Page 1 of 13
AS7.1-2 | ICU Organization, Functions and Admission-Discharge Criteria — SDL Guide
Learning Objectives
- Describe the physical layout, staffing structure, and equipment configuration of a functioning Intensive Care Unit
- Enumerate the clinical and physiological criteria that guide admission of a patient to the ICU
- Enumerate the criteria for discharging a patient from the ICU to a step-down ward or general floor
- Recognise the role of the anaesthesiologist in ICU leadership and multidisciplinary critical-care teamwork
INSTRUCTIONS
Intensive care medicine represents the frontline of life-threatening illness management. Understanding the ICU — its physical design, staffing, equipment, and decision frameworks for admission and discharge — is foundational for every graduating doctor who will counsel patients and families, make initial triage decisions, and coordinate with ICU teams throughout a career.
References
- Morgan & Mikhail's Clinical Anesthesiology, 6th ed., Chapter 57: Critical Care Medicine (textbook)
- Ajay Yadav's Short Textbook of Anaesthesia, Chapter on Intensive Care (textbook)
- Paul G. Barash et al., Clinical Anesthesia, 8th ed., Section on ICU and Critical Care (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 38-year-old road-traffic accident victim arrives unconscious to the casualty. After emergency stabilisation, the surgical team wants to move him to a general ward. The anaesthesiologist firmly advises ICU admission instead — citing a GCS of 8, uncontrolled haemodynamic swings, and the need for invasive arterial monitoring. Forty-eight hours later, the patient walks out of the ICU neurologically intact. That decision — grounded in a clear understanding of what an ICU can offer and who genuinely needs it — is exactly what this module equips you to make.
WHY THIS MATTERS
Every branch of medicine eventually sends patients to intensive care. A gynaecologist managing eclampsia, a physician treating septic shock, a surgeon post-laparotomy — all depend on the ICU to provide a level of monitoring and intervention impossible on the general ward. As a final-year student you will triage admissions, explain ICU care to anxious families, and contribute to discharge decisions. Understanding ICU structure and criteria is therefore not an anaesthesia subspecialty curiosity — it is core clinical knowledge that shapes patient outcomes across every discipline.
RECALL
Before proceeding, recall what you already know: the clinical signs of acute haemodynamic instability (hypotension, tachycardia, poor peripheral perfusion), the components of the Glasgow Coma Scale (eye opening E1-4, verbal response V1-5, motor response M1-6; minimum 3, maximum 15), the physiological parameters tracked on a bedside vital-signs chart, and the general principle that organ support — mechanical ventilation, vasopressors, renal replacement — is qualitatively different from general-ward nursing care. These foundations underpin every admission-discharge criterion you will study here.
The ICU as a Clinical Environment: Context and Historical Indication
The concept of an Intensive Care Unit emerged in the 1950s during polio epidemics, when patients with respiratory failure required continuous ventilatory support and close monitoring that standard wards could not provide. The modern ICU is a geographically distinct clinical area of a hospital designed to care for patients with established or potentially life-threatening, single or multiple, organ failure, where comprehensive clinical monitoring and organ-support technology are immediately available around the clock. The indications that originally justified separate units — ventilatory failure, cardiovascular instability, acute neurological deterioration — remain the core clinical contexts today, though they have expanded to include post-operative high-risk surgery, severe sepsis and septic shock, poisoning with haemodynamic compromise, and complex multi-organ dysfunction. In the Indian hospital setting, ICU beds represent a scarce and expensive resource: national figures consistently show that public hospitals have fewer than two ICU beds per 100,000 population, making appropriate admission and discharge decisions critically important to avoid occupancy by patients who no longer require organ support while ensuring that those who do are not left on general wards where outcomes are significantly worse. The anaesthesiologist's training in airway management, haemodynamic physiology, pharmacology, and mechanical ventilation places the specialty at the centre of modern critical-care leadership — the majority of level-III ICUs globally are led or co-led by intensivists with anaesthesia backgrounds.
