Page 6 of 16
AS8.3 | Pharmacologic Management of Pain — SDL Guide (Part 2)
Opioid Adverse Effects, Tolerance, Dependence, and Safe Prescribing
Competent opioid prescribing requires anticipatory management of the drug class's predictable adverse effects. Ignoring these while titrating dose is clinically dangerous; over-cautious dose restriction because of feared adverse effects leaves patients in avoidable pain. Safe prescribing balances both risks.
Respiratory depression is the most feared opioid adverse effect and the principal cause of opioid-related fatality. μ receptor activation in the pre-Bötzinger complex of the medulla reduces the central respiratory drive's sensitivity to CO₂ — the hypercapnic ventilatory response is blunted. Risk is highest when opioids are combined with other CNS depressants (benzodiazepines, alcohol, gabapentinoids), in opioid-naïve patients, in elderly or compromised patients (low body weight, renal impairment), and during sleep. Management: if opioid toxicity is suspected (pinpoint miosis, decreased respiratory rate <8/min, reduced consciousness), administer naloxone 0.4 mg IV, titrated to effect in 0.1 mg increments (to avoid precipitating acute pain and agitation by over-reversal); repeat every 2–3 minutes if needed. Naloxone's half-life (60–90 minutes) is shorter than most opioids — repeated doses or a naloxone infusion may be needed.
Constipation — unlike most other opioid effects — does not undergo tolerance. μ receptors in the enteric nervous system reduce peristaltic coordination and increase sphincter tone. All patients on regular opioids must be prescribed a stimulant laxative (e.g., senna, bisacodyl) co-currently. Bulk-forming laxatives are insufficient. Methylnaltrexone and naloxegol are peripherally restricted opioid antagonists available for opioid-induced constipation that is refractory to standard laxatives — they do not cross the blood-brain barrier and therefore do not reverse analgesia.
