Page 5 of 13
AS7.3-5 | Unconscious Patient Care, Ventilator Setup and ICU Monitoring — SDL Guide
Learning Objectives
- Describe the systematic management of an unconscious patient in the ICU, including airway, positioning, nursing care, and complication prevention
- Describe the basic setup process of a mechanical ventilator including mode selection, initial settings, and alarm configuration
- Describe the principles of monitoring in the ICU covering cardiovascular, respiratory, neurological, renal, and metabolic parameters
INSTRUCTIONS
Caring for an unconscious patient and operating a mechanical ventilator are foundational competencies for any doctor working in or rotating through an ICU. This module takes you through the systematic assessment and management of unconscious patients, the physiological logic behind ventilator settings, and the integrated monitoring framework that guides every ICU decision.
References
- Morgan & Mikhail's Clinical Anesthesiology, 6th ed., Chapters 57-58: Critical Care and Mechanical Ventilation (textbook)
- Ajay Yadav's Short Textbook of Anaesthesia, Chapters on Unconscious Patient and Monitoring (textbook)
- Paul G. Barash et al., Clinical Anesthesia, 8th ed., Section on ICU Monitoring and Ventilator Management (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 3 AM in the ICU. The nurse calls you to the bedside of a 42-year-old ventilated patient who had a stroke 18 hours ago. The high-pressure alarm on the ventilator is sounding, SpO2 has dropped to 88%, and the patient is beginning to posture abnormally. You have 60 seconds to identify whether this is a ventilator problem, a patient-airway problem, or a neurological deterioration — and act appropriately. Every skill in this module was written for exactly this moment.
WHY THIS MATTERS
The unconscious patient cannot protect themselves, cannot communicate distress, and cannot cooperate with examination. Their survival depends entirely on the vigilance and systematic competence of the clinical team. For any doctor rotating through medicine, surgery, emergency, or anaesthesia, encountering a ventilated unconscious patient is not exceptional — it is routine. Understanding ventilator setup and ICU monitoring is therefore not a subspecialty luxury but a core clinical skill that every graduating MBBS doctor must possess.
RECALL
Recall from earlier modules: the anatomy of the upper airway (nose, mouth, pharynx, larynx, epiglottis, vocal cords, trachea), the physiology of breathing (Boyle's law and pressure-volume relationships, the role of surfactant, functional residual capacity, compliance and resistance), the principles of pulse oximetry (SpO2 reads oxyhaemoglobin saturation, not PaO2 directly), and the Glasgow Coma Scale components (E1-4, V1-5, M1-6, total 3-15). Also recall the concept of a nursing care bundle — systematic checklists that reduce complication rates — from the ICU Organization module.
The Unconscious Patient: Clinical Context and Causes
An unconscious patient in the ICU is defined as one with a Glasgow Coma Scale score of 8 or below — the internationally recognised threshold below which the patient cannot reliably protect their own airway by closing the glottis against aspiration. The range of conditions producing ICU-level unconsciousness is broad: structural brain pathology (ischaemic stroke, haemorrhagic stroke, traumatic brain injury, cerebral oedema, space-occupying lesion); metabolic encephalopathy (hepatic encephalopathy, hypo- or hyperglycaemia, uraemic encephalopathy, hyponatraemia, thiamine deficiency); toxic causes (drug overdose with opioids, benzodiazepines, organophosphates, alcohol); anoxic brain injury (post-cardiac arrest); infectious causes (bacterial or viral meningitis, encephalitis, cerebral malaria); and post-ictal or status epilepticus. Identifying the underlying cause directs both the immediate management (e.g. naloxone for opioid overdose, glucose 25 g IV for hypoglycaemia, mannitol for acute cerebral oedema) and the anticipated recovery trajectory. The clinical context of the unconscious patient also determines the required monitoring intensity: a post-cardiac-arrest patient requires continuous EEG and targeted temperature management; a metabolic encephalopathy patient may recover fully with cause correction alone. The anaesthesiologist's role in managing the unconscious patient spans airway security, ventilatory support, haemodynamic optimisation, and neurological protection — a comprehensive management package rather than a single intervention.
