Page 2 of 9
AS6.1-3 | Recovery Room Monitoring, Crash Cart Readiness and Complication Management — SDL Guide (Part 2)
Crash Cart Contents and Equipment Readiness in the Recovery Room
The crash cart (resuscitation trolley) in the PACU must be immediately accessible — ideally positioned within ten seconds of every PACU bay — and must be checked at the beginning of every nursing shift using a documented checklist. The crash cart is not merely a collection of equipment; it is a system that is relied upon with zero tolerance for missing items in a life-threatening emergency. Understanding the crash cart is an NMC AS6.2 competency and is directly assessed in OSCE stations because a delay finding a drug or device during CPR is not a theoretical problem — it costs lives.
The standard PACU crash cart is organised into logical drawers or zones, typically structured as follows:
Airway and ventilation zone (top of cart or separate trolley): bag-valve-mask (BVM) device in adult and paediatric sizes; oxygen supply with flow meter and mask; oropharyngeal airways (Guedel airways) sizes 2, 3, 4; nasopharyngeal airways; laryngoscope handles with Macintosh blades sizes 3 and 4 with spare batteries and bulbs; endotracheal tubes (ETTs) sizes 7.0, 7.5, 8.0 with 10-mL syringe for cuff inflation; LMA (laryngeal mask airway) sizes 3, 4, 5; Magill forceps; suction catheter (Yankauer) and suction tubing connected to working suction machine; 10-mL syringe and lubricant.
Circulation and defibrillation zone: automated external defibrillator (AED) or manual defibrillator with pads pre-attached; defibrillation gel or pads; ECG monitoring leads.
Drug drawer: the standard ACLS drugs that must be present in the PACU crash cart include:
- Adrenaline (epinephrine) 1 mg/mL ampoules — for PEA/asystole/VF (1 mg IV every 3–5 min in cardiac arrest) and for anaphylaxis (0.5 mg IM in the vastus lateralis)
- Atropine 0.6 mg/mL ampoules — for symptomatic bradycardia (0.5–1 mg IV, repeat to max 3 mg)
- Amiodarone 150 mg/3 mL ampoules — for VF/pulseless VT (300 mg IV bolus in cardiac arrest; 150 mg for stable VT)
- Sodium bicarbonate 8.4% (50 mL vial) — for severe metabolic acidosis or hyperkalaemia-associated cardiac arrest
- 50% dextrose (50 mL vial) — for hypoglycaemia-induced unconsciousness
- Naloxone 0.4 mg/mL ampoules — for opioid-induced respiratory depression (titrated 0.1–0.2 mg increments IV)
- Suxamethonium 100 mg/2 mL ampoule — for rapid-sequence intubation in emergency airway management in the PACU
- Hydrocortisone 100 mg vial and chlorphenamine (10 mg ampoule) — for anaphylaxis second-line
- Calcium gluconate or chloride — for hyperkalaemia treatment
- Normal saline (0.9%) and dextrose-saline (D5NS) IV bags for fluid resuscitation
Vascular access zone: IV cannulae (multiple gauges: 14G, 16G, 18G, 20G), tourniquet, adhesive tape, tegaderm dressing, syringes (2 mL, 5 mL, 10 mL, 20 mL), intravenous giving sets, three-way tap, and an intraosseous needle set for emergency access if IV access fails.
The crash cart must be sealed with a numbered tamper-evident seal after each check, so that a broken seal is immediately visible without needing to open drawers. Seal number must be documented on the shift checklist. Any use of the cart requires immediate restocking and resealing before the next patient is admitted.