Nausea and vomiting occur in 25–40% of patients, mediated by opioid action at the chemoreceptor trigger zone (CTZ) in the area postrema and vestibular apparatus. Antiemetics (ondansetron, metoclopramide, cyclizine) are effective. Nausea typically undergoes tolerance within 3–5 days of regular dosing.
Sedation is common, particularly in opioid-naïve patients. Assess using the Sedation Scale (0 = alert; 1 = mild, occasionally drowsy; 2 = moderate, frequently drowsy; 3 = severe, difficult to rouse). A score of 3 warrants opioid dose reduction and clinical review. Sedation and cognitive impairment also undergo partial tolerance.
Tolerance refers to the need for increasing doses to achieve the same analgesic effect, resulting from μ receptor downregulation, desensitisation, and compensatory upregulation of pro-excitatory mechanisms. Physical dependence refers to the physiological state in which abrupt discontinuation or antagonist administration precipitates a withdrawal syndrome (autonomic hyperactivity, agitation, diarrhoea, craving). Physical dependence does not equate to addiction (psychological compulsion to use despite harm) — a distinction critical for appropriate management of opioid-treated cancer and chronic non-cancer pain patients.
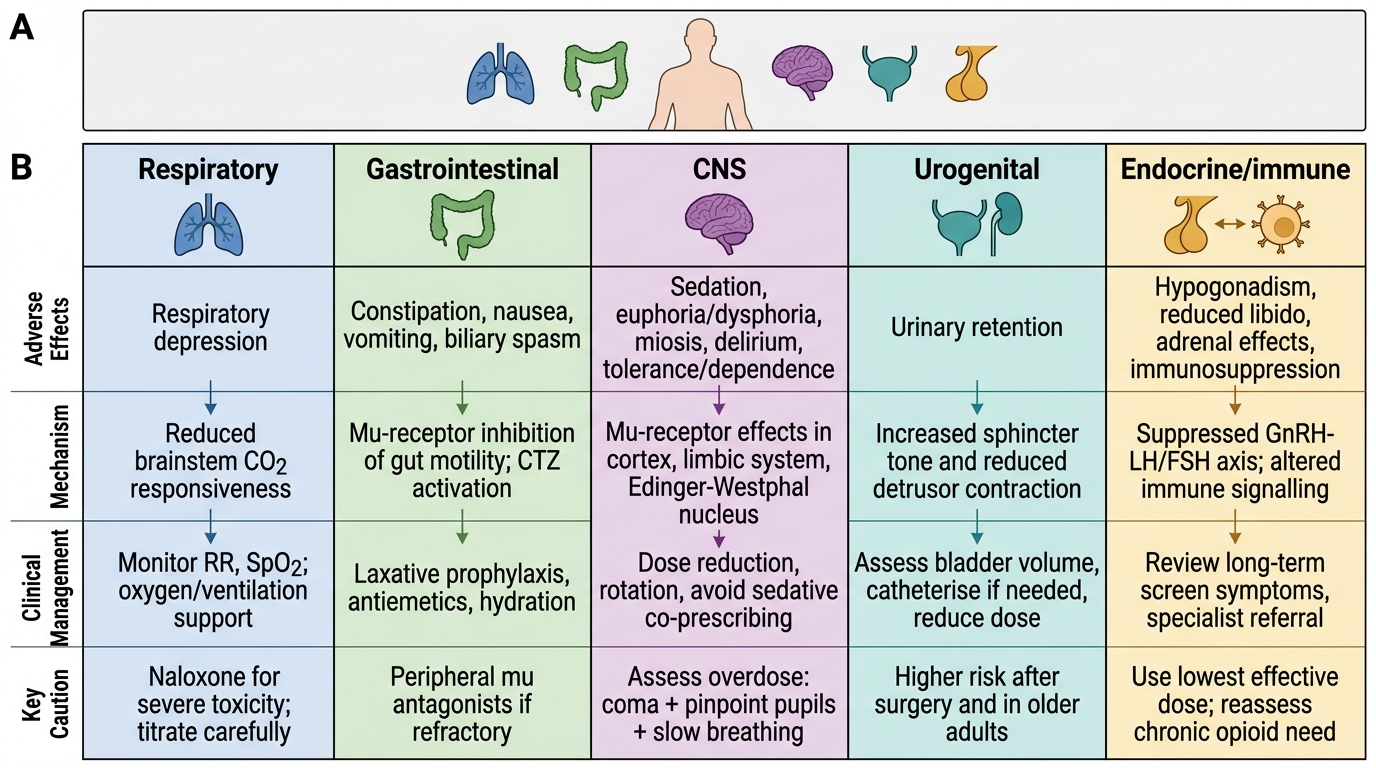
Opioid Adverse Effects by Organ System
Adjuvant Analgesics: Gabapentinoids, Antidepressants, and Other Agents
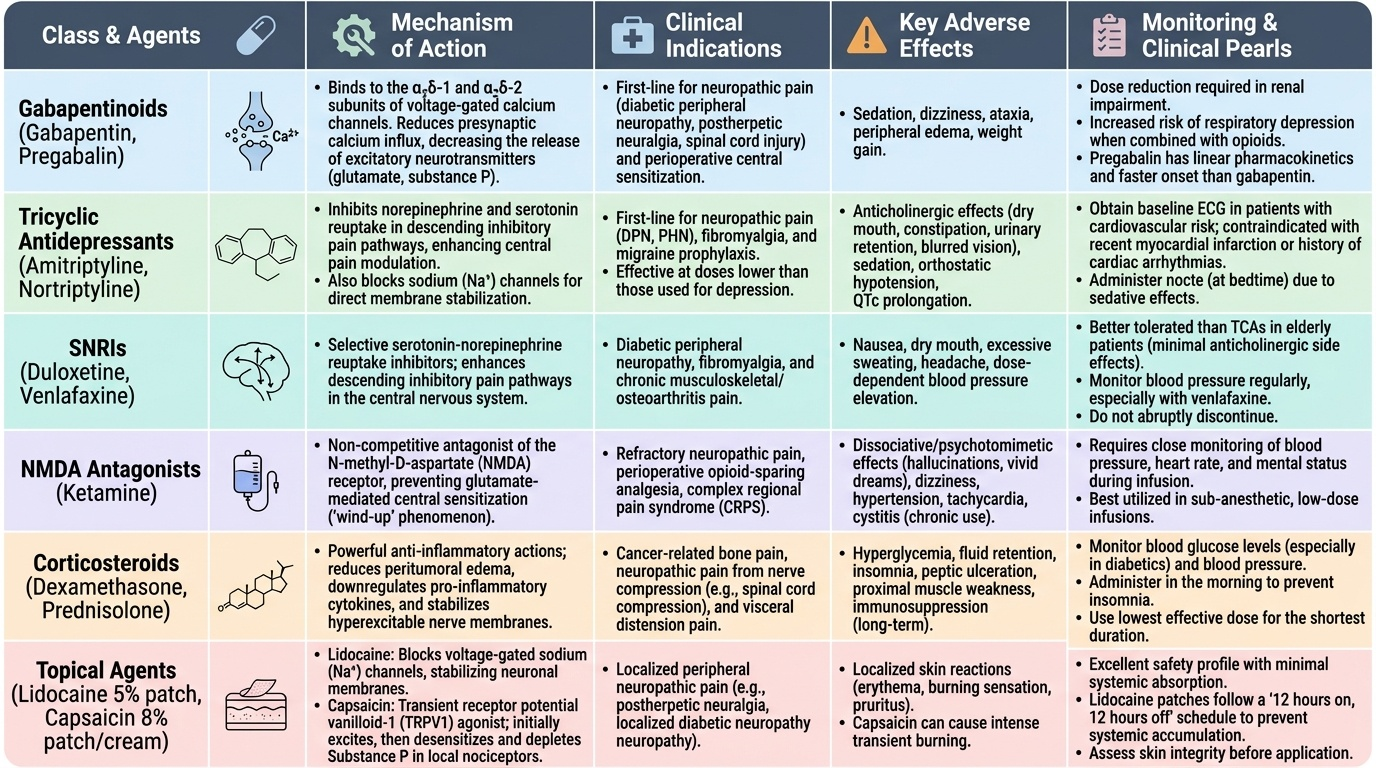
Adjuvant analgesics are drugs whose primary licensed indication is not pain management but which have evidence-based analgesic efficacy in specific pain syndromes. They are particularly valuable for neuropathic pain, which responds poorly to opioids alone, and as opioid-sparing agents in the perioperative setting.
