Page 3 of 8
AN20.1-10 | General Features, Joints, radiographs & surface marking (Lower Limb) — SDL Guide (Part 3)
Important Bony Landmarks of the Lower Limb
Palpate these on yourself as you read (AN20.7):

Figure: Important Bony Landmarks of the Lower Limb
Pelvis/Hip level:
- Highest point of iliac crest: L4 vertebral level (used for lumbar puncture landmark — iliac crest line)
- Posterior superior iliac spine (PSIS): Posterior dimples of Venus — at the level of S2 vertebra and the posterior end of the sacroiliac joint
- Iliac tubercle: 5 cm posterior to ASIS, at L5 level
- Pubic tubercle: Medial to the inguinal ligament origin; at the medial end. Spermatic cord in males passes superior to pubic tubercle. Femoral hernia passes inferior and lateral to it.
- Ischial tuberosity: The 'sitting bone' — palpable in the gluteal fold with hip flexed
- Adductor tubercle: Superior to medial femoral condyle — origin of adductor magnus
Knee level:
- Tibial tuberosity: Attachment of patellar ligament (L4 reflex — patellar reflex)
- Head of fibula: Lateral side below knee joint. Common peroneal nerve winds around its neck — vulnerable to injury (foot drop)
- Medial and lateral condyles of femur and tibia: Define the knee joint line
Ankle/Foot level:
- Medial malleolus: Distal end of tibia — tip is 1 cm higher than lateral malleolus
- Lateral malleolus: Distal end of fibula — 1 cm lower and more posterior than medial malleolus
- Sustentaculum tali: Shelf of calcaneus on its medial surface, 2.5 cm below medial malleolus — supports talus; FHL passes beneath it in a groove
- Tuberosity of 5th metatarsal: Base of 5th MT on lateral border of foot — peroneus brevis inserts here; avulsion fracture site in ankle sprains
- Tuberosity of navicular: Medial mid-foot — tibialis posterior inserts here; accessory navicular is a common variant
- Calcaneal tuberosity: Heel — plantar fascia and intrinsic foot muscles originate here
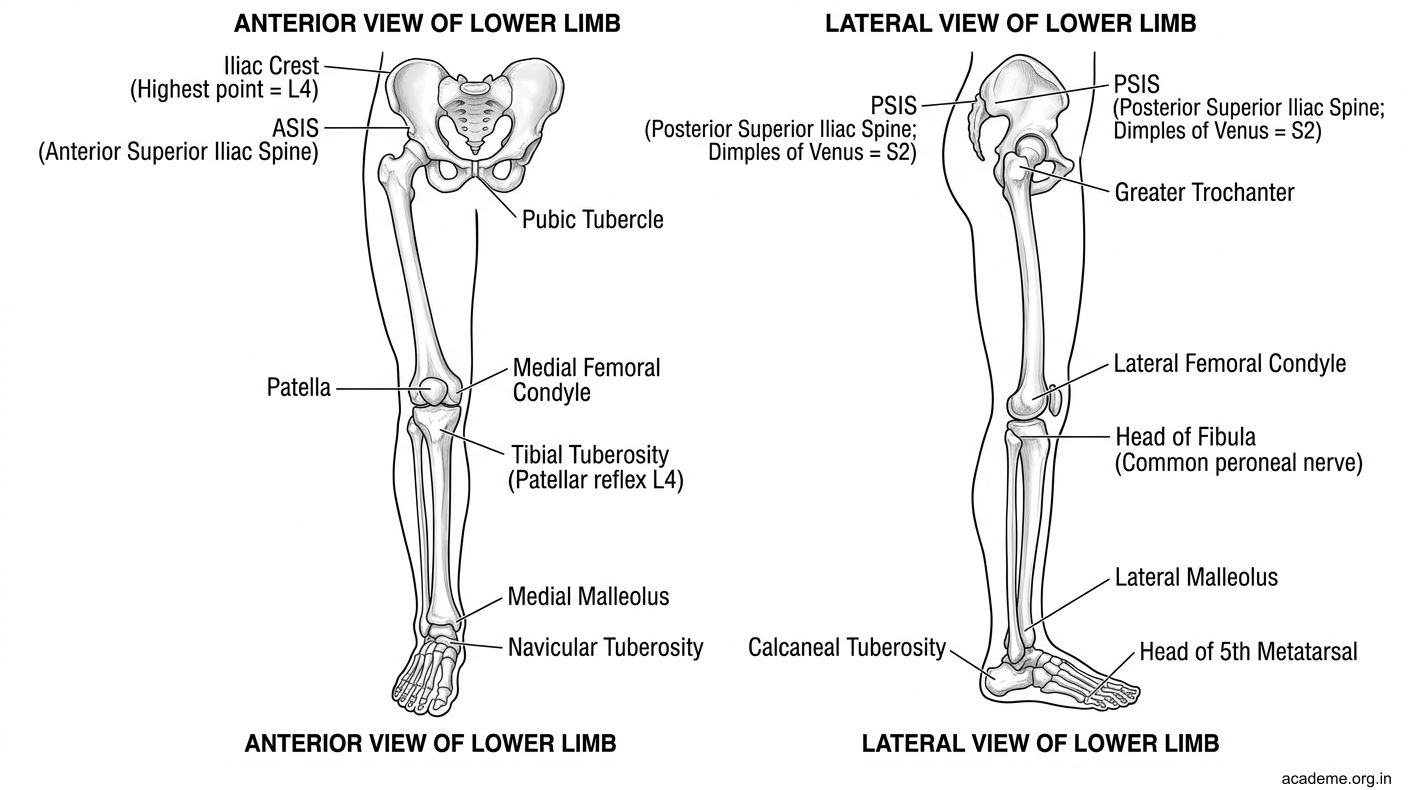
Figure: Important Bony Landmarks of the Lower Limb

Figure: Pelvis/Hip level