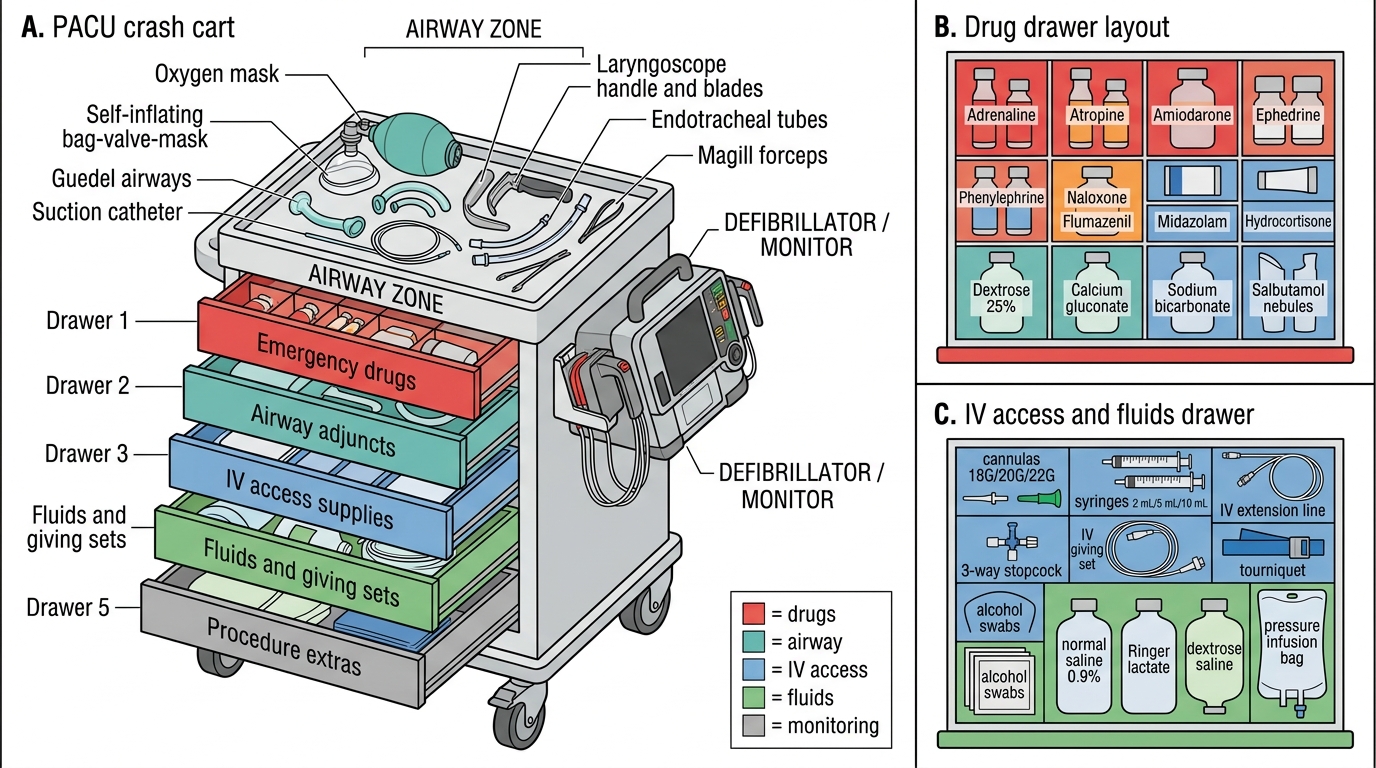
PACU Crash Cart Drawer Layout
Recognition and Management of Common PACU Complications
PACU complications are frequent, predictable, and time-sensitive. The ability to recognise them early and initiate appropriate management is the operational core of AS6.3. The complications described here are organised by body system, consistent with the approach in Morgan & Mikhail's Clinical Anesthesiology.
Respiratory complications are the most dangerous in the PACU:
Airway obstruction is the most common and immediately life-threatening respiratory complication, most frequently caused by the tongue falling back against the posterior pharyngeal wall in a sedated patient with reduced pharyngeal muscle tone. Recognition: snoring or gurgling respirations, paradoxical chest and abdominal movement (see-saw pattern), absent air entry at the mouth and nose despite respiratory effort. Management: immediate jaw thrust or chin lift; insert an oropharyngeal (Guedel) airway if tolerated; apply 100% oxygen via non-rebreather mask; if unresolved, call anaesthetist for laryngoscopy or intubation.
Laryngospasm is a reflexive, sustained closure of the vocal cords triggered by secretions, blood, or stimulation of the larynx before airway reflexes have fully returned. Recognition: high-pitched inspiratory stridor (partial laryngospasm) progressing to complete absence of breath sounds despite respiratory effort (complete laryngospasm), with desaturation. Management: immediate continuous positive airway pressure (CPAP) with 100% oxygen via tight-fitting mask; the Larson manoeuvre (firm digital pressure in the laryngospasm notch — the depression between the mastoid process and the angle of the mandible bilaterally) may break spasm; if SpO₂ drops below 90%, a small dose of suxamethonium (0.1–0.5 mg/kg IV, sometimes called the 'lytic dose') is given to relax the cords without full paralysis. Persistent or complete laryngospasm unresponsive to CPAP requires full suxamethonium dose (1–1.5 mg/kg IV) and emergency intubation.
