Page 10 of 20
AS4.3-5 | Induction, Maintenance, Monitoring and Vital Organ Support During Anaesthesia — SDL Guide (Part 2)
Monitoring During Anaesthesia: Principles and Standards
Anaesthetic monitoring exists because general anaesthesia abolishes the patient's ability to communicate distress, suppresses normal physiological homeostatic responses, and introduces multiple pharmacological stressors simultaneously. The purpose of monitoring is not merely to detect problems — it is to enable the anaesthesiologist to anticipate and prevent physiological derangements before they cause harm. The standard of care for anaesthetic monitoring is defined by published guidelines (e.g., the World Federation of Societies of Anaesthesiologists minimum standards; the Indian Society of Anaestheologists guidelines); as a final-year medical student, you are expected to know the rationale for each modality, what it measures, its normal values, and the clinical significance of common abnormalities.
The minimum standard monitoring for every general anaesthetic includes five core modalities, remembered by the mnemonic CEOS+P — Capnography, ECG, Oxygen saturation (SpO₂), Sphygmomanometry (NIBP), and the Peripheral nerve stimulator (neuromuscular monitoring):
- Pulse oximetry (SpO₂): continuously displays oxygen saturation by measuring differential light absorption at 660 nm (deoxy-Hb) and 940 nm (oxy-Hb). Normal SpO₂ ≥95% (ideally ≥98% on supplemental O₂). Warning: pulse oximetry detects hypoxaemia — it does not detect hypercarbia or apnoea in a patient receiving supplemental oxygen (a patient breathing O₂ with no ventilation can maintain SpO₂ above alarm threshold for many minutes while CO₂ rises dangerously). Capnography is essential for detecting apnoea and oesophageal intubation.
- Capnography (EtCO₂): measures end-tidal CO₂ concentration (normal 35–45 mmHg = 4.6–6.0%) via infrared spectroscopy. It is the gold standard for confirming tracheal tube placement (sustained waveform = tracheal; flat trace = oesophageal). Continuously monitors ventilation adequacy — rising EtCO₂ means hypoventilation; falling EtCO₂ may indicate pulmonary embolism, cardiac arrest, or circuit disconnection.
- ECG: three- or five-lead monitoring for heart rate, rhythm, and ischaemia. Five-lead with CM5 configuration is preferred for detecting ST changes.
- Non-invasive blood pressure (NIBP): automated oscillometric cycling every 2–5 minutes; arterial line (invasive BP) for major surgery or haemodynamic instability.
- Temperature: mandatory for procedures >30 minutes; hypothermia (<36°C) impairs coagulation, drug metabolism, and neuromuscular function — core temperature monitoring (oesophageal probe, nasopharyngeal, tympanic) preferred.
- Neuromuscular monitoring (train-of-four): acceleromyography or mechanomyography of the adductor pollicis using ulnar nerve stimulation at the wrist. TOF ratio ≥0.9 = adequate reversal and safe extubation. TOF ratio <0.9 = residual neuromuscular block — postoperative respiratory complications.