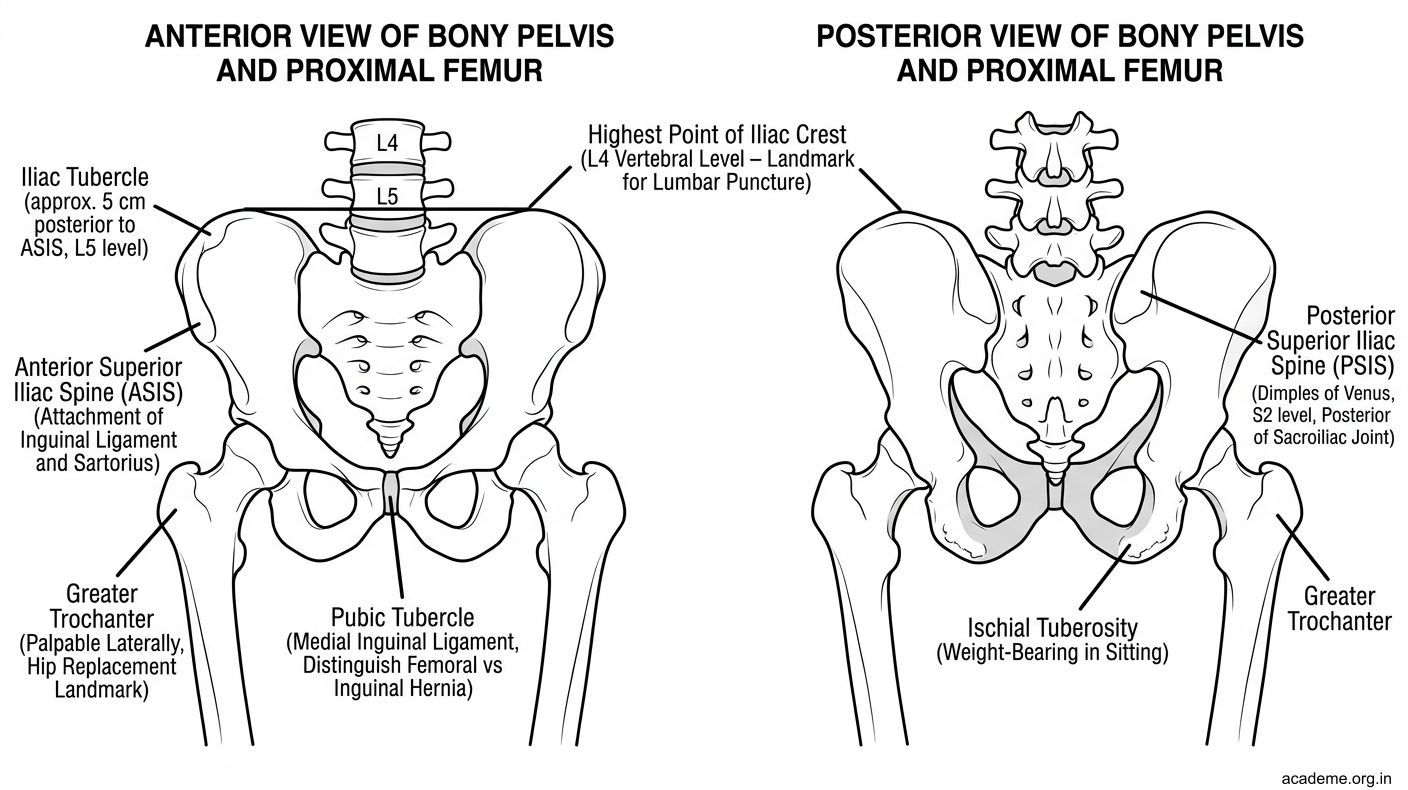
Figure: Pelvis/Hip level
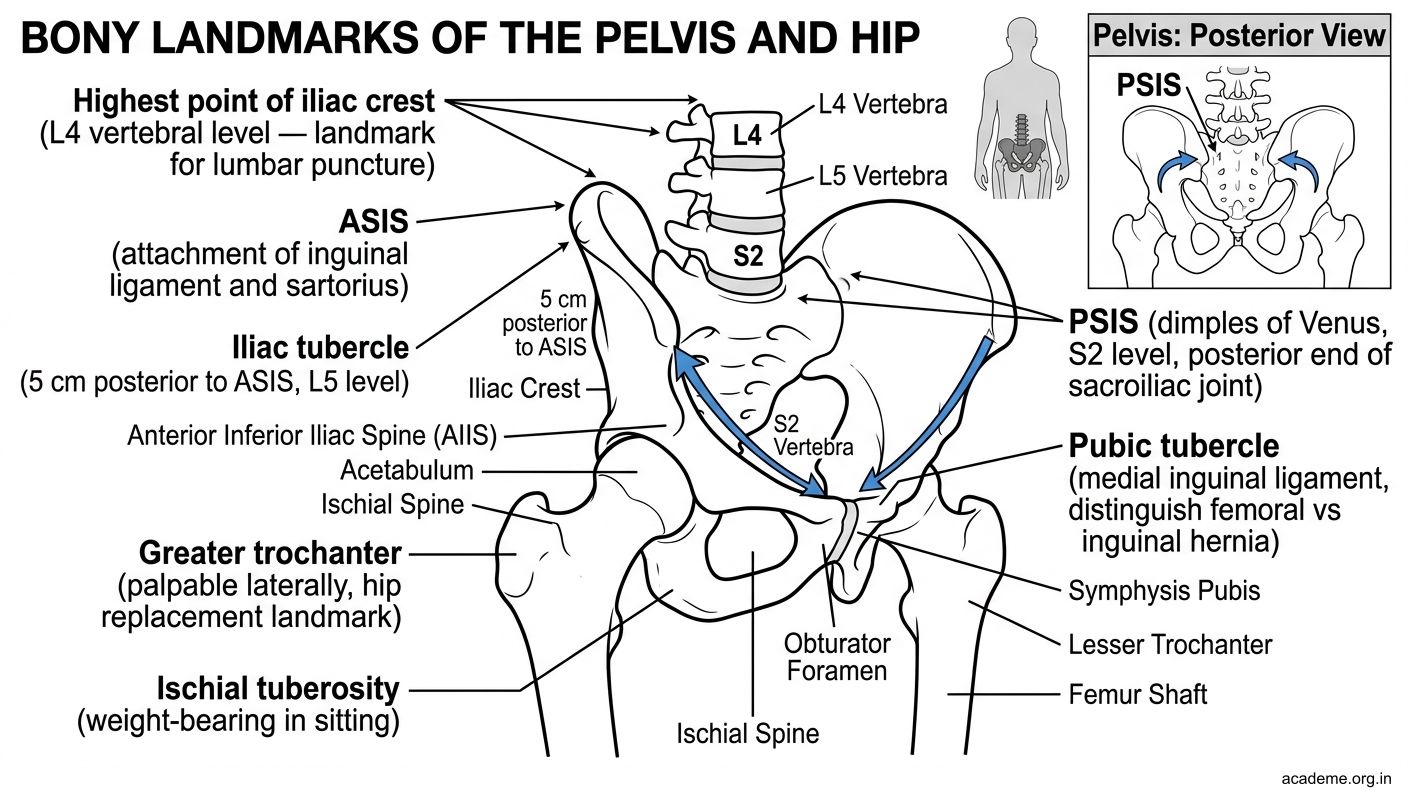
Figure: Pelvis/Hip level

Figure: Ankle/Foot level
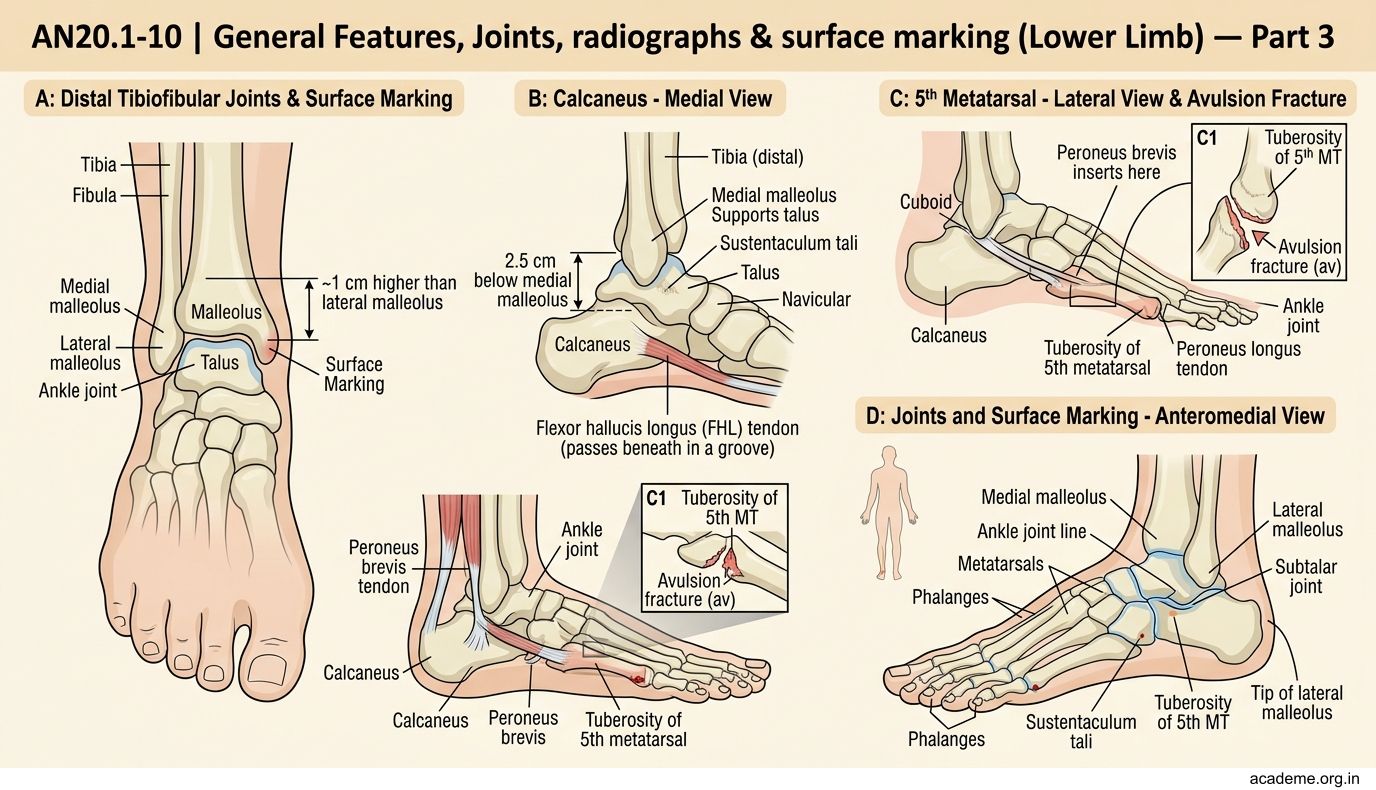
Figure: Ankle/Foot level
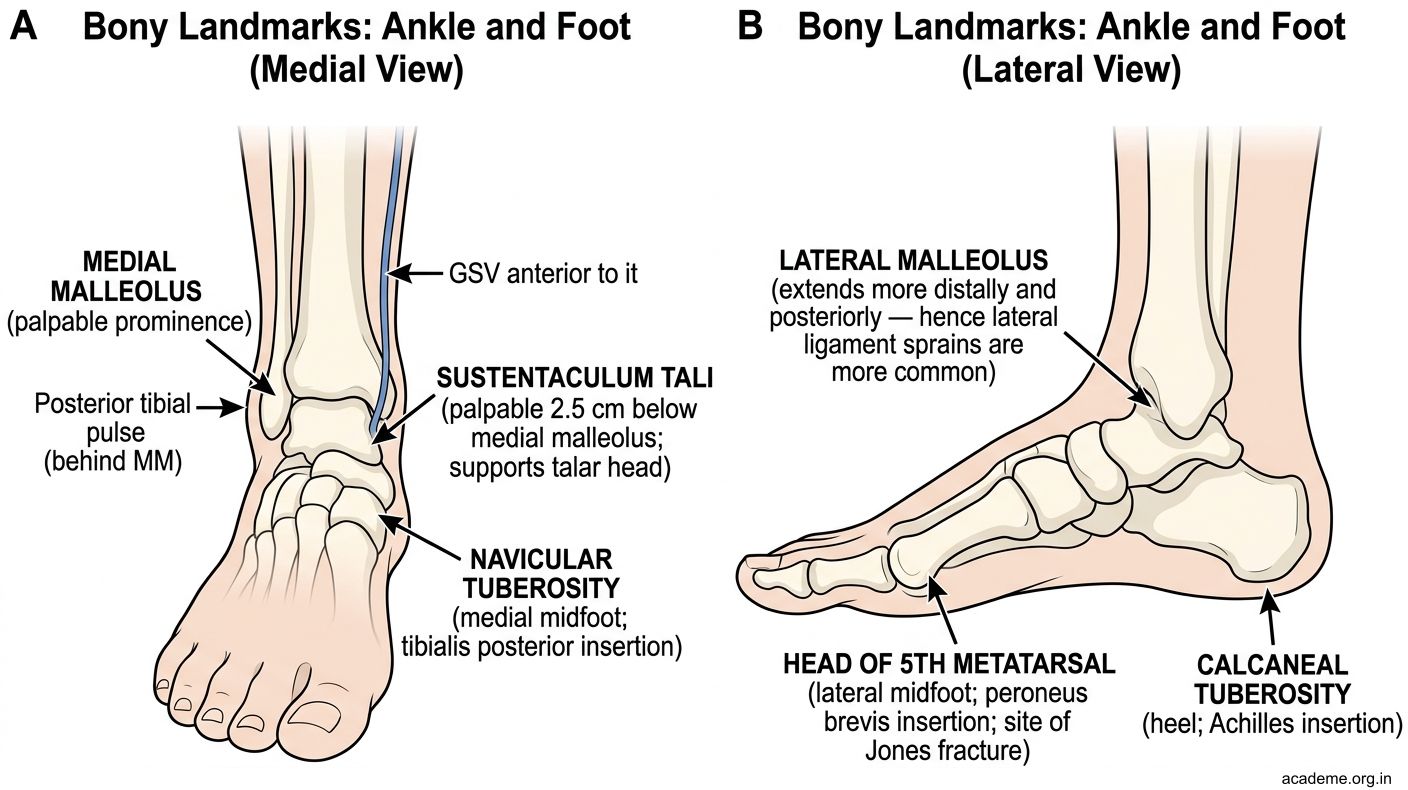
Figure: Ankle/Foot level
Surface Projection of Lower Limb Arteries
AN20.8 — Arterial Pulse Palpation (practice on your own leg)

Figure: Surface Projection of Lower Limb Arteries
1. Femoral Artery
- Surface marking: Mid-inguinal point (midpoint between ASIS and pubic symphysis) — the femoral artery enters the thigh here under the inguinal ligament
- Pulse palpation: Press firmly just below the inguinal ligament at the mid-inguinal point
- Clinical: Femoral artery cannulation for angiography, IABP insertion, cardiac catheterisation, CPR in PEA
- Note: Femoral vein is just medial to the artery; femoral nerve is just lateral
2. Popliteal Artery
- Surface marking: Deep in the popliteal fossa — runs from the adductor hiatus (junction of middle and lower thirds of femur) to the lower border of popliteus
