Page 9 of 20
AS4.3-5 | Induction, Maintenance, Monitoring and Vital Organ Support During Anaesthesia — SDL Guide
CLINICAL SCENARIO
Watch any anaesthesiologist at the start of a case and you witness a precisely choreographed sequence: monitors applied, drugs drawn up in labelled syringes, oxygen running, suction checked, laryngoscope tested, drugs given in a specific order, the patient's airway secured, the ventilator set, and then — for the next two hours — continuous interpretation of waveforms, alarms, vital signs, and surgical feedback, all while adjusting the anaesthetic depth in real time. This is the conduct of general anaesthesia. Every step has a reason rooted in physiology and pharmacology, and every deviation from normal monitoring data demands a differential diagnosis and an immediate response. This SDL maps the clinical procedure from first monitor to final reversal.
WHY THIS MATTERS
AS4.3 requires you to observe and describe the principles and practical aspects of induction and maintenance of anaesthesia. AS4.4 covers maintenance of vital organ functions in patients undergoing surgery. AS4.5 covers monitoring principles and techniques during anaesthesia. Together these three competencies form the procedural core of general anaesthesia — the applied translation of the pharmacology and anatomy covered in the preceding SDLs. Understanding this sequence is essential not just for anaesthesia rotations but for any clinical setting where you must recognise and respond to a deteriorating patient under sedation or general anaesthesia: the ICU, the endoscopy suite, and the emergency department all share the same fundamental monitoring and vital-organ-support principles.
RECALL
Recall the following before proceeding: (1) induction agents and their doses — propofol 1.5–2.5 mg/kg, thiopentone 3–5 mg/kg, ketamine 1–2 mg/kg IV, etomidate 0.2–0.3 mg/kg; (2) suxamethonium 1–1.5 mg/kg for rapid-sequence induction; (3) the three-axis alignment and sniffing position for laryngoscopy; (4) ASA fasting guidelines — clear fluids 2 h, breast milk 4 h, light meal 6 h, full meal 8 h; (5) end-tidal CO₂ capnography as the gold standard for confirming tracheal tube placement; (6) the concept of balanced anaesthesia — multiple agents at lower individual doses for all four anaesthetic components.
Clinical Indication and Preparation for General Anaesthesia
General anaesthesia (GA) is indicated whenever a surgical or diagnostic procedure requires the patient to be completely unconscious, free of pain and movement, with the airway under controlled management. The specific indications include: procedures too long or painful for sedation/regional anaesthesia alone; patients unable to cooperate with regional techniques; failed regional anaesthesia; procedures requiring controlled ventilation (intrathoracic or upper abdominal surgery, neurosurgery); and patient preference when regional anaesthesia is technically feasible. Understanding when GA is the appropriate choice — versus regional anaesthesia, neuraxial block, or monitored anaesthesia care — is itself a clinical decision requiring knowledge of the procedure, patient physiology, and available resources.
Preoperative preparation is systematic. The anaesthesiologist completes a structured pre-anaesthetic assessment: review of past medical history, prior anaesthetic records (looking for difficult airway history, adverse drug reactions, family history of malignant hyperthermia), current medications (anticoagulants, antihypertensives, insulin), allergies, and fasting status. Relevant investigations are reviewed — haemoglobin, coagulation, renal/hepatic function, ECG, echocardiogram in patients with cardiac disease. ASA physical status (I–VI) is assigned: it grades the severity of systemic co-morbidity and guides risk communication. An ASA I patient is completely healthy; ASA II has mild controlled systemic disease; ASA III has severe systemic disease; ASA IV has severe life-threatening disease; ASA V is moribund and not expected to survive 24 hours without surgery; ASA VI is brain-dead for organ donation. The 'E' suffix denotes an emergency procedure. ASA physical status grades systemic disease severity — it does not directly grade operative difficulty or airway status.
