Page 1 of 9
AS6.1-3 | Recovery Room Monitoring, Crash Cart Readiness and Complication Management — SDL Guide
References
CLINICAL SCENARIO
A 52-year-old woman undergoes elective laparoscopic cholecystectomy under general anaesthesia. Within eight minutes of arriving in the recovery room, she becomes increasingly agitated, her SpO₂ drops to 88% on 4 L/min oxygen, and her respiratory rate climbs to 28 breaths per minute. The recovery nurse calls for help and reaches for the crash cart. What has happened, how should it be recognised, and what must already be in place before it occurs? The post-anaesthesia recovery room is a deceptively high-acuity environment: patients arrive pharmacologically impaired, physiologically stressed, and often unable to articulate their distress. The difference between a smooth recovery and a catastrophe is a combination of vigilant structured monitoring, immediate access to resuscitation equipment, and the ability to recognise and treat complications without hesitation.
WHY THIS MATTERS
For a final-year medical student who will rotate through surgical wards, emergency departments, and eventually supervise post-operative patients, the recovery room represents the first interface between intraoperative anaesthetic management and the ward environment. Understanding PACU monitoring principles and crash cart readiness is directly relevant to your day-to-day clinical work: you will be the first responder at many post-operative bedside emergencies before the anaesthetist or senior surgeon arrives. The NMC 2024 competencies AS6.1–AS6.3 require you to describe monitoring and resuscitation principles, enumerate crash cart contents, and explain how common PACU complications are recognised and managed. Mastery of these competencies operationalises patient safety in the immediate post-operative period — a domain where junior doctors can and do save lives.
RECALL
Before engaging with this module, take a moment to consolidate what you already know. Recall the four main drug classes used in a general anaesthetic — induction agents, volatile or intravenous maintenance agents, opioids, and neuromuscular blocking agents (NMBAs) — because the recovery period is defined physiologically by their residual effects and pharmacological reversal. Recall the basics of oxygen delivery: the nasal cannula delivers approximately 24–44% FiO₂ at 1–6 L/min, a simple facemask delivers approximately 40–60% FiO₂, and the non-rebreather mask can achieve 60–90% FiO₂. Recall the adult basic life support algorithm: chest compressions at 100–120/min, depth 5–6 cm, ratio 30:2, with defibrillation reserved for shockable rhythms (VF and pulseless VT) — not for asystole or PEA. Finally, recall the distinction between the sympathetic and parasympathetic nervous systems, because many PACU complications — laryngospasm, bronchospasm, PONV, and haemodynamic instability — reflect autonomic imbalance in a patient whose homeostasis has been chemically disrupted.
The Post-Anaesthesia Care Unit: Purpose, Transfer Criteria, and Initial Stabilisation
The Post-Anaesthesia Care Unit (PACU), commonly called the recovery room, is a dedicated, purpose-built clinical area staffed by trained nurses and with immediate anaesthetist cover, where patients are observed during the critical period of emergence from anaesthesia and before return to the general ward. The fundamental rationale for the PACU is that the hour following extubation or emergence from anaesthesia carries the highest risk of airway compromise, haemodynamic instability, and pharmacological side effects from residual anaesthetic agents. General anaesthetics blunt all the protective reflexes — laryngeal, gag, and cough — and the PACU provides a bridge during which these reflexes return to baseline while continuous monitoring identifies deterioration early enough for intervention.
Transfer from the operating theatre to the PACU requires that the patient meets a minimum set of transfer criteria before leaving the anaesthetist's direct care. The patient must have an adequate airway — spontaneous ventilation restored and maintained, SpO₂ ≥95% on supplemental oxygen, and no signs of laryngeal obstruction. Cardiovascular stability is required: blood pressure within 20% of the pre-operative baseline and heart rate between 50 and 100 beats per minute without life-threatening arrhythmia. Airway reflexes (cough and gag) must be returning and the patient should be responsive to verbal commands, even if not yet fully awake. Any neuromuscular block must have been reversed pharmacologically or demonstrated to have resolved clinically (sustained head-lift for 5 seconds, strong hand grip). The anaesthetist provides a verbal handover to the PACU nurse using a structured communication tool — minimally: patient name, procedure, anaesthetic technique, intraoperative events, intravenous fluids given, and any specific concerns.