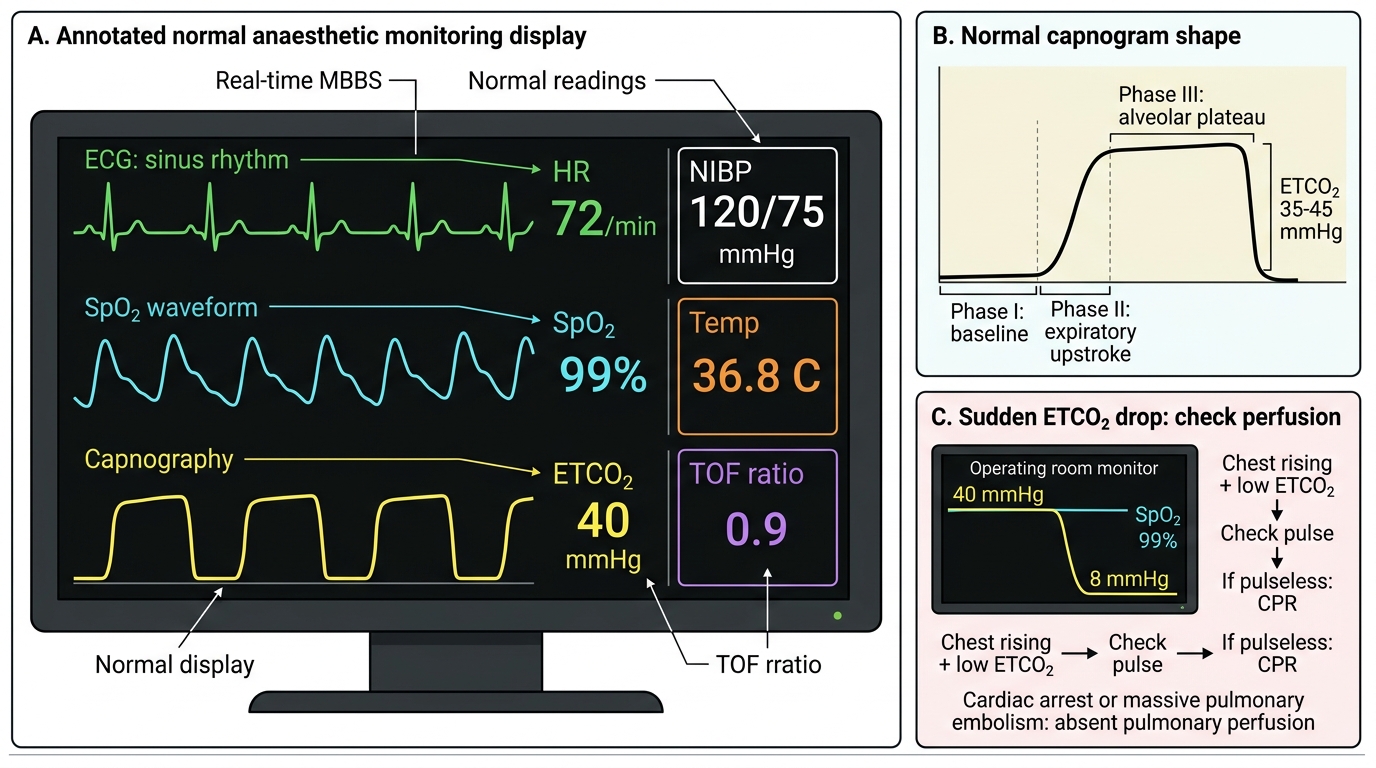
Normal Anaesthetic Monitoring Display
SELF-CHECK
During maintenance of general anaesthesia for a laparotomy, the capnograph shows a sudden drop in ETCO₂ from 40 to 8 mmHg. The patient's SpO₂ remains 99% and the chest is rising with ventilation. What is the most likely cause and what is your immediate action?
A. Oesophageal intubation — immediately remove and re-intubate; the SpO₂ will fall within seconds
B. Cardiac arrest or massive pulmonary embolism causing absent pulmonary perfusion — call for help, check pulse, begin CPR if pulseless
C. Bronchospasm causing air-trapping — increase FiO₂ and give salbutamol
D. Malignant hyperthermia — the falling ETCO₂ is a reassuring sign of decreasing metabolism
Reveal Answer
Answer: B. Cardiac arrest or massive pulmonary embolism causing absent pulmonary perfusion — call for help, check pulse, begin CPR if pulseless
A sudden drop in ETCO₂ to near zero during ongoing mechanical ventilation (chest is rising, so there is no oesophageal intubation or circuit disconnection) with preserved SpO₂ indicates a catastrophic reduction in pulmonary blood flow — either cardiac arrest (pulseless) or massive pulmonary embolism. SpO₂ remains elevated briefly because oxygenated blood already in the pulmonary venous circulation continues to oxygenate for a short period. The immediate response is to check for a pulse — if absent, begin CPR immediately. Oesophageal intubation (A) would have caused a flat trace from the beginning; the scenario states the ETCO₂ dropped suddenly from a normal value, implying it was previously normal. Bronchospasm (C) causes rising ETCO₂ and a 'shark fin' capnograph waveform. Malignant hyperthermia (D) causes dramatically rising ETCO₂, not falling.