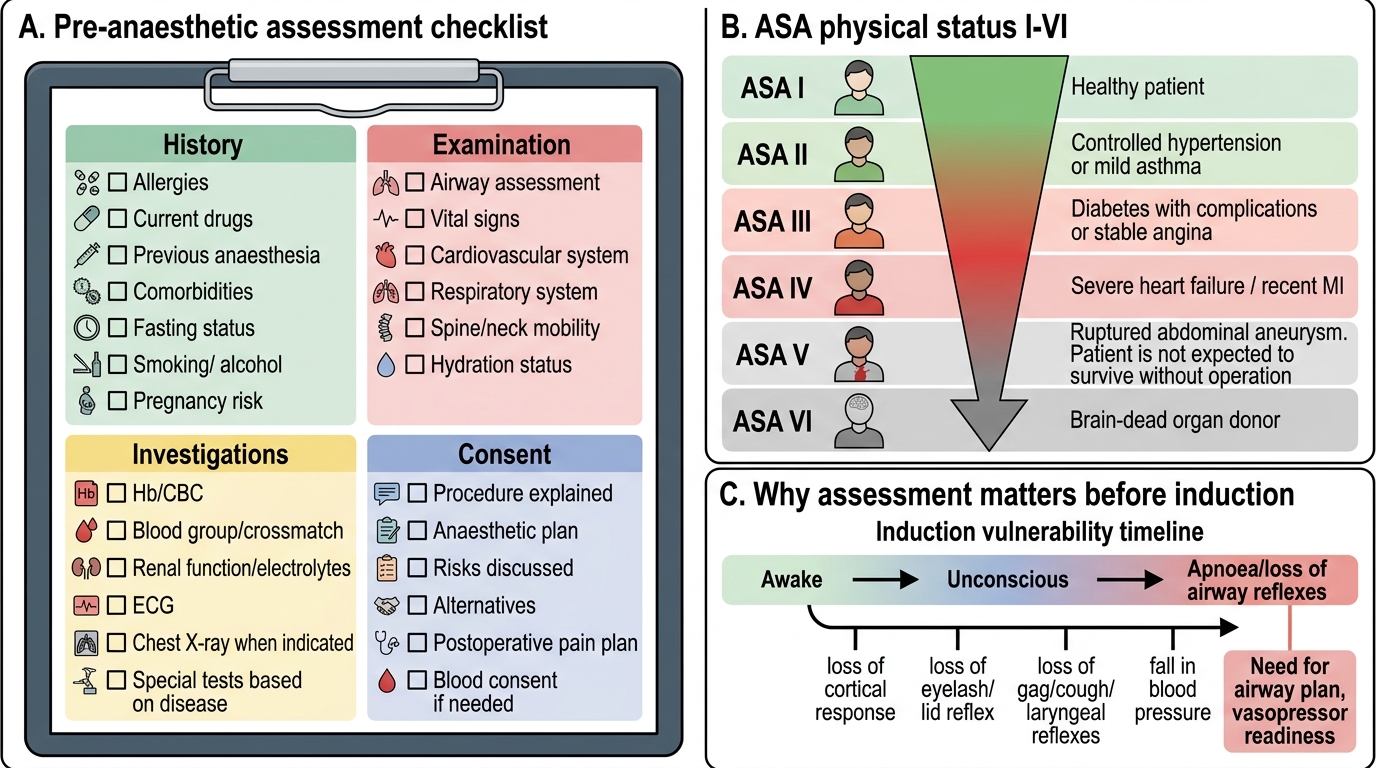
Pre-anaesthetic Assessment and ASA Classification
Anatomy and Governing Principles of Induction
The induction of general anaesthesia is a period of maximum physiological vulnerability. As the patient transitions from consciousness to unconsciousness, protective airway reflexes are lost in a predictable sequence: first, higher cortical functions are suppressed (consciousness, purposeful response), then sub-cortical reflexes (eyelash reflex, lid reflex), and finally brainstem reflexes (gag, cough, laryngeal protective reflexes). The anaesthetic depth at which laryngeal protective reflexes are lost varies with the agent — this determines the 'window' between loss of consciousness and loss of laryngeal reflex, which has direct implications for timing of laryngoscopy.
The governing physiological principles of induction are: (1) Speed of onset is determined by cerebral blood flow and drug lipid solubility — propofol reaches the brain within one arm-brain circulation time (~30 seconds); (2) Cardiovascular depression accompanies induction with most agents — a fall in systemic vascular resistance (propofol) and/or myocardial contractility (thiopentone) causes blood pressure to fall; the anaesthesiologist anticipates this and has vasopressors (ephedrine, phenylephrine) drawn and ready; (3) Apnoea invariably accompanies adequate induction — the anaesthesiologist must be prepared to ventilate the patient by mask the moment spontaneous breathing ceases; (4) Airway obstruction frequently occurs at induction as pharyngeal muscle tone is lost — relieved by jaw thrust, oropharyngeal airway, or laryngeal mask airway.