On arrival in the PACU, initial stabilisation is performed within the first two minutes. Oxygen is applied immediately — typically a simple facemask at 6–8 L/min or a non-rebreather mask if the patient is hypoxic. Continuous monitoring is connected: pulse oximetry, ECG, and non-invasive blood pressure (NIBP) are the mandatory minimum. Temperature is checked, because hypothermia from cold operating theatres and open body cavities is nearly universal and predisposes to shivering, increased oxygen demand, and cardiac arrhythmias. An intravenous cannula must be confirmed patent and accessible. The PACU nurse performs a structured primary survey — airway patency, respiratory rate and quality, SpO₂, blood pressure, heart rate, level of consciousness, and pain score — and documents a baseline set of observations.
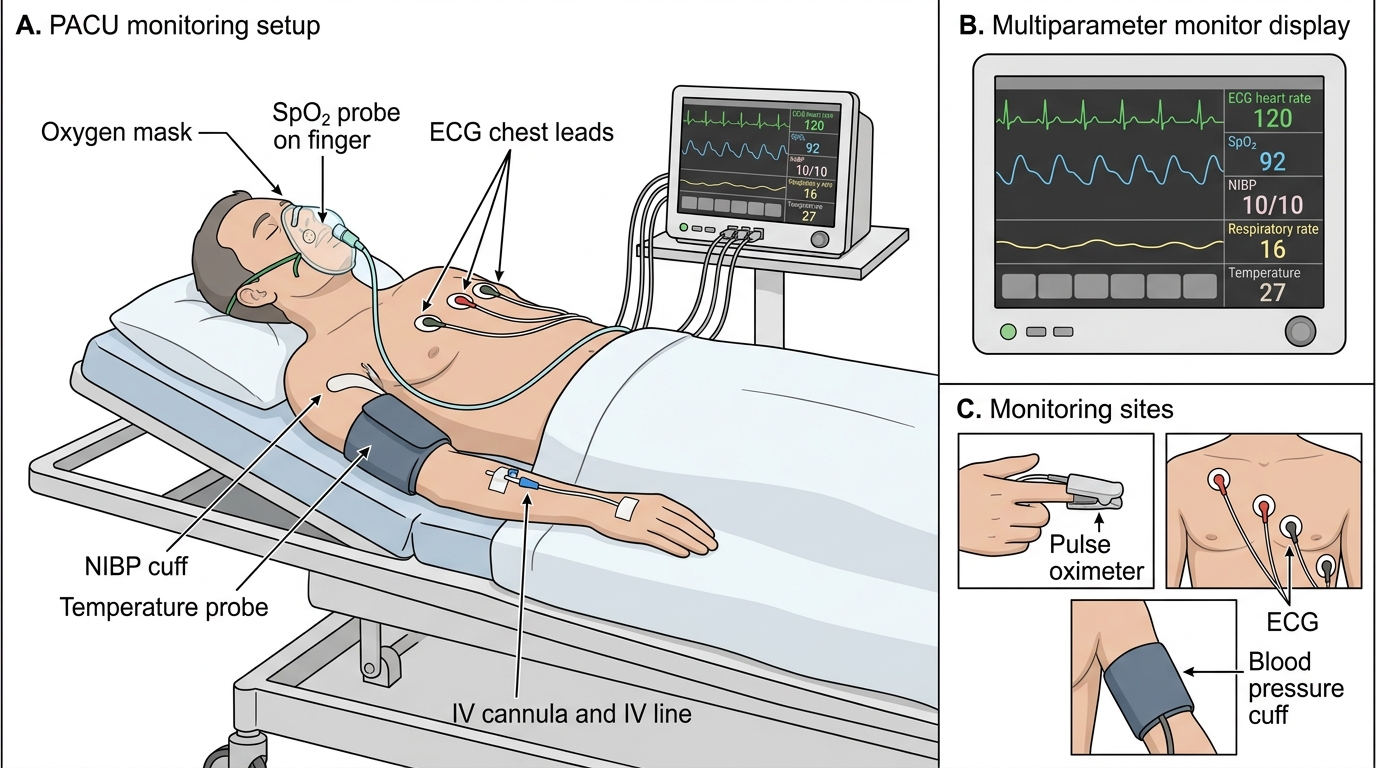
PACU Monitoring Setup
Physiological Vulnerabilities in the Immediate Post-Anaesthetic Period
Understanding why the recovery room is hazardous requires a precise appreciation of the pharmacological and physiological disruptions that all anaesthetic agents produce. The immediate post-anaesthetic period is not a passive 'waking up' but an active state of physiological vulnerability shaped by the residual effects of every drug administered intraoperatively.