Provided image
Gabapentinoids — gabapentin and pregabalin — are structural analogues of GABA that paradoxically do not act on GABA receptors. Their mechanism of analgesia involves binding to the α₂δ-1 and α₂δ-2 subunits of voltage-gated calcium channels, reducing calcium influx at presynaptic terminals of primary afferents and dorsal horn neurons, and thereby reducing glutamate and substance P release. They are first-line agents for neuropathic pain (diabetic peripheral neuropathy, postherpetic neuralgia, spinal cord injury pain) and are used perioperatively to reduce central sensitisation. Adverse effects: sedation, dizziness, ataxia, peripheral oedema, weight gain. Dose reduction required in renal impairment. Pregabalin has linear pharmacokinetics and a faster onset than gabapentin. Risk of respiratory depression is increased when combined with opioids — an important safety consideration in perioperative prescribing.
Tricyclic antidepressants (TCAs) — amitriptyline, nortriptyline — are first-line adjuvants for neuropathic pain. Their analgesic mechanism is independent of their antidepressant effect and operates at lower doses. They block norepinephrine and serotonin reuptake in descending inhibitory pathways, enhancing central pain modulation. Additional mechanisms include sodium channel blockade (direct membrane stabilisation). Amitriptyline 10–75 mg nocte is effective for diabetic neuropathy, postherpetic neuralgia, and migraine prophylaxis. Adverse effects: anticholinergic effects (dry mouth, constipation, urinary retention, blurred vision), sedation, orthostatic hypotension, cardiac arrhythmias (QTc prolongation — contraindicated with recent MI or arrhythmia history), weight gain.
Serotonin-norepinephrine reuptake inhibitors (SNRIs) — duloxetine, venlafaxine — are first-line for diabetic peripheral neuropathy and useful for fibromyalgia and chronic musculoskeletal pain. Better tolerated than TCAs in elderly patients; preferred when anticholinergic adverse effects are unacceptable.
Ketamine (sub-anaesthetic dose range 0.1–0.5 mg/kg/h IV infusion) is an NMDA receptor antagonist that interrupts wind-up and central sensitisation. Indicated perioperatively in opioid-tolerant patients, major surgeries with high chronic pain risk (thoracotomy, spinal surgery), and for opioid-refractory cancer pain. Adverse effects at sub-anaesthetic doses: dysphoria, hallucinations, tachycardia, hypertension, hypersalivation. Concurrent low-dose midazolam reduces psychomimetic effects.
Corticosteroids (dexamethasone, methylprednisolone) have analgesic effects in several contexts: reducing inflammatory oedema compressing neural structures (spinal cord compression, nerve root compression), palliative care for bone pain and visceral pain from tumour, and post-operative nausea and pain reduction. Dexamethasone 4–8 mg IV is a standard antiemetic-analgesic adjuvant for major surgery. Adverse effects with chronic use are extensive (immunosuppression, hyperglycaemia, adrenal suppression, osteoporosis, peptic ulceration) — short perioperative courses carry minimal risk.
Topical analgesics — lidocaine patches (5%), capsaicin cream (0.025–0.1%; 8% patch for postherpetic neuralgia) — provide localised relief for peripheral neuropathic pain syndromes with minimal systemic absorption.