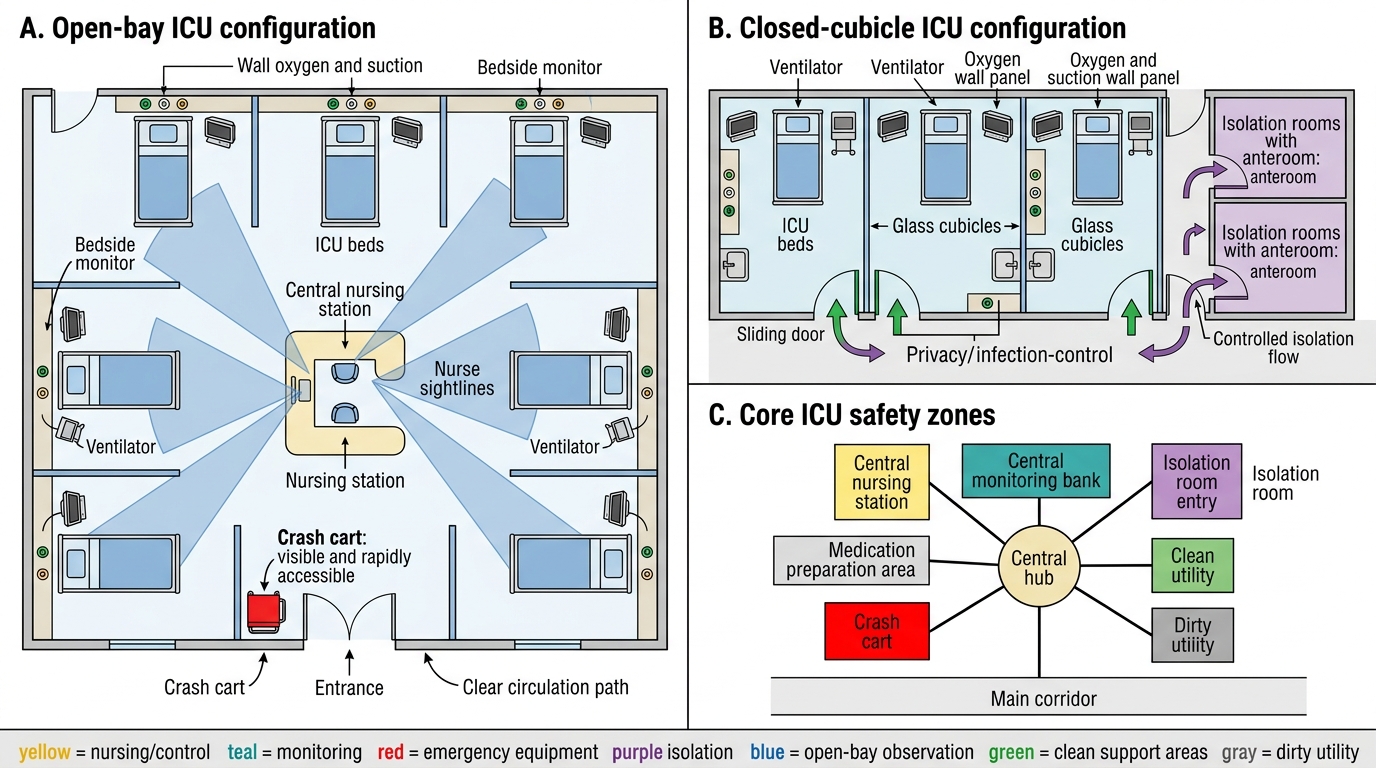
Modern ICU Ward Layout: Open-Bay and Cubicle Configurations
ICU Classification and Physical Layout
ICUs are classified both by the level of care they provide and by the patient population they serve. By care level, the three-tier system is most widely referenced: Level I (basic) units offer continuous monitoring of vital signs, basic life support, and 24-hour nursing care but rely on transfer to higher-level facilities for complex intervention; Level II (intermediate) units provide mechanical ventilation, invasive haemodynamic monitoring, and basic organ support; Level III (tertiary/referral) units are fully equipped for all forms of organ support including renal replacement therapy, extracorporeal membrane oxygenation (ECMO), continuous renal replacement therapy (CRRT), intra-aortic balloon pump (IABP), and high-level specialist input. By patient population, ICUs are further specialised into medical (MICU), surgical (SICU), cardiac (CCU or CICU), neuro (NICU), paediatric (PICU), and neonatal (NICU) units. The physical layout follows one of two major configurations: open-bay designs place multiple beds in a shared space separated by curtains or low partitions, maximising nurse-to-patient visual surveillance; closed-cubicle designs provide individual rooms or glass-walled bays, essential for infection control in immunocompromised patients and for isolation of multidrug-resistant organisms. National and international guidelines (ISCCM 2014; SCA India; Australian and New Zealand Intensive Care Society) specify minimum space per bed — typically 15-20 square metres in a closed bay — and mandate dedicated power supply (UPS-backed), piped medical gases (oxygen, air, nitrous oxide), vacuum suction at each bedside, and provision for minimum nurse-to-patient ratios.