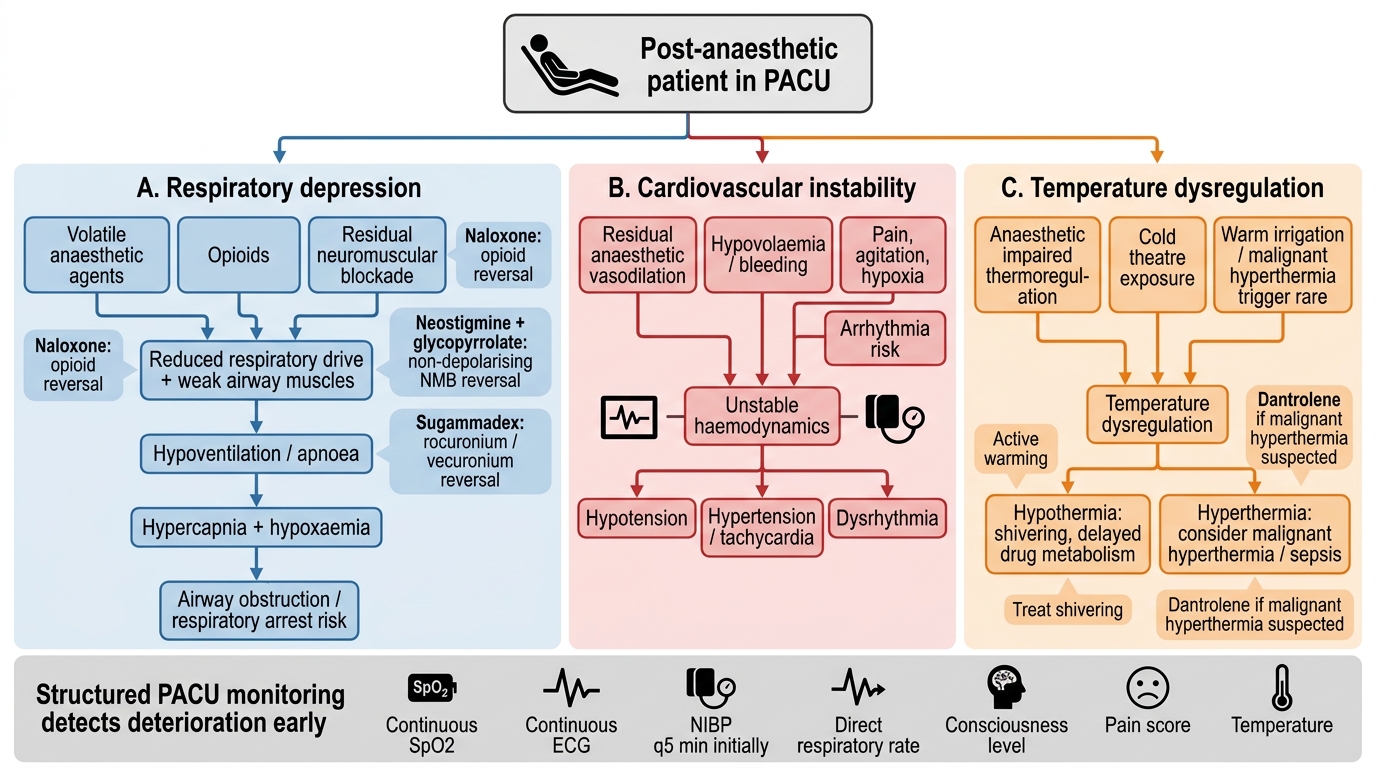
Respiratory system vulnerability is the most immediately life-threatening axis. Volatile anaesthetic agents (sevoflurane, isoflurane, desflurane) produce dose-dependent depression of the hypoxic and hypercapnic ventilatory drives. Even at low residual concentrations these agents blunt the normal reflex increase in respiratory rate and tidal volume in response to rising PaCO₂. Intraoperative opioids — fentanyl, morphine, remifentanil — add opioid-mediated respiratory depression, characterised by a slow rate (bradypnoea) with relatively preserved tidal volumes in mild cases, progressing to apnoea with high doses or in opiate-naïve patients. Residual neuromuscular block from non-depolarising NMBAs (vecuronium, rocuronium, atracurium) reduces the force-generating capacity of the diaphragm and intercostal muscles, causing hypoventilation even if the patient appears awake. The upper airway is particularly vulnerable: pharyngeal muscle tone is the last to return after general anaesthesia, so the patient who appears to be breathing spontaneously may still have a partially obstructed airway requiring a simple jaw thrust or oral airway adjunct.