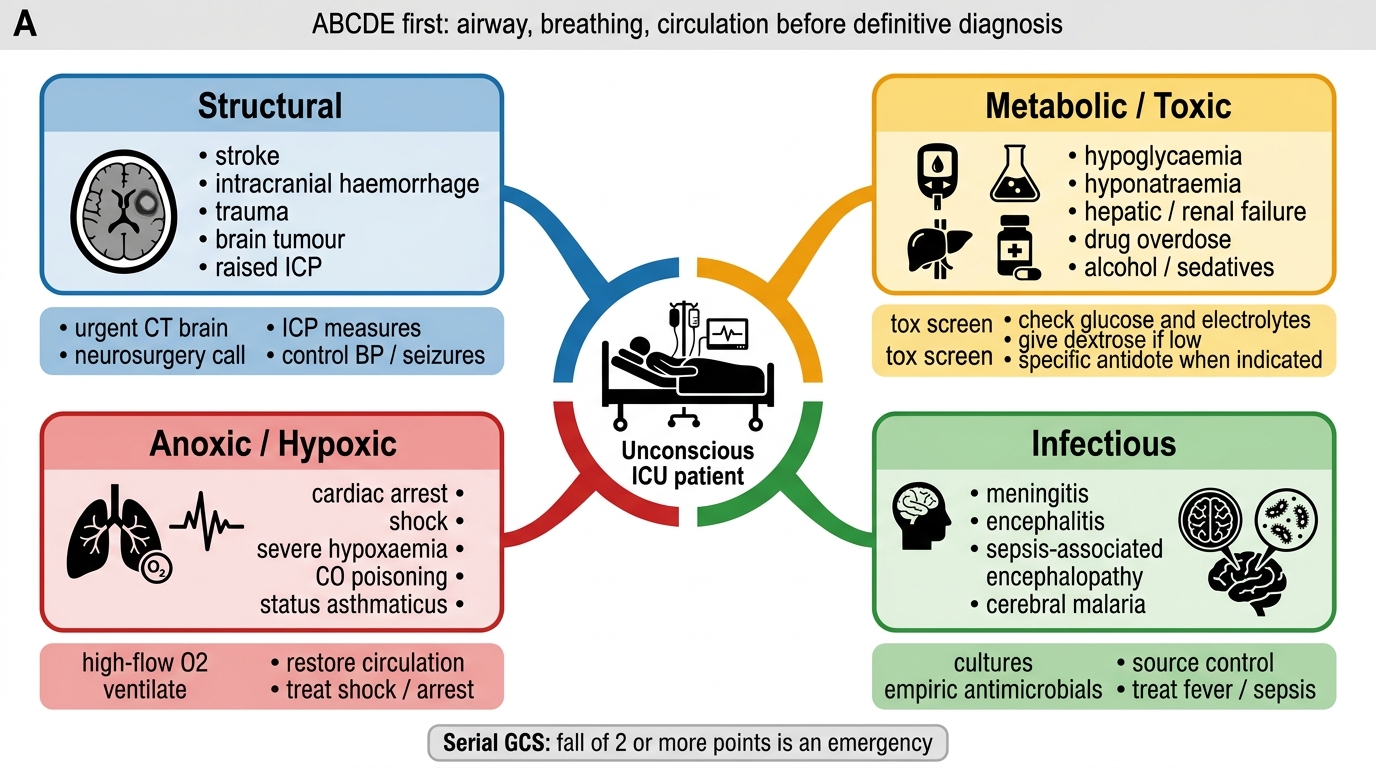
Causes of Unconsciousness in ICU
Management of the Unconscious Patient: Systematic Approach
The management of an unconscious patient follows the ABCDE framework in sequence, ensuring that life-threatening threats are addressed in the correct priority order before moving to secondary concerns. Airway: The unconscious patient with GCS 8 or below requires a definitive airway — an endotracheal tube (ETT) or tracheostomy — because passive loss of pharyngeal tone causes posterior tongue displacement, upper airway obstruction, and aspiration risk. In the interim, positioning the patient in the lateral decubitus (recovery) position partially opens the airway by allowing the tongue to fall away from the posterior pharyngeal wall; this is the standard first aid position for any unconscious patient who is not yet intubated. Breathing: Once intubated, mechanical ventilation settings are initiated (see next section). Circulation: Continuous haemodynamic monitoring is essential; neurological injury frequently causes secondary cardiovascular instability (neurogenic stunned myocardium in subarachnoid haemorrhage, Cushing's reflex — hypertension with bradycardia and irregular breathing — in raised intracranial pressure). Disability (Neurological): Serial GCS assessment is mandatory; a drop of 2 or more GCS points is a clinical emergency requiring urgent re-evaluation. Exposure: The unconscious patient cannot report pain or detect the early signs of pressure injury, urinary retention, or aspiration; regular exposure and systematic head-to-toe examination every 4-8 hours is essential.
Nursing care of the unconscious patient encompasses a specific bundle of evidence-based interventions: eye care (corneal drying from absent blinking causes exposure keratitis — eyes must be kept moist with lubricant drops or artificial tear gel, and taped closed during sleep); oral care (2-hourly mouth cleaning with chlorhexidine 0.12% to prevent VAP and oral candidiasis); pressure area care (2-hourly repositioning using a turn schedule to prevent pressure sores over sacrum, heels, and occiput; pressure-relieving mattress); catheter care (urinary catheter with strict aseptic maintenance to prevent catheter-associated urinary tract infection, CAUTI); DVT prophylaxis (low-molecular-weight heparin subcutaneously once daily plus graduated compression stockings or intermittent pneumatic compression where bleeding risk is acceptable).