Key layout components at each bedside: ceiling-mounted or articulated arm-mounted ventilator, bedside monitoring unit (multi-parameter monitor for ECG, SpO2, ETCO2, IBP, CVP, temperature), infusion pump stack, bedside height-adjustable table for documentation, patient call system, isolation gown and glove dispenser in cubicle units.
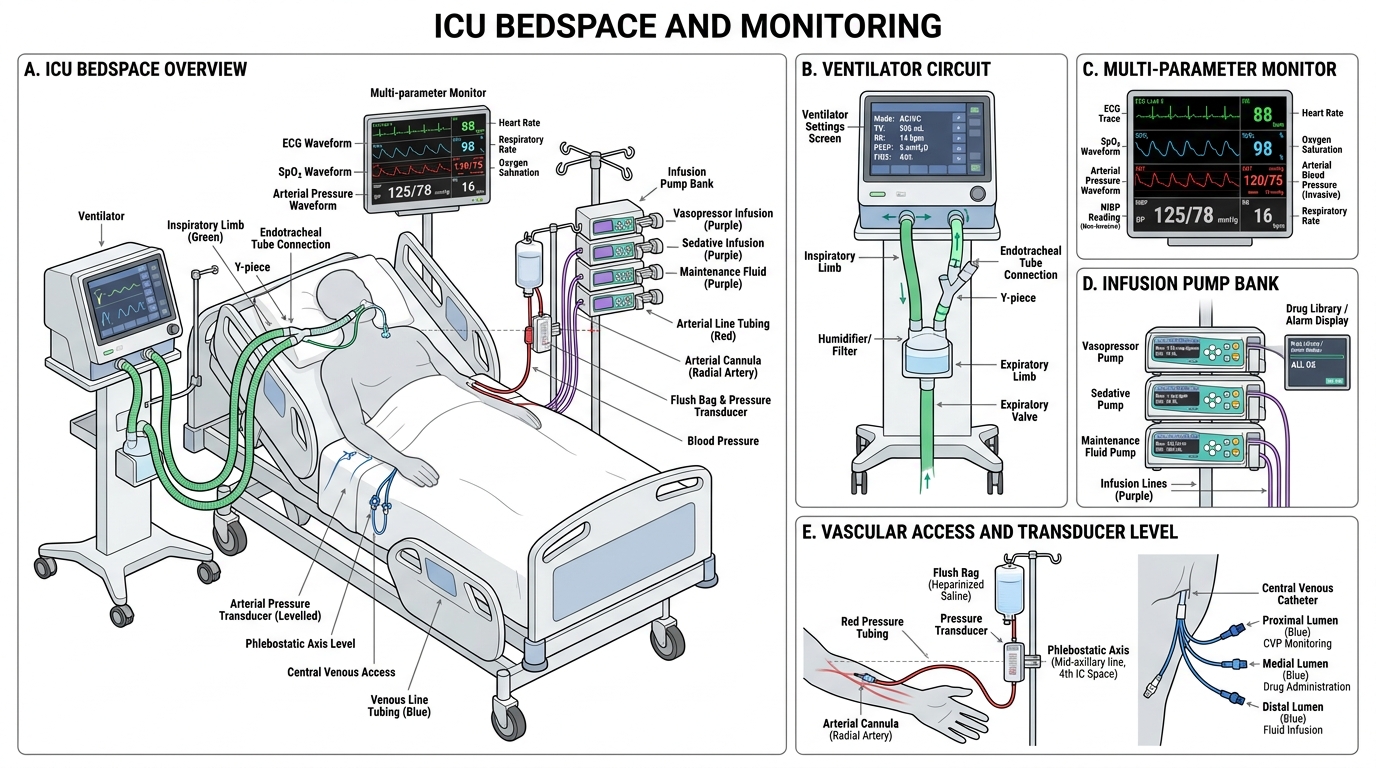
Single ICU Bedspace: Essential Equipment and Vascular Access
ICU Staffing: The Multidisciplinary Team and Its Functions
The staffing model of an ICU is multidisciplinary by design, because no single professional discipline can provide all the competencies critical care demands. At the core is the consultant intensivist (typically an anaesthesiologist, pulmonologist, or physician with intensive care specialty training), who bears overall clinical responsibility for ICU patients, leads daily ward rounds, drives therapeutic decision-making, and represents the team in family meetings. The intensivist is supported by a resident medical officer (RMO) or critical-care fellow on duty at all times, responsible for immediate clinical response, procedural support, and initial management of deterioration. Nursing is the numerically largest component of the ICU team: international standards recommend a minimum nurse-to-patient ratio of 1:1 for ventilated or haemodynamically unstable patients and 1:2 for stable monitored patients; Indian ISCCM guidelines currently recommend a minimum 1:2 ratio with a target of 1:1 for critical cases. Specialist respiratory therapists or physiotherapists manage ventilator weaning protocols, pulmonary rehabilitation, and secretion clearance. The clinical pharmacist embedded in the ICU team reviews medication appropriateness, checks for drug interactions, adjusts doses for renal and hepatic impairment, and oversees antimicrobial stewardship. Dietitians calculate caloric targets, design enteral and parenteral nutrition regimens, and monitor metabolic tolerance. Infection control nurses enforce hand-hygiene protocols, surveillance of healthcare-acquired infections, and care bundle compliance (central-line bundle, ventilator bundle). This multidisciplinary team gathers daily in a structured ICU ward round, during which each patient's 24-hour events, monitoring data, laboratory results, imaging, and therapeutic targets are reviewed systematically.