Cardiovascular vulnerability reflects the interplay of residual vasodilatory effects of anaesthetic agents, fluid shifts, residual pain, and neuroendocrine stress responses. Propofol and volatile agents both reduce systemic vascular resistance; combined with the fluid losses of surgery (perspiration, bleeding, third-space redistribution), hypotension is a common early PACU event. Conversely, the emergence stimulus — laryngeal irritation at extubation, pain on awakening, and catecholamine surge — produces hypertension and tachycardia in many patients, particularly those with pre-existing hypertension or cardiac disease. Shivering, which occurs in up to 40% of patients due to intraoperative hypothermia, dramatically increases oxygen consumption and cardiac work, creating relative ischaemia in patients with limited cardiac reserve.
Pharmacological reversal agents used in the PACU must be understood by mechanism and risk. Naloxone is a competitive opioid-receptor antagonist used to reverse opioid-induced respiratory depression; it is given in titrated increments of 0.1–0.2 mg IV (not 0.4 mg boluses, which cause abrupt reversal with catecholamine surge, pulmonary oedema, and severe pain). Naloxone has a short half-life of approximately 30–60 minutes, shorter than most surgical opioids, so re-narcotisation (return of respiratory depression) can occur after an initial reversal — vigilance must continue and repeated doses may be needed. Neostigmine (paired with glycopyrrolate to block its muscarinic side effects) reverses non-depolarising NMB by inhibiting acetylcholinesterase at the neuromuscular junction. It is not effective if block is profound (train-of-four count <2 twitches) and has a ceiling effect; sugammadex is the modern reversal agent for rocuronium and vecuronium, capable of reversing even deep block. Flumazenil reverses benzodiazepine sedation but has a shorter duration than midazolam, so re-sedation is possible.
Physiological Vulnerabilities in the Post-anaesthetic Period
Structured Monitoring in the PACU: Parameters, Tools, and the Aldrete Score
Systematic, structured monitoring is the mechanism by which the PACU nurse detects deterioration before it becomes an emergency. This is not intuitive monitoring — it is protocol-driven, documented observation at defined intervals, using validated scoring tools that force a complete assessment every time.
The minimum mandatory monitoring parameters in the PACU, consistent with the standards described in Morgan & Mikhail's Clinical Anesthesiology, are: (1) pulse oximetry — continuous SpO₂ with an audible alarm; (2) ECG — continuous cardiac rhythm monitoring; (3) non-invasive blood pressure — at minimum every 5 minutes in the first 30 minutes, then every 15 minutes when stable; (4) respiratory rate — directly counted, not inferred from SpO₂; (5) level of consciousness — assessed using a simple scale (eyes open spontaneously / to command / to pain / none); (6) pain score — numerical rating scale 0–10 or a behavioural scale for non-communicative patients; (7) temperature — at admission and as indicated. For high-acuity patients — those who were intubated and ventilated, had major blood loss, known cardiac disease, or received high-dose opioids — end-tidal CO₂ monitoring should continue, and invasive arterial pressure monitoring (via pre-existing arterial line) is used in haemodynamically unstable patients.
