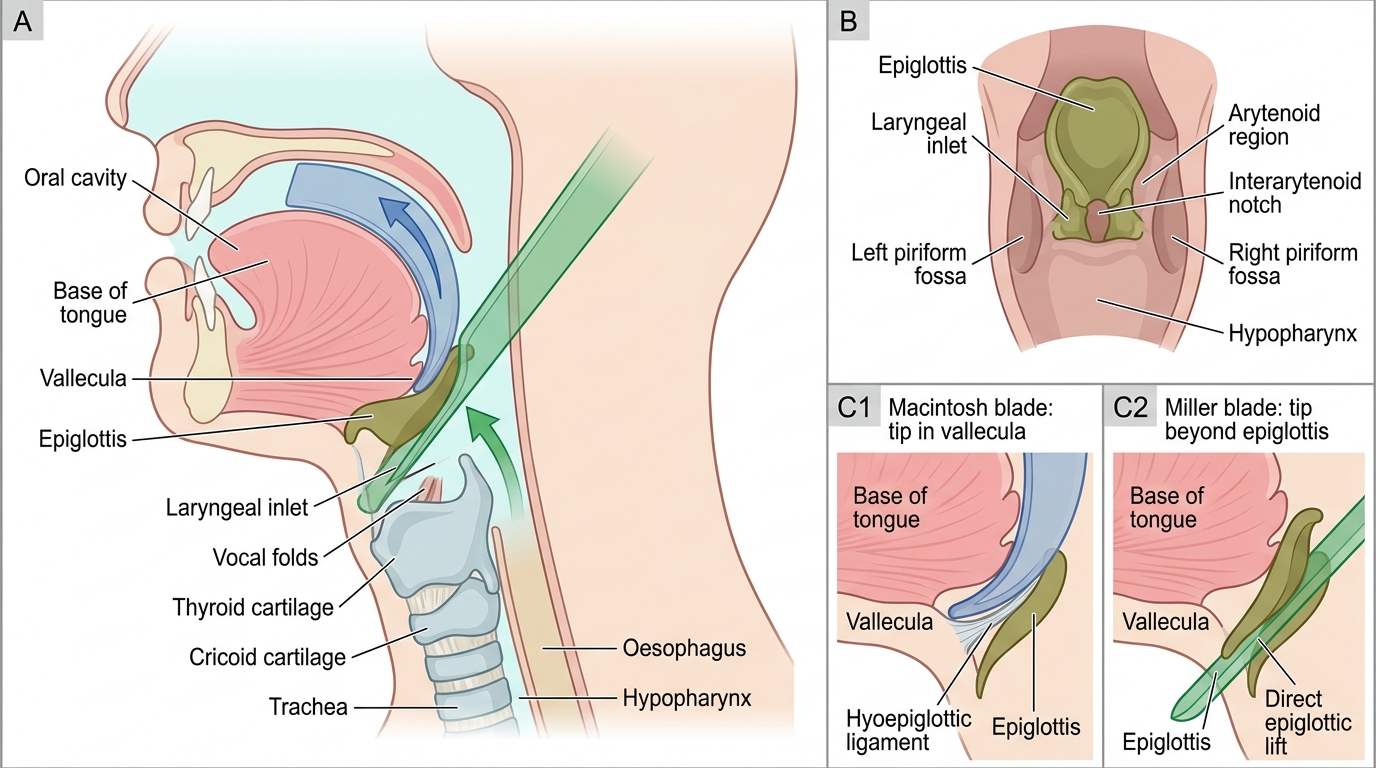
Laryngoscope Blade Trajectories at the Laryngeal Inlet
The Larynx: Cartilages, Vocal Folds, and Subglottis
The larynx is the critical gateway between the pharynx and the trachea. It serves three biological functions — phonation, airway protection during swallowing, and regulation of airflow — all of which are relevant to anaesthesia. The laryngeal skeleton consists of nine cartilages: three single (thyroid, cricoid, epiglottis) and three paired (arytenoids, cuneiform, corniculate).