SELF-CHECK
A 78-year-old woman with stage-IV ovarian cancer and moderate renal impairment (eGFR 28 mL/min) requires escalation of her opioid analgesia. She is currently on oral morphine 30 mg twice daily (modified-release). Her pain is 7/10 NRS. Which action is MOST appropriate?
A. Increase oral morphine to 45 mg twice daily — morphine is the safest strong opioid in renal failure
B. Switch to oral oxycodone 15 mg twice daily — oxycodone has no active metabolites
C. Switch to transdermal fentanyl 25 μg/h patch — fentanyl has no renally excreted active metabolites and is appropriate for stable severe pain
D. Add gabapentin 300 mg three times daily as the first dose-escalation step before increasing the opioid
Reveal Answer
Answer: C. Switch to transdermal fentanyl 25 μg/h patch — fentanyl has no renally excreted active metabolites and is appropriate for stable severe pain
In significant renal impairment (eGFR <30 mL/min), morphine accumulates its active metabolite morphine-6-glucuronide (M6G) — which is renally excreted and is 4–6 times more potent than morphine — risking prolonged sedation and respiratory depression. Oxycodone also has active renally-excreted metabolites (oxymorphone) and is not clearly safer than morphine in severe renal failure. Transdermal fentanyl is the preferred strong opioid in renal impairment: fentanyl is metabolised to inactive norfentanyl, does not accumulate renally, and the patch formulation provides stable plasma levels suitable for background pain. The equianalgesic dose of oral morphine 60 mg/24 h corresponds approximately to a 25 μg/h fentanyl patch — appropriate for this patient who was on 60 mg morphine/24 h and has inadequate control. Option D (gabapentin) would address neuropathic pain but is not a rational first step for dose escalation of background nociceptive cancer pain.
Multimodal Analgesia and Route of Administration
Multimodal analgesia — the simultaneous administration of two or more analgesics with different mechanisms of action — is the standard of care for perioperative pain management and is increasingly applied in chronic and cancer pain. The principle rests on additive or synergistic analgesic effects at multiple targets while dose-reducing each individual agent, thereby limiting the adverse effects associated with high doses of any single drug. The evidence base for this approach is compelling: randomised controlled trials consistently demonstrate that multimodal regimens produce superior pain control, earlier return of function, shorter hospital stays, and fewer opioid-related adverse events compared with single-agent approaches. The anaesthesiologist's role is not simply to prescribe a 'pain killer' but to engineer a comprehensive analgesic plan that addresses all active pain mechanisms — nociceptive, inflammatory, and neuropathic — across the full analgesic spectrum, from the periphery to the spinal cord to higher centres. Understanding which agents to combine, in what sequence, at what doses, and via which routes of administration is a core clinical skill that directly determines patient outcomes.
A standard multimodal regimen for post-operative major abdominal surgery exemplifies the approach:
- Paracetamol 1 g IV/oral every 6 hours (regularly, not as needed)
- Ketorolac 15 mg IV every 8 hours (if no contraindications) for the first 48–72 hours
- Epidural analgesia (local anaesthetic + low-dose opioid infusion) targeting the wound dermatomal level — provides the most effective post-operative pain control for thoracic and major abdominal surgery and also reduces the systemic opioid requirement by 50–70%
- IV morphine via patient-controlled analgesia (PCA): a demand dose of 1–2 mg with a lockout interval of 5–10 minutes; background infusion generally avoided in opioid-naïve adults (increases respiratory depression risk without improving analgesia)
- Gabapentin 300–600 mg on the night before surgery and for 48–72 hours post-operatively in patients at risk of chronic post-surgical pain
Route of administration principles: the oral route is always preferred once tolerated — bioavailability, patient control, avoidance of needle-related risks. Subcutaneous (SC) infusion via a syringe driver is the preferred route in palliative care when swallowing is impaired — diamorphine (where available) or morphine can be infused continuously with booster doses available on demand. Intramuscular (IM) injection is unreliable for analgesic dosing (variable absorption, particularly in low-perfusion states) and painful — avoid when SC or IV is available. Neuraxial routes (intrathecal or epidural opioids and/or local anaesthetics) produce profound segmental analgesia and are widely used perioperatively and in obstetric practice.
Patient-controlled analgesia (PCA) devices allow patients to self-administer a predetermined bolus dose within programmed safety limits. PCA respects pharmacokinetic variability between individuals (a dose that relieves pain in one patient may cause respiratory depression in another of identical weight) and empowers patients, improving satisfaction and reducing time to effective analgesia.