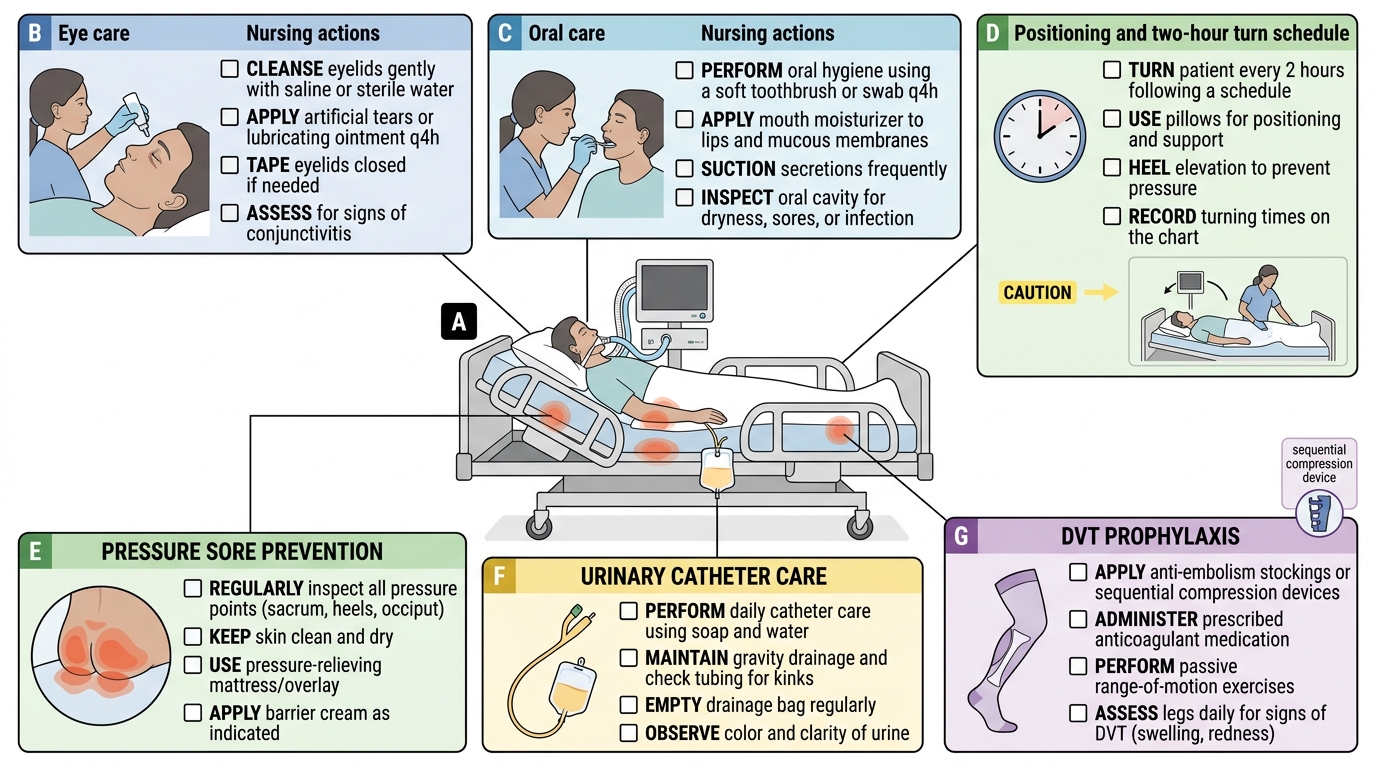
Nursing Care Checklist for the Unconscious ICU Patient
Mechanical Ventilator: Physiological and Pharmacological Basis
A mechanical ventilator replicates the pressure-volume relationship of normal breathing by generating positive pressure at the airway opening during inspiration, which drives gas into the lungs; during expiration, the chest wall and lung elastic recoil expel gas passively. This is the reverse of normal spontaneous breathing, where the diaphragm and external intercostals create a negative intrapleural pressure that draws air in. Understanding this reversal is fundamental: positive-pressure ventilation increases intrathoracic pressure during inspiration, which can reduce venous return to the right heart (decreased cardiac preload) and potentially reduce cardiac output — a haemodynamic consequence that must be anticipated and managed, particularly in hypovolaemic or right-heart-compromised patients. The physiological targets of mechanical ventilation are: adequate oxygenation (SpO2 94-98% or PaO2 60-80 mmHg in most patients; a higher SpO2 target may worsen outcomes in some contexts — hyperoxia causes pulmonary vasoconstriction and oxidative injury); adequate ventilation (elimination of CO2 to maintain arterial pH 7.35-7.45 and PaCO2 35-45 mmHg, unless deliberate hypercapnia is used in severe ARDS permissive hypercapnia); and lung protection (avoiding overdistension of recruited alveoli and avoiding cyclic opening and closing of collapsed alveoli — atelectrauma). The pharmacological context of ventilation encompasses sedation and analgesia, collectively termed SASH (Sedation, Analgesia, Safety, Humanisation in modern practice): opioids (morphine, fentanyl) provide analgesia and reduce the distress of breathing against the ventilator; benzodiazepines (midazolam, lorazepam) reduce ventilator dyssynchrony but are associated with ICU delirium and prolonged ventilation; propofol infusion provides titratable sedation for short-term ventilation; dexmedetomidine (alpha-2 agonist) produces sedation with preserved arousability and is associated with reduced delirium compared to benzodiazepines; neuromuscular blocking agents (NMBAs) (vecuronium, rocuronium, cisatracurium) are used short-term in severe ARDS or dyssynchrony but must never be given without adequate sedation as they cause paralysis without sedation, which is profoundly distressing.