- Pulse palpation: Knee slightly flexed, press fingers into the popliteal fossa and feel for the deep pulsation
- Hardest pulse to palpate; absent in Baker's cyst, popliteal artery entrapment syndrome
3. Anterior Tibial Artery
- Passes through the interosseous membrane near the proximal fibula to enter the anterior compartment
- Pulse palpation: On the dorsum of the foot as the dorsalis pedis artery — lateral to extensor hallucis longus tendon, between the 1st and 2nd metatarsals
4. Posterior Tibial Artery
- Pulse palpation: In the groove between medial malleolus and the Achilles tendon (posterior to medial malleolus)
5. Dorsalis Pedis
- Continuation of anterior tibial artery on the dorsum of the foot
- Palpation: Lateral to extensor hallucis longus tendon between 1st and 2nd metatarsals
- Absent in ~10% normal population (not always pathological)
- Critical for diabetic foot assessment: Compare both feet; absent dorsalis pedis + absent posterior tibial = critical ischaemia → risk of amputation
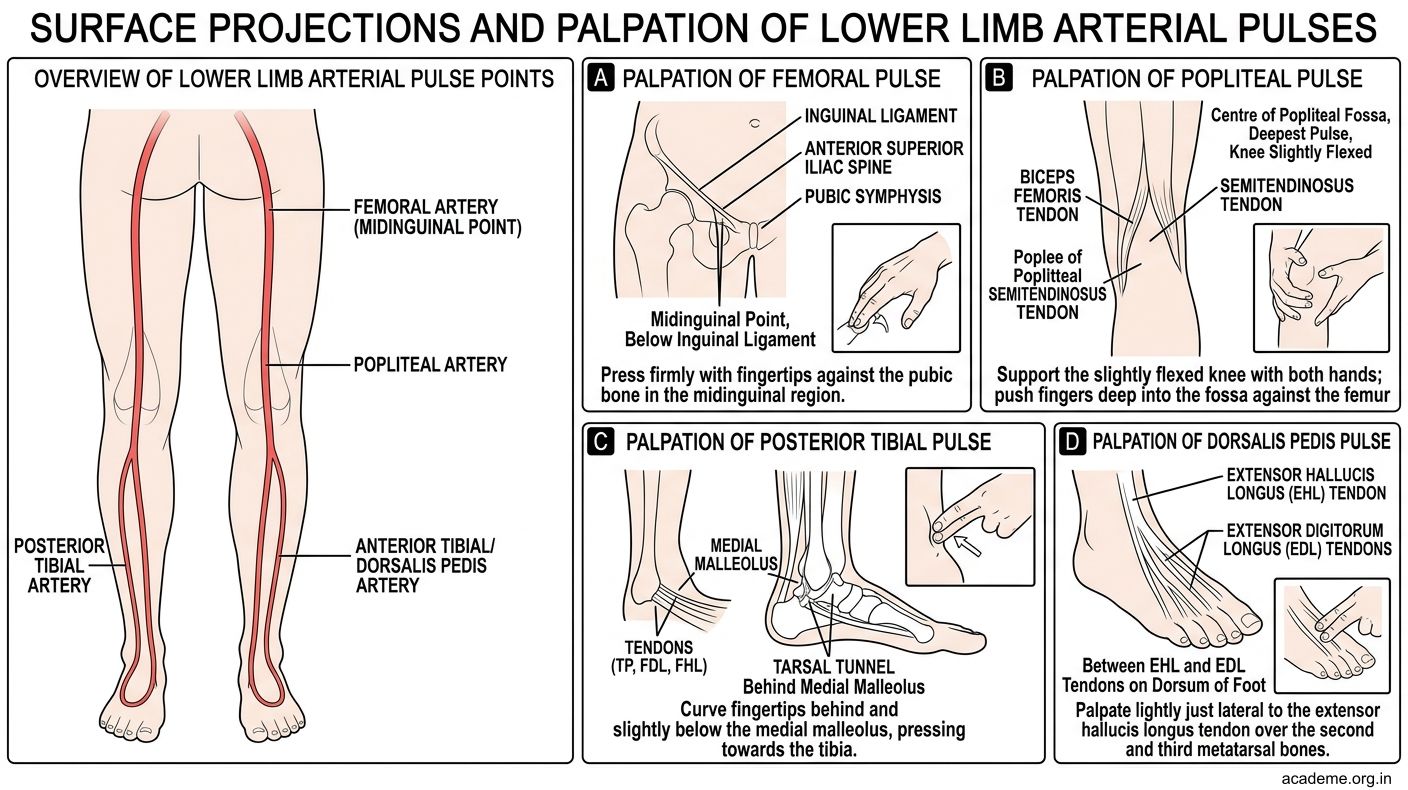
Figure: Surface Projection of Lower Limb Arteries
Surface Projection of Lower Limb Nerves & Veins
AN20.9 — Surface Projections

Figure: Saphenous Opening (Fossa Ovalis)

Figure: Small Saphenous Vein (SSV)

Figure: Great Saphenous Vein (GSV)

Figure: Common Peroneal Nerve

Figure: AN20.9 — Surface Projections
Femoral Nerve:
- Lateral to femoral artery at the mid-inguinal point
- Divides just below the inguinal ligament into multiple branches
- Saphenous nerve is its longest cutaneous branch — accompanies GSV, supplies medial leg/foot (L4)
- Femoral nerve block: Inject lateral to the femoral artery at the inguinal ligament — anaesthetises anterior thigh and knee
Sciatic Nerve:
- Exits the greater sciatic foramen below piriformis, midway between ischial tuberosity and greater trochanter
- Runs down the posterior thigh to the popliteal fossa where it bifurcates
- Sciatic nerve injection danger zone: Intramuscular injections in the gluteal region must be in the upper outer quadrant to avoid the sciatic nerve
Common Peroneal Nerve:
- Winds around the neck of the fibula (most superficial major nerve in the body at this point)
- Injury here → foot drop (loss of dorsiflexion, eversion; loss of sensation on dorsum of foot)
- Causes: Tight cast, prolonged crossing of legs, fibula neck fracture
Great Saphenous Vein (GSV):
- Anterior to medial malleolus → medial leg → posterior to medial femoral condyle → saphenous opening → femoral vein
- GSV cutdown: Classic emergency access site — anterior to medial malleolus (always present, predictable anatomy)
Small Saphenous Vein (SSV):
- Posterior to lateral malleolus → midline posterior leg → popliteal fossa → popliteal vein
Saphenous Opening (Fossa Ovalis):
- Oval deficiency in deep fascia, 4 cm below and lateral to pubic tubercle
- GSV drains into femoral vein here. Femoral hernia protrudes through the femoral canal (medial to femoral vein), covered by cribriform fascia, emerges below and lateral to pubic tubercle.