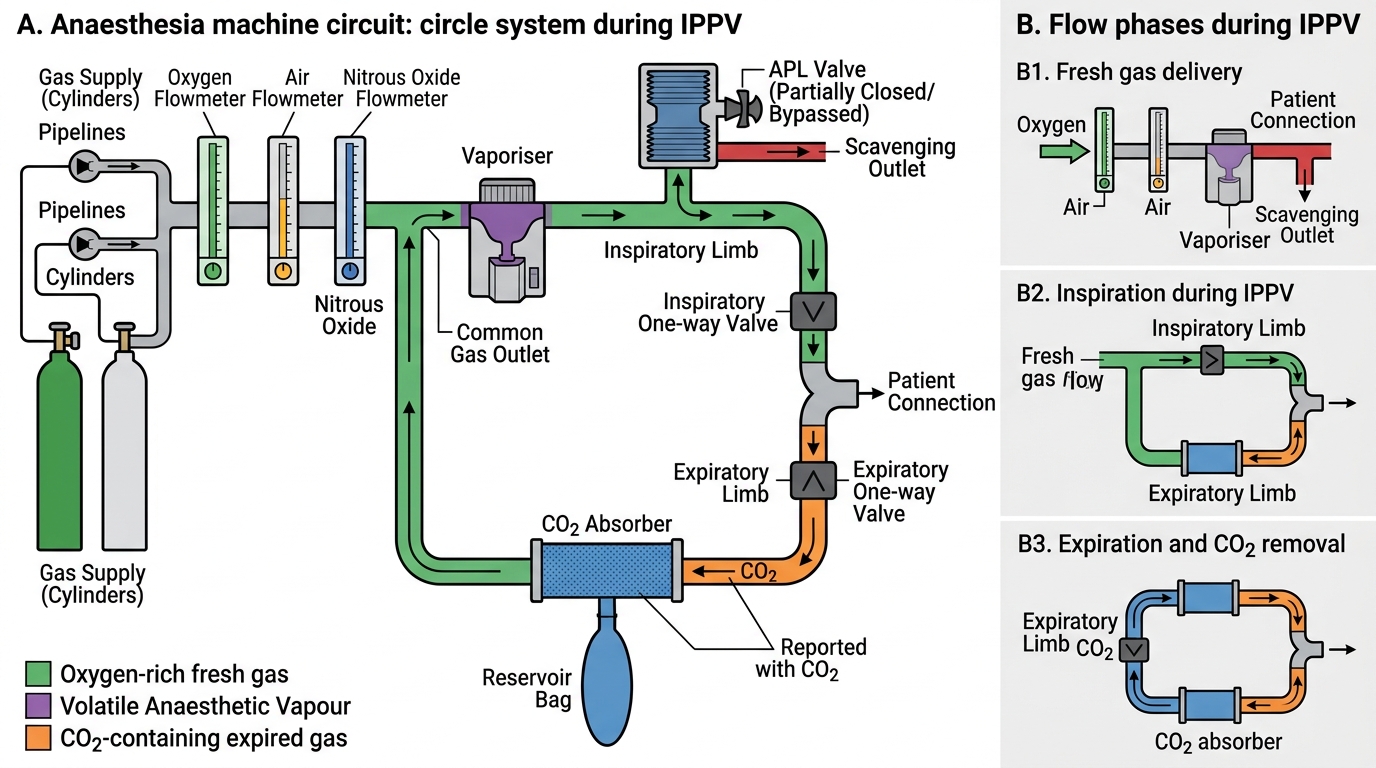
Anaesthesia Machine Circle Circuit During IPPV
Step-by-Step Induction Technique
A standard intravenous induction of general anaesthesia for an elective adult patient follows a defined sequence. Each step has a specific rationale; deviation from the sequence without a clinical reason is unsafe practice.
Step 1 — Pre-induction setup: IV access secured (at least one large-bore cannula; two if major surgery); monitoring applied (see 'Monitoring' section); anaesthetic machine checked (ABCDE: A=airway circuit, B=breathing circuit, C=cylinders, D=drugs, E=equipment including suction); emergency drugs drawn — ephedrine 3–6 mg/mL, atropine 0.6 mg, suxamethonium 200 mg; difficult airway equipment accessible (video laryngoscope, bougies, LMA sizes, surgical airway kit).
Step 2 — Preoxygenation: tight-fitting mask, 100% O₂, 3–5 minutes tidal breathing (or 4 deep breaths if time-critical). Denitrogenates the FRC, extending the safe apnoea window. A patient with an FRC of 2 L contains ~400 mL O₂ on room air; after preoxygenation, ~2 L O₂ — buying 3–5 additional minutes before desaturation.
Step 3 — Analgesic premedication: Fentanyl 1–2 mcg/kg IV, given ~3–5 minutes before induction agent. Blunts the pressor response to laryngoscopy; reduces induction agent requirement.