The Aldrete Score (Modified Aldrete or Post-Anaesthetic Recovery Score) is the validated scoring system used to determine when a patient is ready for discharge from the PACU to the ward. It assesses five parameters, each scored 0, 1, or 2, giving a maximum total score of 10:
- Activity: 2 = moves all four extremities voluntarily or on command; 1 = moves two extremities; 0 = unable to move extremities
- Respiration: 2 = breathes deeply and coughs freely; 1 = dyspnoea, shallow or limited breathing; 0 = apnoea
- Circulation: 2 = BP within ±20% of pre-anaesthetic level; 1 = BP within ±20–49%; 0 = BP differs >50% from baseline
- Consciousness: 2 = fully awake; 1 = arousable on calling; 0 = not responding
- Oxygen saturation: 2 = SpO₂ >92% on room air; 1 = SpO₂ >90% requiring supplemental O₂; 0 = SpO₂ <90% even with supplemental O₂
A score of 9 or 10 is typically required for discharge from the PACU to the general ward. A score of 8 or below, or any individual parameter scoring 0, requires medical review before discharge. The score is reassessed every 15–30 minutes and documents the trajectory of recovery.
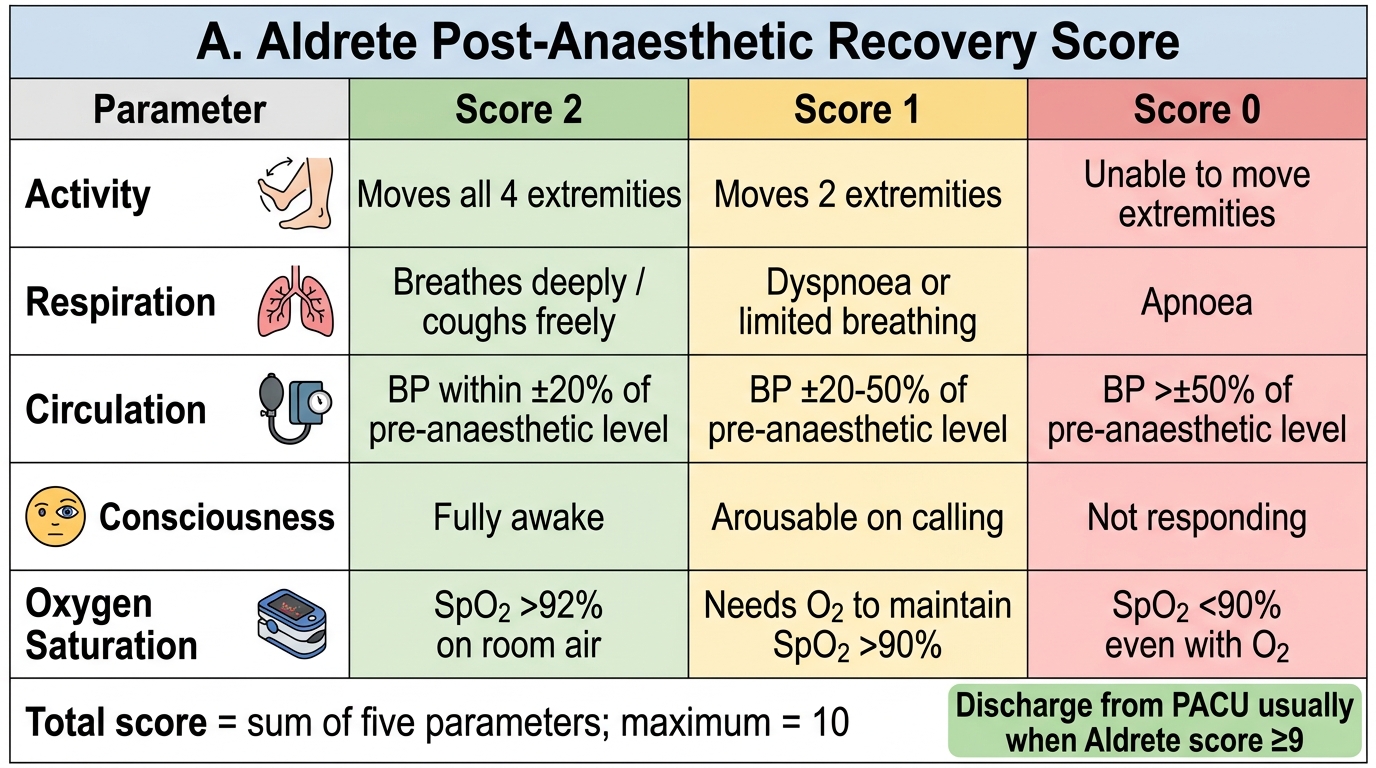
Aldrete Post-Anaesthetic Recovery Score