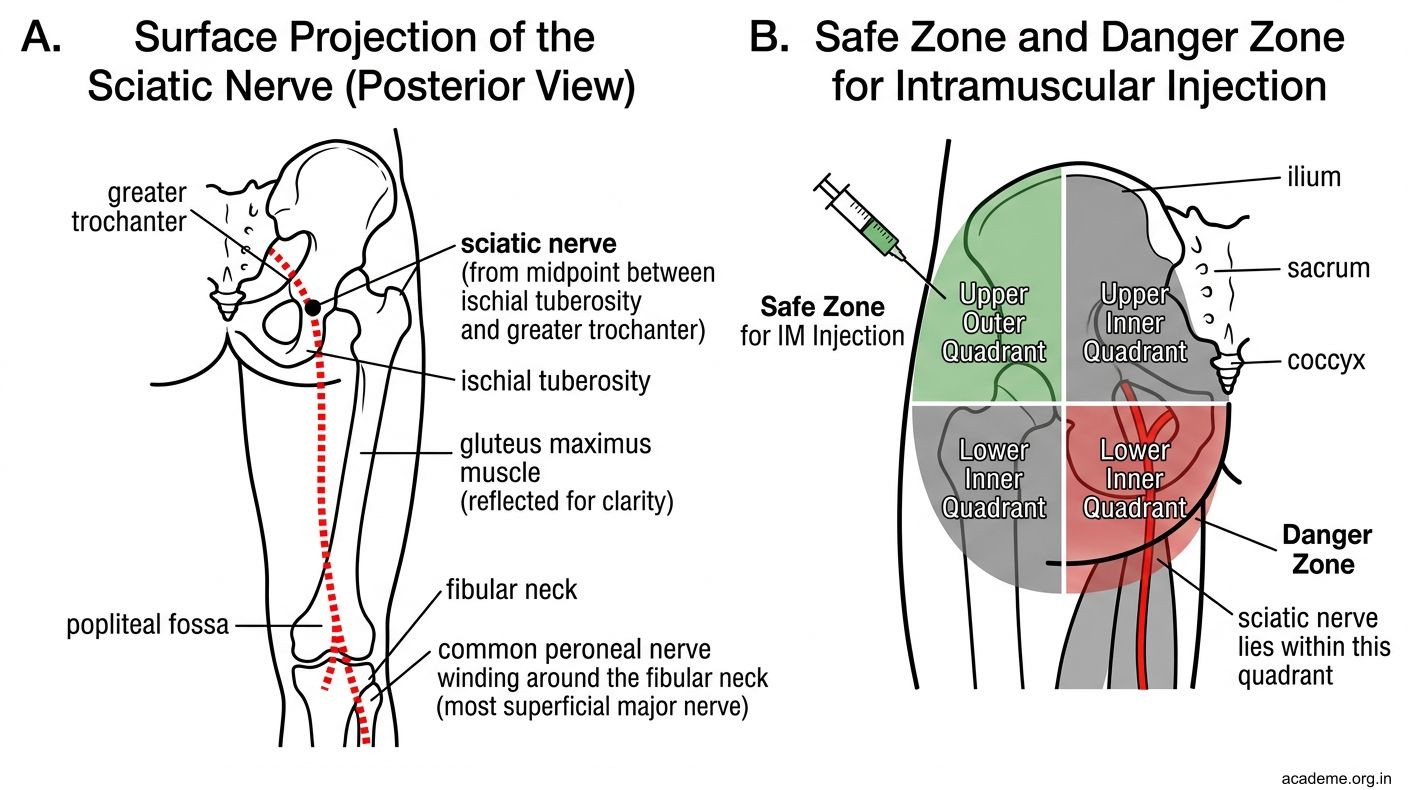
Figure: AN20.9 — Surface Projections
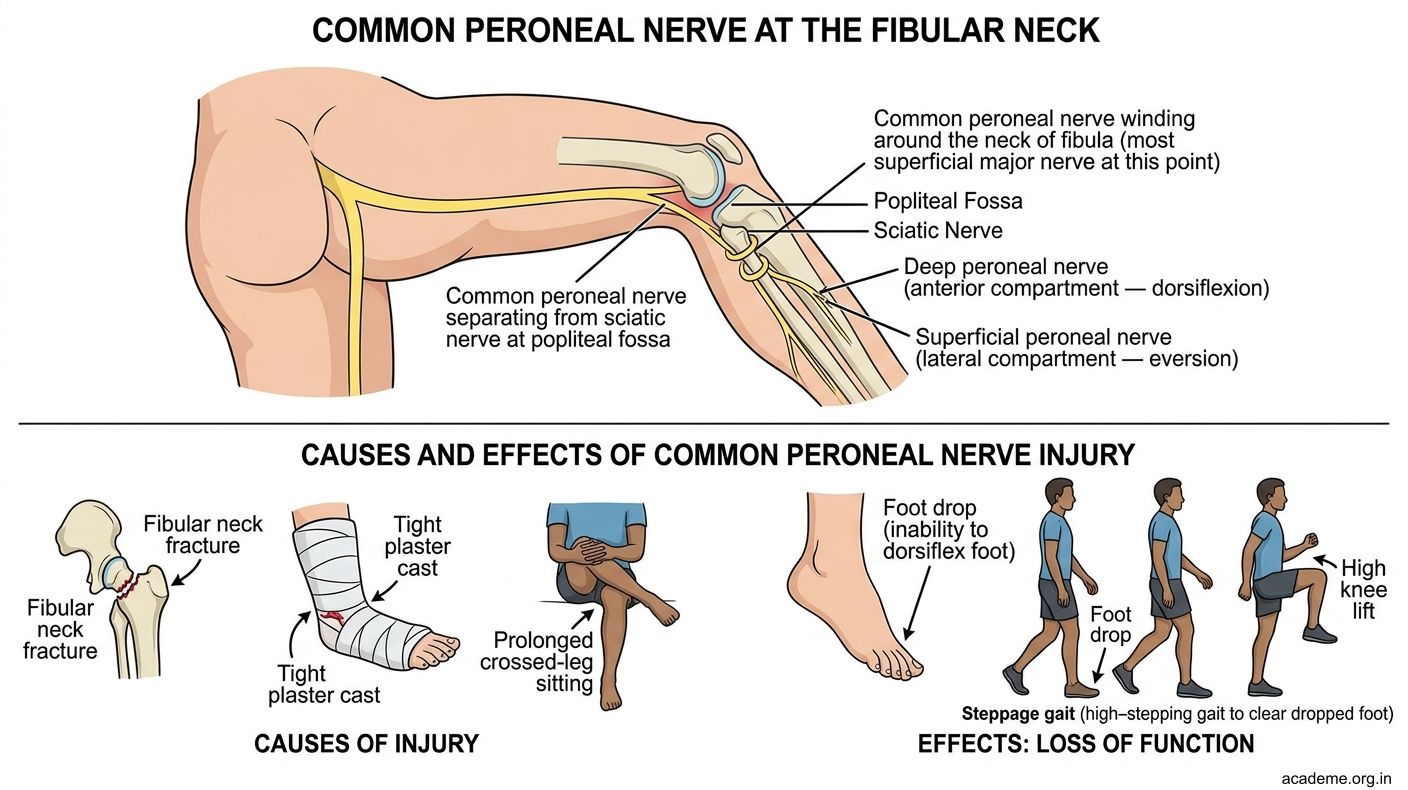