Bronchospasm presents with expiratory wheeze, prolonged expiratory phase, and rising peak airway pressures (in a ventilated patient). It is more common in patients with asthma, COPD, smokers, and following airway irritation. Management: 100% oxygen; inhaled salbutamol (2.5–5 mg nebulised); IV aminophylline or hydrocortisone in severe cases; adrenaline for refractory bronchospasm.
Hypoventilation and hypercapnia result from residual opioid effect, NMBA residual block, or splinting due to pain. Recognition: slow respiratory rate (<10/min), shallow breathing, CO₂ rise on capnography, patient difficult to arouse. Management: verbal stimulation; supplemental oxygen; if opioid-mediated — titrate naloxone (0.1–0.2 mg increments IV, observing for effect); if NMBA residual — neostigmine or sugammadex under anaesthetist direction; if pain-mediated — analgesia.
Hypoxia despite oxygen therapy warrants careful assessment: consider atelectasis (commonest — managed with deep breathing exercises and physiotherapy), pulmonary oedema (common in patients with heart failure or following large fluid loads — managed with diuretics and upright positioning), or pulmonary embolism in high-risk patients.
Cardiovascular complications:
Post-operative hypertension (BP >20% above baseline) is extremely common, driven by pain, anxiety, fluid overload, hypercapnia, pre-existing hypertension, and bladder distension. Initial management targets the cause: adequate analgesia, treat hypercapnia, empty the bladder. If persistent and above 180/110 mmHg, intravenous antihypertensives (labetalol, hydralazine, or glyceryl trinitrate infusion) may be required.
Post-operative hypotension (BP >20% below baseline) requires rapid assessment of cause: hypovolaemia (most common — surgical bleeding or inadequate intraoperative fluid replacement), cardiac dysfunction (MI, arrhythmia), vasodilation (sepsis, anaphylaxis, neuraxial block), or high spinal anaesthesia. Management: raise legs (Trendelenburg if no contraindication), IV fluid bolus (250–500 mL crystalloid), vasopressors (metaraminol or ephedrine for anaesthetic-related vasodilation), and senior review if unresponsive.
Cardiac arrhythmias in the PACU — sinus tachycardia (pain, hypovolaemia), sinus bradycardia (opioids, high spinal, vagal stimulus — treat with atropine 0.5–1 mg IV), atrial fibrillation (underlying cardiac disease, electrolyte abnormality), and VF/VT requiring immediate ACLS.
Neurological complications:
Delayed emergence (failure to wake within 30–60 minutes of stopping anaesthesia) should prompt a structured assessment: overdose of residual agents (opioids — give naloxone; benzodiazepines — give flumazenil), severe hypothermia (rewarm), hypoglycaemia (check BGL — give 50 mL of 50% dextrose IV if <3 mmol/L), hypoxia and hypercarbia (check ABG), stroke (rare — CT head if no pharmacological cause found).
Emergence agitation (disorientation, combativeness) is common in young male patients, those with a history of alcohol use, following sevoflurane anaesthesia, and in patients in pain. Management: ensure safety (prevent falls, protect IV line), rule out hypoxia and hypoglycaemia, adequate analgesia, reassurance, and small doses of propofol (10–20 mg IV) or midazolam if required.
Post-operative nausea and vomiting (PONV) occurs in 20–30% of all surgical patients, with higher risk in females, non-smokers, patients with history of PONV or motion sickness, those receiving opioids, and longer procedures. Management: ondansetron 4 mg IV (first-line); metoclopramide 10 mg IV; dexamethasone (if not given prophylactically); prochlorperazine. Positioning the patient on their side reduces aspiration risk during active vomiting.
Hypothermia (core temperature <36°C) is nearly universal after prolonged general anaesthesia. It causes shivering (increases O₂ demand 300%), impairs coagulation, delays drug metabolism, and triggers sympathetic activation. Management: active warming with forced-air warming blankets (Bair Hugger), warmed IV fluids, increasing room temperature. Pethidine 25 mg IV specifically suppresses shivering by acting on κ-opioid receptors.