The thyroid cartilage forms the anterior shield of the larynx (the 'Adam's apple' prominence, more pronounced in adult males). Its inner surface provides attachment for the vocal ligaments anteriorly. The cricoid cartilage is the only complete cartilaginous ring in the respiratory tract — it has a narrow anterior arch and a broad posterior signet ring-shaped lamina. This structural completeness makes the cricoid the only structure capable of transmitting posterior pressure to occlude the oesophagus (the anatomical basis of Sellick's manoeuvre — cricoid pressure during RSI to reduce aspiration risk). The cricothyroid membrane spans the gap between the inferior border of the thyroid cartilage and the superior border of the cricoid arch — midline, covered by skin with minimal soft tissue overlay in most patients. It is the preferred site for emergency surgical airway (needle cricothyrotomy or surgical cricothyrotomy) precisely because it is the most accessible point of the lower airway from outside.
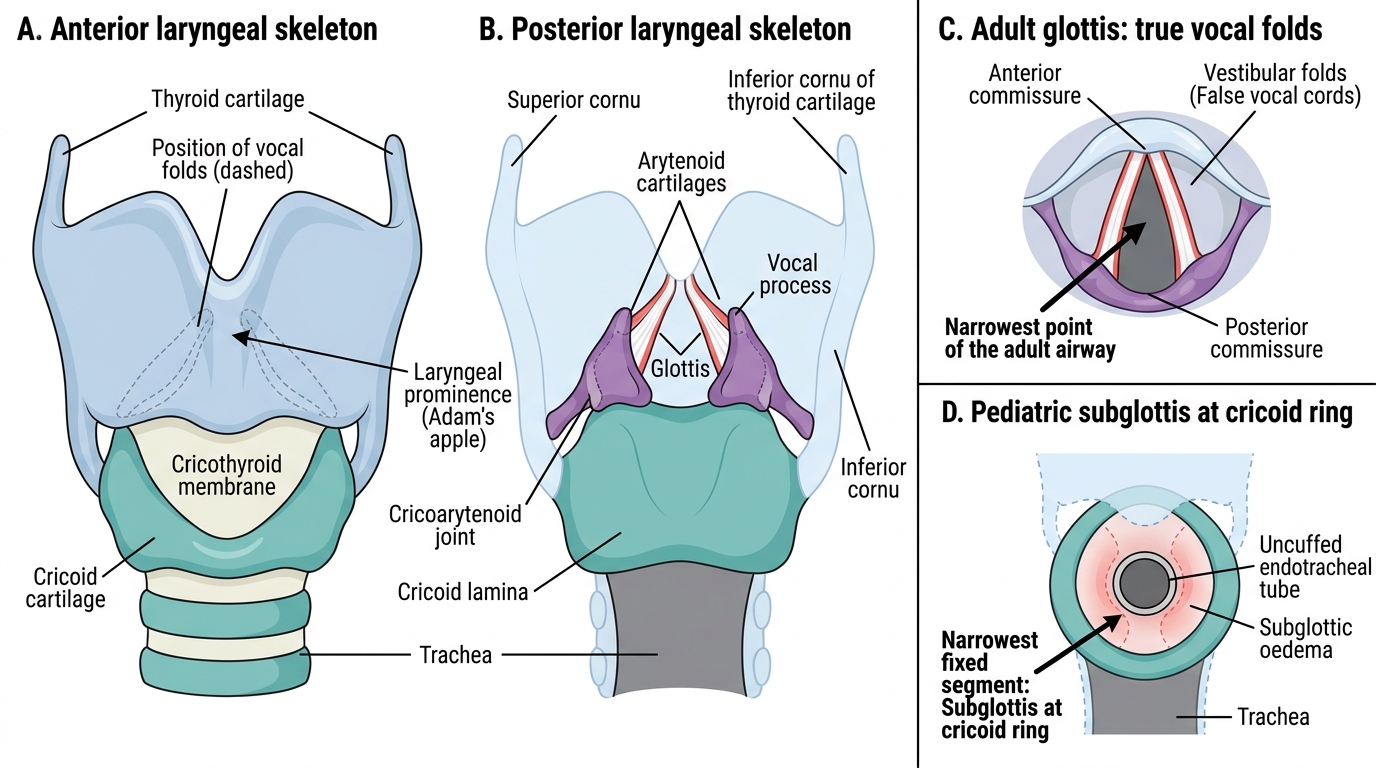
Laryngeal Cartilage Skeleton and Vocal Fold Position
The vocal folds (true cords) are the narrowest point of the adult airway at the level of the glottis. They are formed by the vocal ligament (stretched between the vocal process of the arytenoid posteriorly and the inner angle of the thyroid cartilage anteriorly) covered by stratified squamous epithelium. In the adult, the glottic opening measures approximately 23 × 17 mm at its widest (during full abduction). The space immediately inferior to the true cords — the subglottis — is the narrowest fixed segment of the pediatric airway (in children, the subglottis at the level of the cricoid ring is the narrowest point, not the glottis, because the cricoid is a complete ring that cannot expand). This is why uncuffed endotracheal tubes are used in young children — a tube that fits the subglottis snugly without a cuff provides an appropriate seal. Subglottic oedema (post-intubation croup) develops in this inelastic space, causing proportionally greater airway narrowing in children than in adults.