Maintenance of Anaesthesia and Vital Organ Support
Maintenance of anaesthesia requires the anaesthesiologist to simultaneously maintain unconsciousness at an appropriate depth, manage analgesia, ensure adequate muscle relaxation (when required), and support the vital functions of the cardiovascular, respiratory, and renal systems — all while anticipating and responding to the physiological insults imposed by surgery. This is the period during which most intraoperative critical incidents occur, and systematic vigilance is the primary preventive strategy.
Respiratory support: All patients under GA with an ETT receive intermittent positive-pressure ventilation (IPPV). Standard initial settings: tidal volume 6–8 mL/kg ideal body weight (lung-protective ventilation), respiratory rate 10–14/min, I:E ratio 1:2, PEEP 5 cmH₂O. FiO₂ titrated to maintain SpO₂ ≥95% (typically 0.4–0.6 for most cases; avoid routine 100% O₂). End-tidal CO₂ target 35–45 mmHg. Ventilator settings are adjusted based on continuous capnography and periodic arterial blood gas analysis in longer cases.
Cardiovascular support: Blood pressure must be maintained within an acceptable range (generally within 20–30% of the preoperative baseline). Hypotension (most common cause = vasodilation from anaesthetic agents, blood loss, or neuraxial spread) is treated by: reducing anaesthetic depth, IV fluid bolus (crystalloid or colloid), vasopressors (ephedrine 3–6 mg IV bolus for mixed alpha-beta effect; phenylephrine 50–100 mcg for predominantly alpha effect preserving heart rate; noradrenaline infusion for refractory hypotension). Hypertension (most common cause = inadequate anaesthetic depth, pain, or pre-existing hypertension) is treated by deepening the anaesthetic, additional analgesia, or antihypertensive agents.
Fluid management: Maintenance IV fluids during surgery are typically Hartmann's solution (compound sodium lactate) or normal saline (0.9% NaCl). Blood loss monitoring (surgical field, suction canisters, swab weights) guides transfusion decisions: typically transfuse when haemoglobin falls below 7–8 g/dL in a healthy patient (lower threshold for cardiac patients: maintain Hb ≥10 g/dL). Coagulation and platelet support as indicated by TEG/ROTEM or clinical/laboratory assessment.
Temperature management: Active warming (forced-air warming blankets, fluid warmers, warm theatre temperature) is mandatory to prevent perioperative hypothermia. Hypothermia (<36°C) impairs platelet function, coagulation factor activity, prolongs drug metabolism, and increases postoperative infection risk.