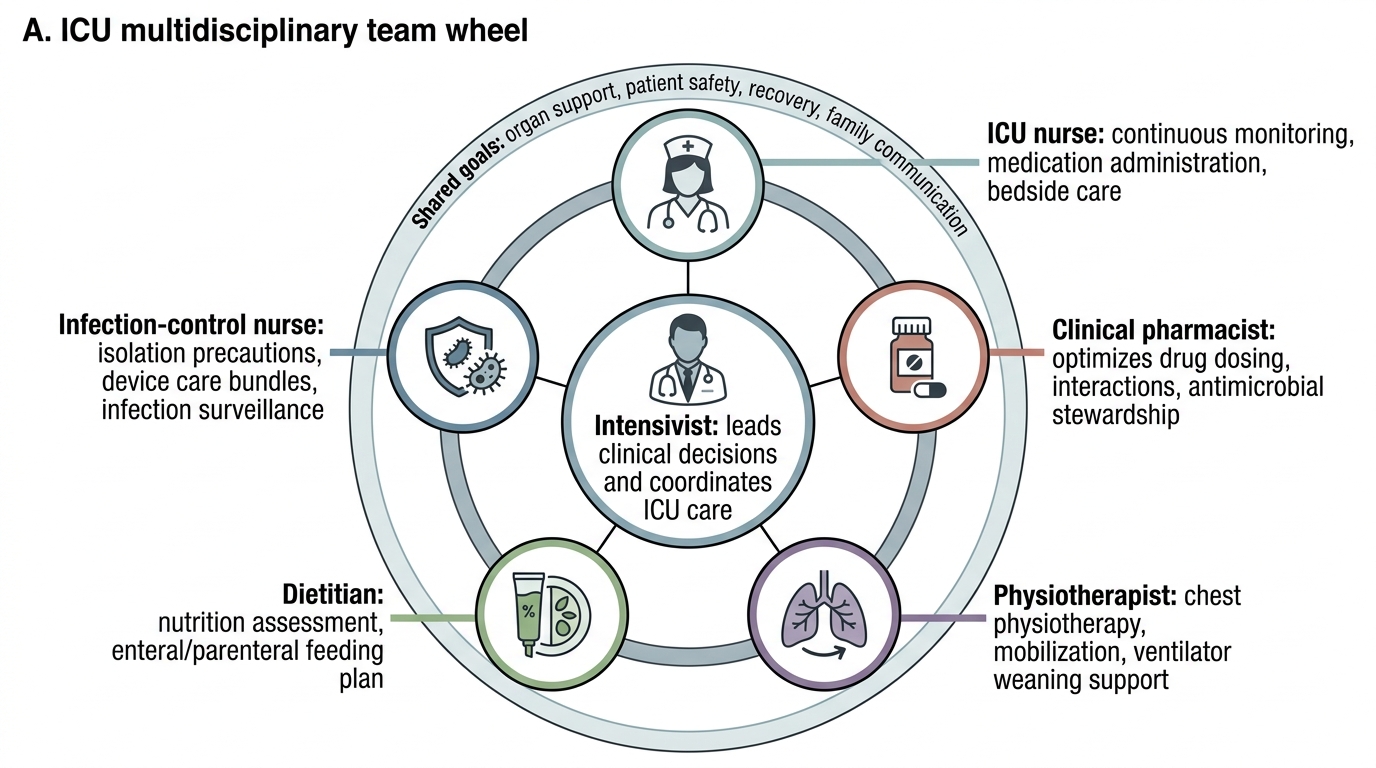
ICU Multidisciplinary Team Wheel