Step 4 — Induction agent: Propofol 1.5–2.5 mg/kg IV, titrated to effect (loss of verbal response + eyelash reflex). Or appropriate alternative per clinical context. Observe for apnoea and airway obstruction.
Step 5 — Mask ventilation: As the patient becomes apnoeic, establish bag-mask ventilation with 100% O₂. Confirm chest rise and ETCO₂ waveform. If obstruction: chin lift, jaw thrust, oral airway.
Step 6 — Muscle relaxant and intubation: Non-depolarising NMBA (rocuronium 0.6 mg/kg, vecuronium 0.1 mg/kg) or suxamethonium 1.5 mg/kg for RSI. Wait for adequate relaxation. Laryngoscopy — confirm Cormack-Lehane view, pass ETT through cords under direct vision, inflate cuff.
Step 7 — Confirm tube position: Capnography (sustained ETCO₂ waveform = tracheal position), bilateral auscultation, chest rise. Secure tube.
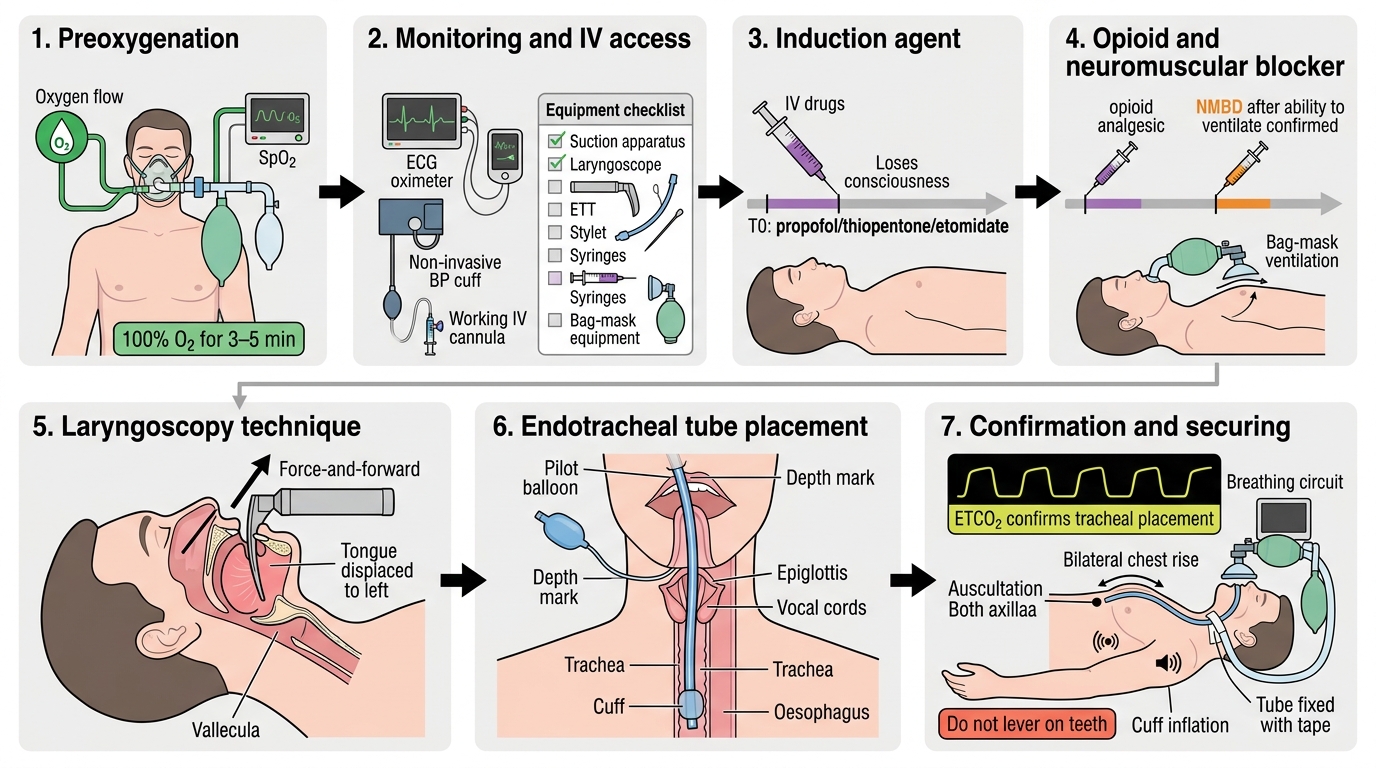
Steps of IV Induction and Endotracheal Intubation