Depth of anaesthesia monitoring: Bispectral index (BIS) or entropy monitoring measures processed EEG to quantify anaesthetic depth numerically. BIS of 40–60 is the target for adequate unconsciousness; BIS >60 risks awareness; BIS <40 risks excessive depth and delayed emergence. Awareness under anaesthesia (accidental intraoperative consciousness with or without recall) is a rare but devastating complication (incidence ~0.1–0.2%) — risk factors include RSI, light anaesthesia, inadequate NMBA reversal while conscious.
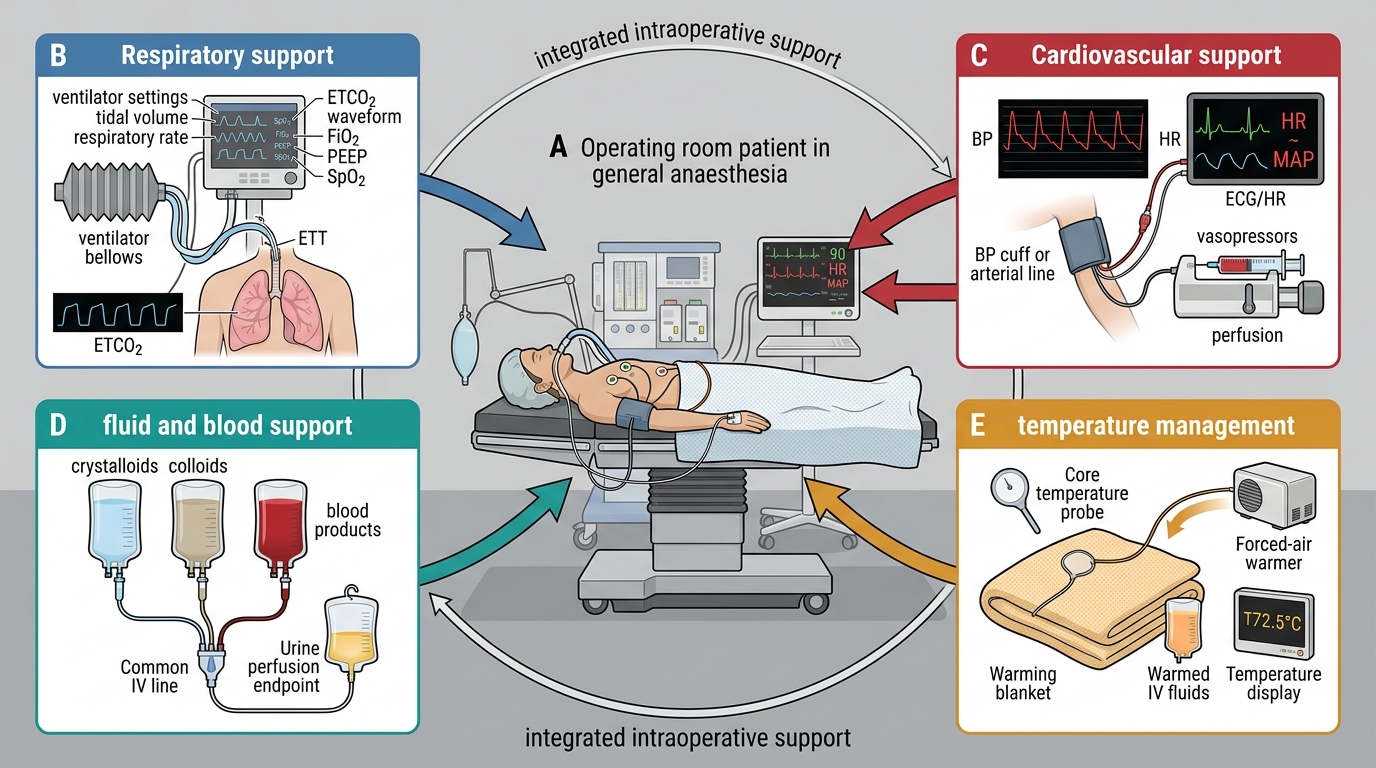
Integrated Intraoperative Vital Organ Support
Applied and Supervised Practice: Emergence, Extubation, and Recovery
Emergence from general anaesthesia — the transition from unconsciousness back to full consciousness — is the second period of maximum vulnerability. Like induction, it involves a predictable sequence of returning protective reflexes: the reverse of their loss, but with added complication that the patient may be in pain, hypothermic, nauseated, residually paralysed, or disoriented. The anaesthesiologist manages emergence systematically, anticipating each potential problem.
Planned emergence sequence: As surgery concludes, inhalational agent or TIVA infusion is reduced to allow the patient to regain spontaneous ventilation. If a neuromuscular blocking agent was used, reversal is given (neostigmine + glycopyrrolate, or sugammadex) and confirmed by TOF ratio ≥0.9 before extubation. Analgesic coverage must be adequate before extubation — opioid tolerance from intraoperative remifentanil infusion means post-infusion analgesia must be pre-emptively established with a longer-acting agent (morphine or fentanyl bolus, paracetamol, NSAID) before stopping the remifentanil.
Extubation criteria (all must be met simultaneously): patient responsive to commands; spontaneous breathing with adequate tidal volumes; SpO₂ maintained without manual assistance; TOF ratio ≥0.9; normothermic; haemodynamically stable; protective airway reflexes returning (swallowing, gagging on the tube). Extubation before these criteria are met risks laryngospasm, aspiration, hypoxia, and re-intubation.
Post-extubation monitoring: After extubation, the patient is placed in the semi-recumbent or lateral recovery position (reduces tongue-fall obstruction and aspiration risk). Supplemental O₂ is applied (Hudson mask 40% or nasal cannula 2–4 L/min). The patient is transferred to the Post-Anaesthesia Care Unit (PACU) where monitoring continues: SpO₂, ECG, NIBP, respiratory rate, pain score (numeric rating scale 0–10), PONV (postoperative nausea and vomiting) assessment. The Aldrete score or modified Aldrete score (activity, respiration, circulation, consciousness, SpO₂) is used to determine readiness for discharge from PACU to the ward.
