Page 2 of 13
AS7.1-2 | ICU Organization, Functions and Admission-Discharge Criteria — SDL Guide (Part 2)
ICU Equipment and Monitoring Capabilities: Physiological Basis for Organ Support
Understanding the physiological rationale behind each ICU intervention helps clinicians recognise why particular equipment is essential and what limitations exist. The cornerstone of ICU therapy is mechanical ventilation: patients with respiratory failure — defined by PaO2/FiO2 (P/F) ratio below 200 (Berlin ARDS criteria) or ventilatory failure with rising PaCO2 and respiratory acidosis — require positive-pressure mechanical support because the work of breathing is unsustainable. Volume-controlled ventilation delivers a fixed tidal volume per breath, while pressure-controlled ventilation delivers flow until a target pressure is reached; the lung-protective strategy for ARDS (tidal volume 6 mL/kg ideal body weight, plateau pressure 30 cmH2O or less, PEEP titrated to oxygenation) is grounded in avoiding ventilator-induced lung injury (VILI) from overdistension and repetitive alveolar collapse. Haemodynamic monitoring extends from non-invasive (NIBP, ECG, SpO2) to invasive: the arterial line (radial or femoral) provides beat-to-beat blood pressure waveform and an arterial blood gas sampling port; the central venous catheter (internal jugular, subclavian, femoral) provides central venous pressure (CVP) measurement and a high-flow conduit for vasopressors and concentrated electrolyte solutions. Modern ICUs increasingly use point-of-care ultrasonography (POCUS) and less-invasive cardiac output monitors (FloTrac/Vigileo, PiCCO based on pulse-contour analysis) for dynamic haemodynamic assessment. Renal replacement therapy (CRRT or intermittent haemodialysis) supports patients in acute kidney injury with volume overload, dangerous electrolyte derangement, or uraemic encephalopathy; continuous techniques (CVVHDF, CVVHF) are preferred in haemodynamically unstable patients because the slower solute and volume removal rate avoids the hypotensive episodes that complicate intermittent dialysis. Enteral nutrition delivered via nasogastric or nasojejunal tube is preferred over parenteral nutrition to preserve gut mucosal integrity and the intestinal microbiome, reducing bacterial translocation and systemic sepsis risk.
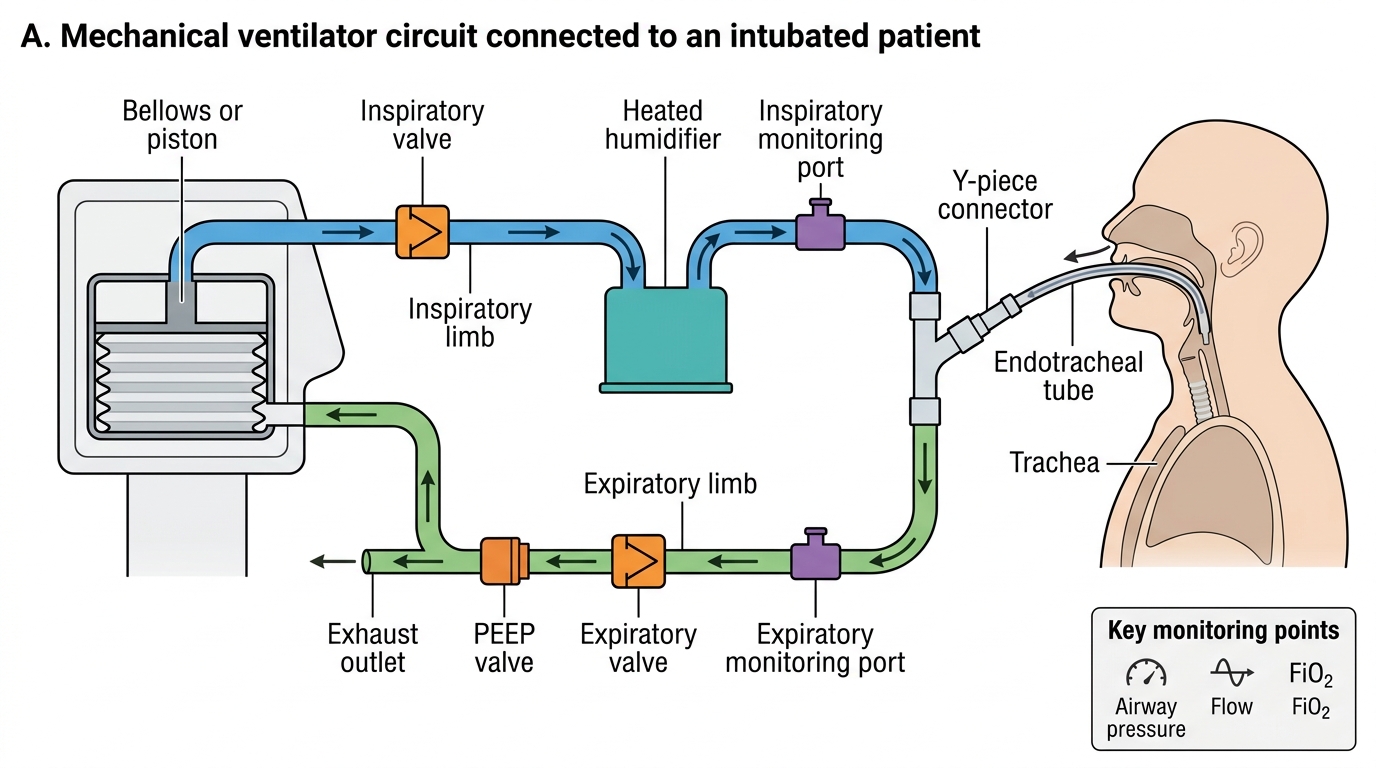
Mechanical Ventilator Circuit Components
SELF-CHECK
A ventilated ARDS patient has a PaO2 of 65 mmHg on FiO2 0.8. What is the P/F ratio and how does it classify this patient under Berlin ARDS criteria?