Surgical site bleeding: any patient with unexpected tachycardia, hypotension, and swelling or drainage at the operative site must be assessed for post-operative haemorrhage. Senior surgical review is mandatory; aggressive IV fluid resuscitation and preparation for return to theatre if haemorrhage is confirmed.
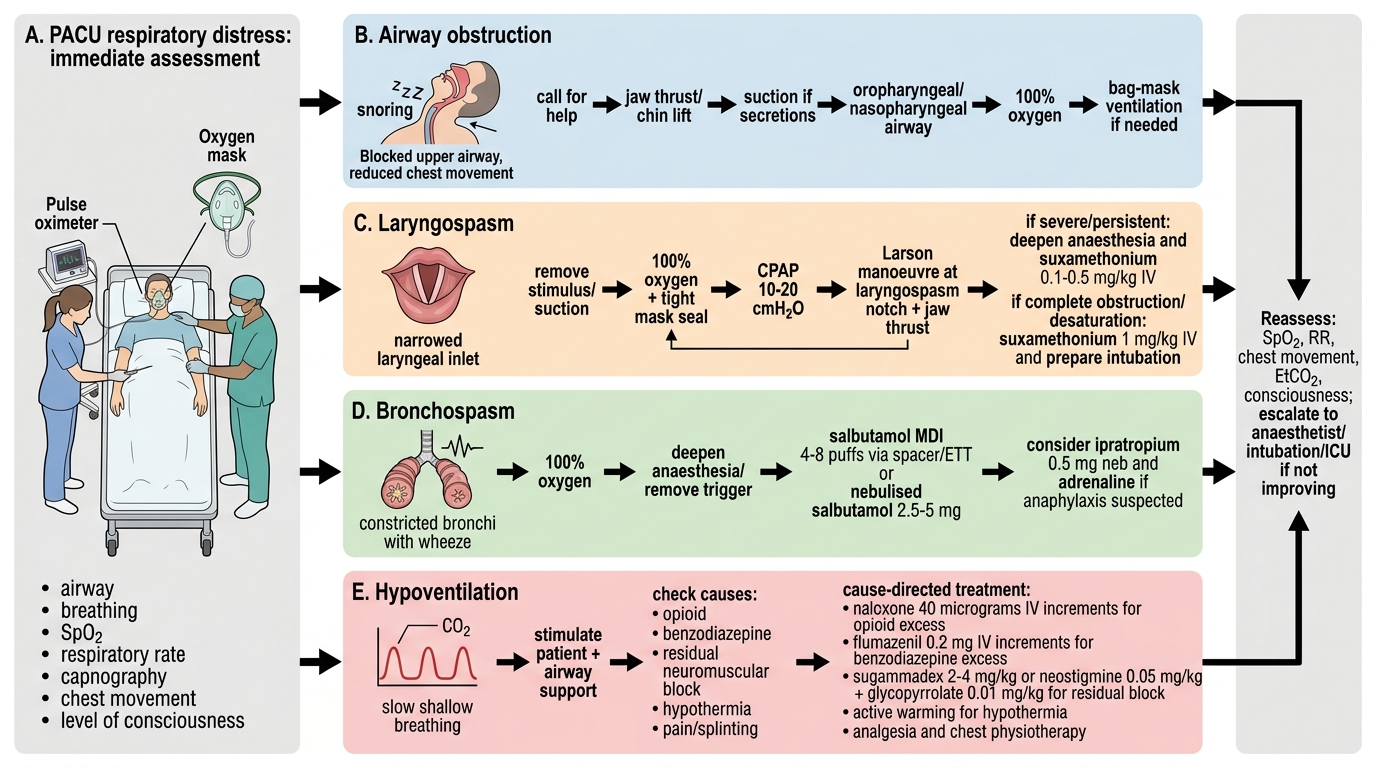
PACU Respiratory Complication Management
Discharge Criteria and Handover from the PACU
Discharge from the PACU to the surgical ward is a formal clinical decision — not a passive event that happens when the patient 'looks well enough.' The anaesthetist or a senior recovery nurse with delegated authority signs off discharge based on objective criteria, documented in the patient's anaesthetic record.