Postoperative nausea and vomiting (PONV) is the most common postoperative complication (~30% incidence; up to 80% in high-risk patients — female sex, non-smoker, history of PONV/motion sickness, opioid use, volatile anaesthetic use). Prophylaxis: ondansetron 4–8 mg IV, dexamethasone 4–8 mg IV at induction (also reduces pain and swelling in some contexts), metoclopramide. TIVA with propofol reduces PONV vs volatile anaesthesia.
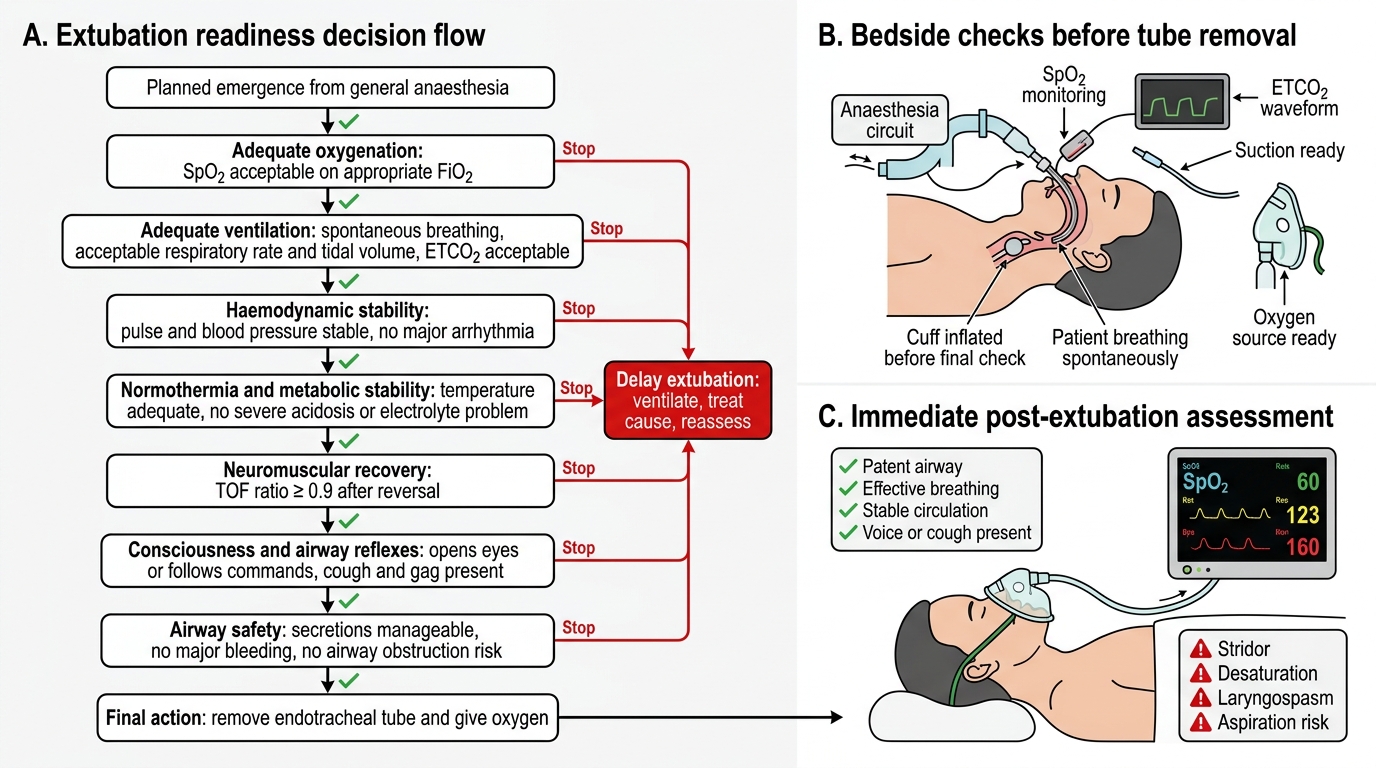
Extubation Readiness Assessment