A. P/F = 81 mmHg; severe ARDS (P/F < 100)
B. P/F = 81 mmHg; moderate ARDS (P/F 100-200)
C. P/F = 52 mmHg; severe ARDS (P/F < 100)
D. P/F = 52 mmHg; not ARDS — Berlin criteria use SpO2 not PaO2
Reveal Answer
Answer: A. P/F = 81 mmHg; severe ARDS (P/F < 100)
P/F ratio = PaO2 / FiO2 = 65 / 0.8 = 81.25 mmHg. Berlin ARDS criteria classify: mild P/F 200-300, moderate P/F 100-200, severe P/F < 100. This patient's P/F of 81 is below 100, placing them in the severe ARDS category. The Berlin criteria specify PaO2 (arterial partial pressure of oxygen), not SpO2.
ICU Admission Criteria: Assessment Framework and Decision-Making
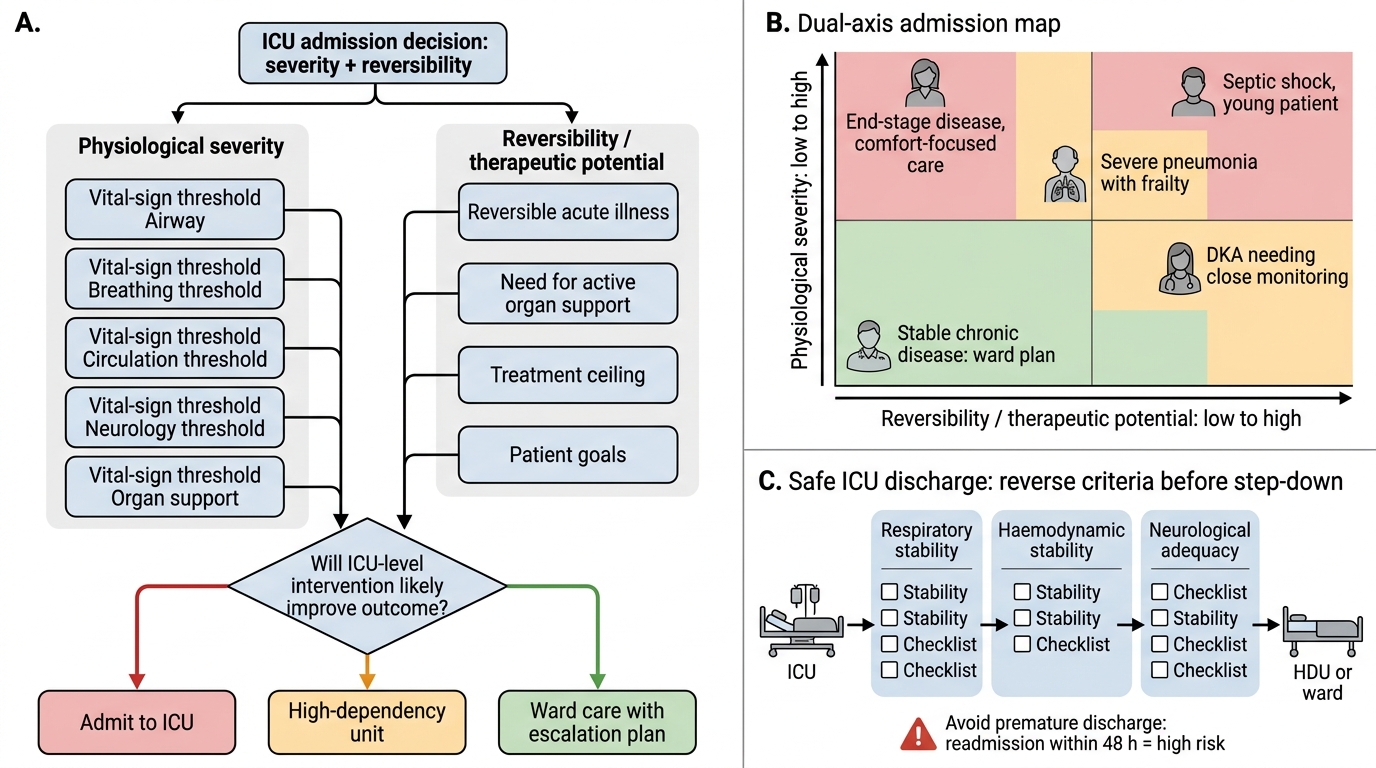
The decision to admit a patient to the ICU is one of the most consequential in acute medicine, because it determines resource allocation, patient trajectory, and family expectations. ICU admission criteria are grounded in two complementary axes: severity of current physiological derangement and reversibility or therapeutic potential of the underlying condition. A patient who is physiologically deranged but has an irreversible terminal condition may not benefit from ICU admission; conversely, a patient with apparently mild acute illness but high risk of rapid deterioration (e.g. post-cardiac surgery, anaphylaxis resolving, acute epiglottitis) warrants ICU-level monitoring. In India, ISCCM guidelines provide the operational reference framework.
Objective physiological criteria for ICU admission include any of the following: respiratory rate persistently above 35 breaths/min or below 6 breaths/min; SpO2 below 90% on supplemental oxygen at 6 L/min or more; systolic blood pressure below 90 mmHg unresponsive to initial fluid challenge; heart rate above 150 bpm or below 40 bpm; Glasgow Coma Scale (GCS) total score 8 or below or acute drop of 2 or more points from baseline; urine output below 0.5 mL/kg/h for 2 consecutive hours despite adequate fluid resuscitation; acute metabolic acidosis (pH below 7.20 with appropriate clinical context).
Disease-specific indications encompass: acute respiratory failure requiring mechanical ventilation; septic shock requiring vasopressor support (norepinephrine, vasopressin); acute myocardial infarction complicated by cardiogenic shock or lethal arrhythmia; post-operative care after major cardiovascular, thoracic, or neurosurgical procedures; severe head injury with GCS 8 or below; drug overdose with haemodynamic compromise or risk of airway loss; fulminant hepatic failure with hepatic encephalopathy grade III or IV; diabetic ketoacidosis with altered sensorium, severe acidosis (pH below 7.10), or electrolyte crisis.