The arytenoid cartilages sit on the posterosuperior surface of the cricoid lamina. They are pyramid-shaped and their vocal processes provide the posterior attachment for the vocal ligaments. During laryngoscopy, the arytenoids appear as two rounded posterior prominences ('arytenoid knobs') and are the first structures identified in establishing the posterior boundary of the glottis. The inter-arytenoid notch between them, and the posterior commissure, are landmarks for assessing the posterior component of the Cormack-Lehane laryngoscopic view.
The Trachea and Three-Axis Alignment for Intubation
The trachea begins at the lower border of the cricoid cartilage (C6 vertebral level) and extends approximately 10–12 cm to the carina at the level of the sternal angle (T4–T5). It is composed of 16–20 C-shaped cartilaginous rings (open posteriorly), united by the trachealis muscle — the posterior membranous wall — which abuts the oesophagus. The trachea is not rigid: it is compressed from behind by the oesophagus (distended by a nasogastric tube or food), and its compliance can be altered by external masses (goitre, mediastinal tumours) or intrinsic pathology (tracheomalacia). These considerations are critically important during anaesthetic planning for patients with mediastinal masses — the risk of airway collapse on induction of anaesthesia must be weighed before muscle relaxants are given.
A standard 7.0–7.5 mm internal-diameter endotracheal tube is appropriate for most adult women; 8.0–8.5 mm for adult men. The tube must be advanced beyond the vocal folds to a position where the cuff sits in the subglottic/upper tracheal region, and the tip must be at least 3–4 cm above the carina (to prevent right main bronchus intubation, the right mainstem bronchus being less acutely angled than the left). Clinical confirmation of tracheal tube position includes: auscultation of bilateral breath sounds, waveform capnography (gold standard — sustained end-tidal CO₂ waveform confirms tracheal position; absence indicates oesophageal intubation), direct visualisation through the cords, chest X-ray, and fibreoptic confirmation when indicated.