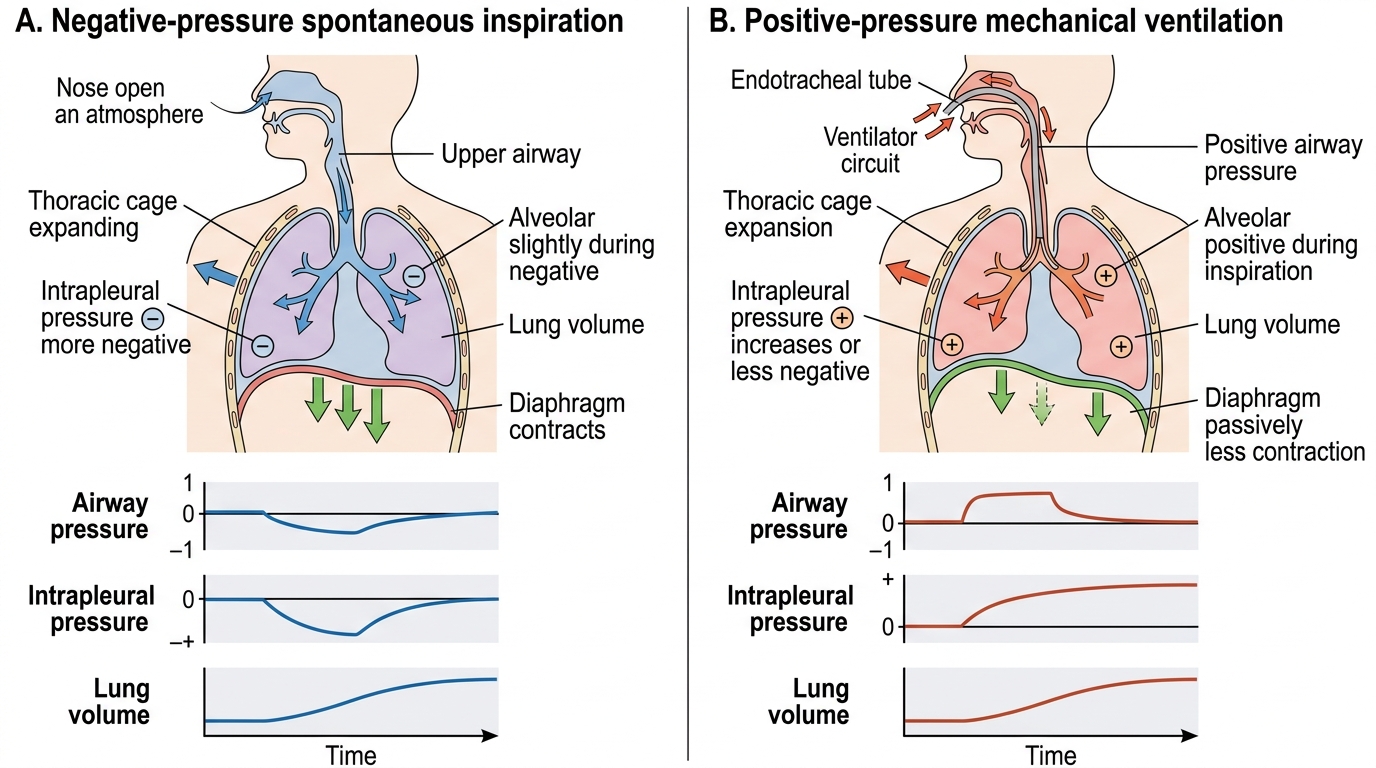
Spontaneous Breathing vs Positive-Pressure Ventilation