In addition to achieving an Aldrete Score of ≥9, the following criteria must be met before discharge: adequate pain control (pain score ≤4 on a 0–10 scale, patient able to perform deep breathing and coughing), PONV absent or controlled, no active bleeding from the surgical site, temperature ≥36°C (or active warming in progress on the ward if mildly hypothermic), urine output satisfactory if urinary catheter in situ, and intravenous access patent. For patients who received a regional anaesthetic — spinal or epidural — motor block must be resolving and haemodynamic stability must be confirmed before transfer, because a high residual spinal block can cause sudden cardiovascular collapse during movement.
The handover to the ward nurse must include: patient name, procedure, anaesthetic technique, intraoperative events, fluid balance, current analgesic plan (including what has been given and what is prescribed), antiemetic given, any special instructions (nil by mouth duration, next physiotherapy time, wound drain care), and any concerns for the next 12 hours. A written anaesthetic record must accompany the patient. Poor handover is a recognised root cause of preventable post-operative adverse events and must be approached with the same rigour as a structured professional handover in any other clinical setting.
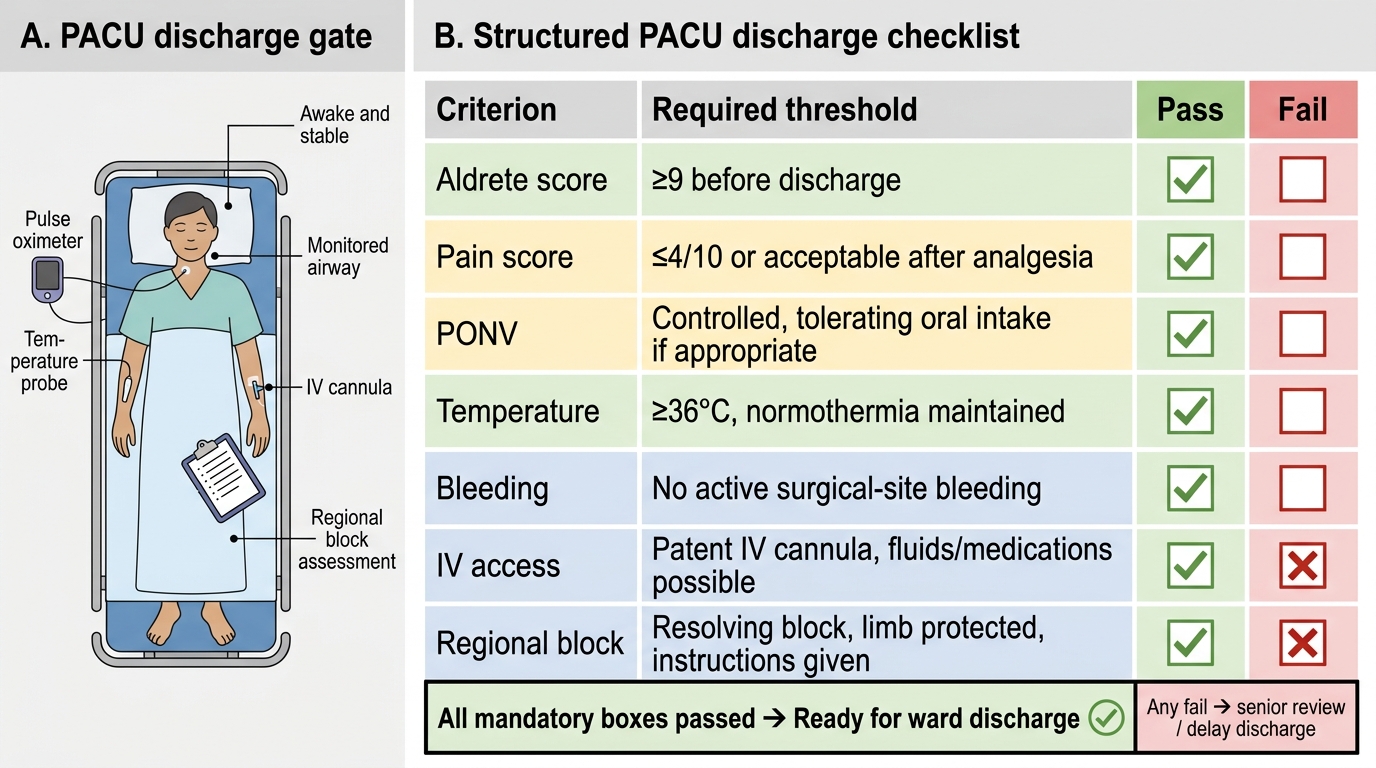
Structured PACU Discharge Checklist