ICU Admission and Safe Step-Down Decision Framework
ICU Discharge Criteria: Planning Safe Step-Down
Discharge from the ICU requires a structured assessment that the patient has both recovered sufficiently to be managed safely at a lower level of care AND that the receiving ward or step-down facility can meet the patient's residual monitoring and nursing needs. Premature discharge risks rapid deterioration and unplanned readmission — ICU readmission within 48 hours is associated with significantly higher mortality than index admissions. The physiological criteria for ICU discharge mirror the admission criteria in reverse.
Respiratory stability means the patient maintains adequate ventilation spontaneously or on low-level respiratory support (e.g. 4-6 L/min nasal prongs, FiO2 0.35 or less) with SpO2 of 95% or above on that support, respiratory rate 10-25 breaths/min, and no imminent extubation failure risk. Haemodynamic stability means mean arterial pressure (MAP) at or above 65 mmHg maintained without vasopressors for at least 4-6 hours, or on minimal vasopressor that a high-dependency unit can safely manage. Neurological adequacy requires GCS adequate for the patient's baseline (typically 12 or above unless premorbid GCS was lower), ability to protect the airway, and absence of active seizures. Metabolic stability means electrolytes within acceptable range, glucose controllable on sliding-scale insulin rather than continuous infusion, and arterial pH 7.30-7.45. Absence of active organ support means no ongoing CRRT that cannot be continued in a step-down setting.
In addition to objective criteria, the social and family readiness dimension matters: discharge planning should confirm that follow-up arrangements, family understanding of the post-ICU trajectory, and outpatient appointments are in place. Scoring tools such as the SOFA score, APACHE II, and MPM can assist but do not replace clinical judgment; no single score mandates ICU discharge.

ICU Admission vs Discharge Criteria by Organ System