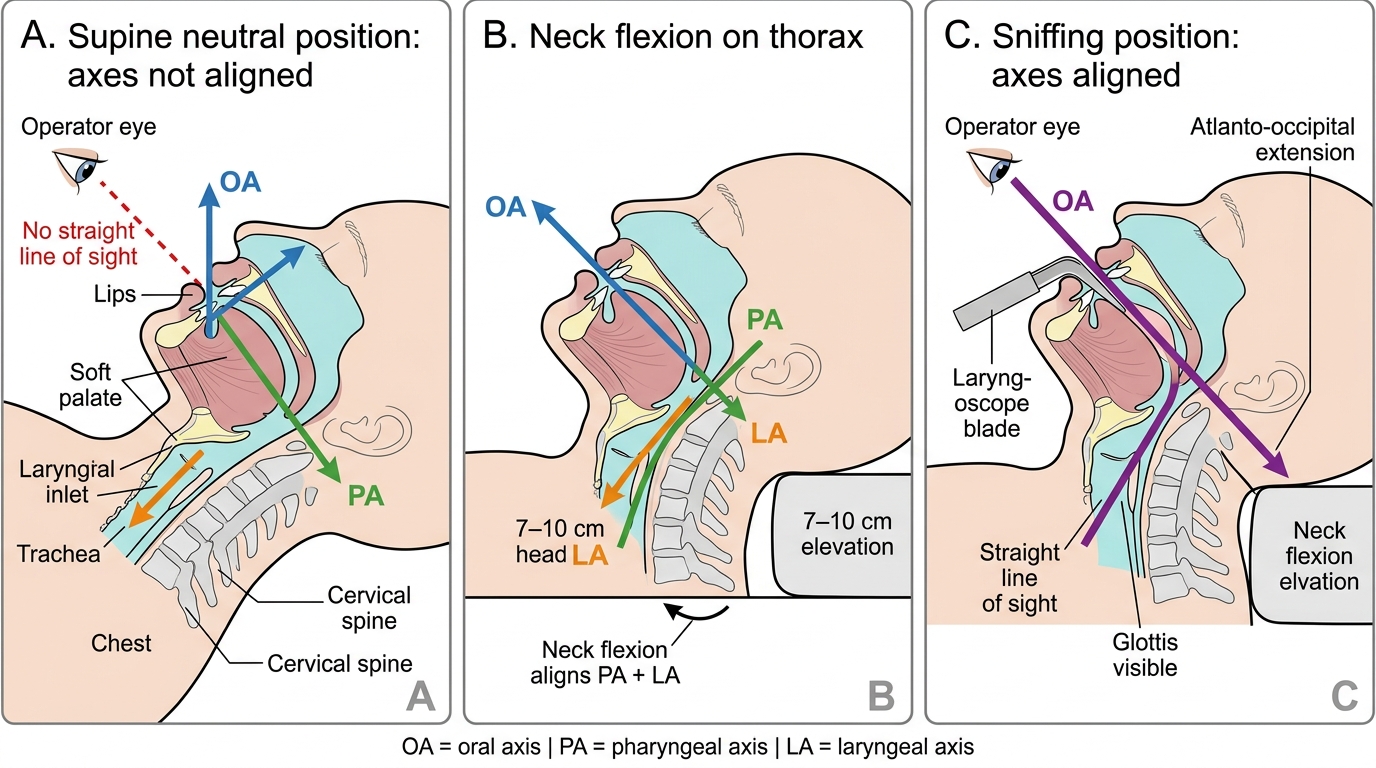
Three-Axis Alignment in the Sniffing Position
Three-axis alignment is fundamental to understanding why patient positioning matters for intubation. Direct laryngoscopy requires a straight line of sight from the operator's eye through the oral opening, past the tongue, through the oropharynx, past the epiglottis, to the glottis. Three axes exist:
- Oral axis (OA): the direction of the oral opening, perpendicular to the face (vertical when supine)
- Pharyngeal axis (PA): directed posteroinferiorly from the pharynx toward the larynx
- Laryngeal axis (LA): the long axis of the trachea, directed anteroinferiorly
These three axes must be aligned ('superimposed') into a single straight line for direct laryngoscopy. The sniffing position — neck flexion on the thorax (pillow under head, approximately 7–10 cm) combined with atlantoaxial extension (head extended at the atlanto-occipital joint) — achieves this alignment by: (1) flexion aligns the PA and LA, and (2) extension aligns the OA with the combined PA-LA axis. Without adequate positioning, even a skilled laryngoscopist cannot achieve a satisfactory laryngoscopic view.