Figure: Common Peroneal Nerve
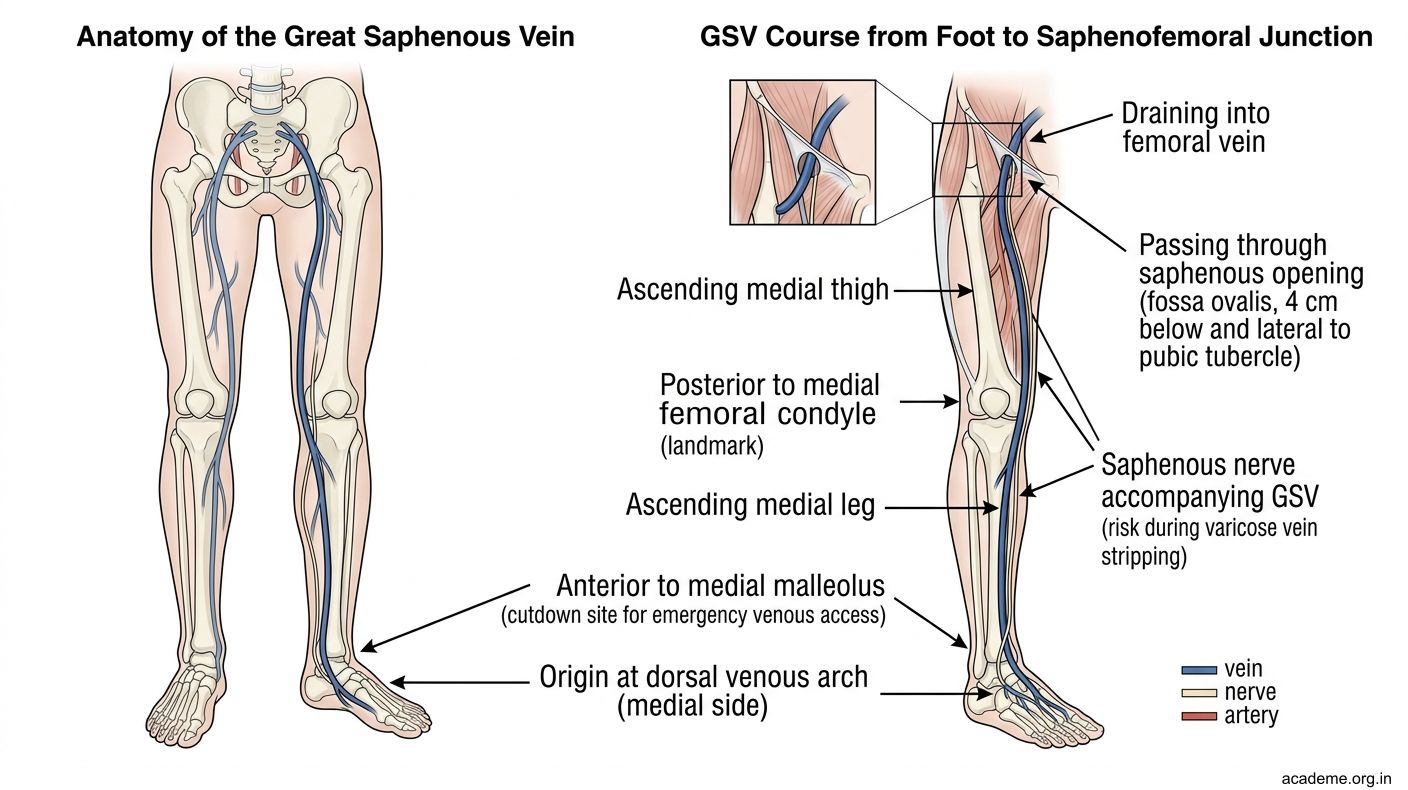
Figure: Great Saphenous Vein (GSV)
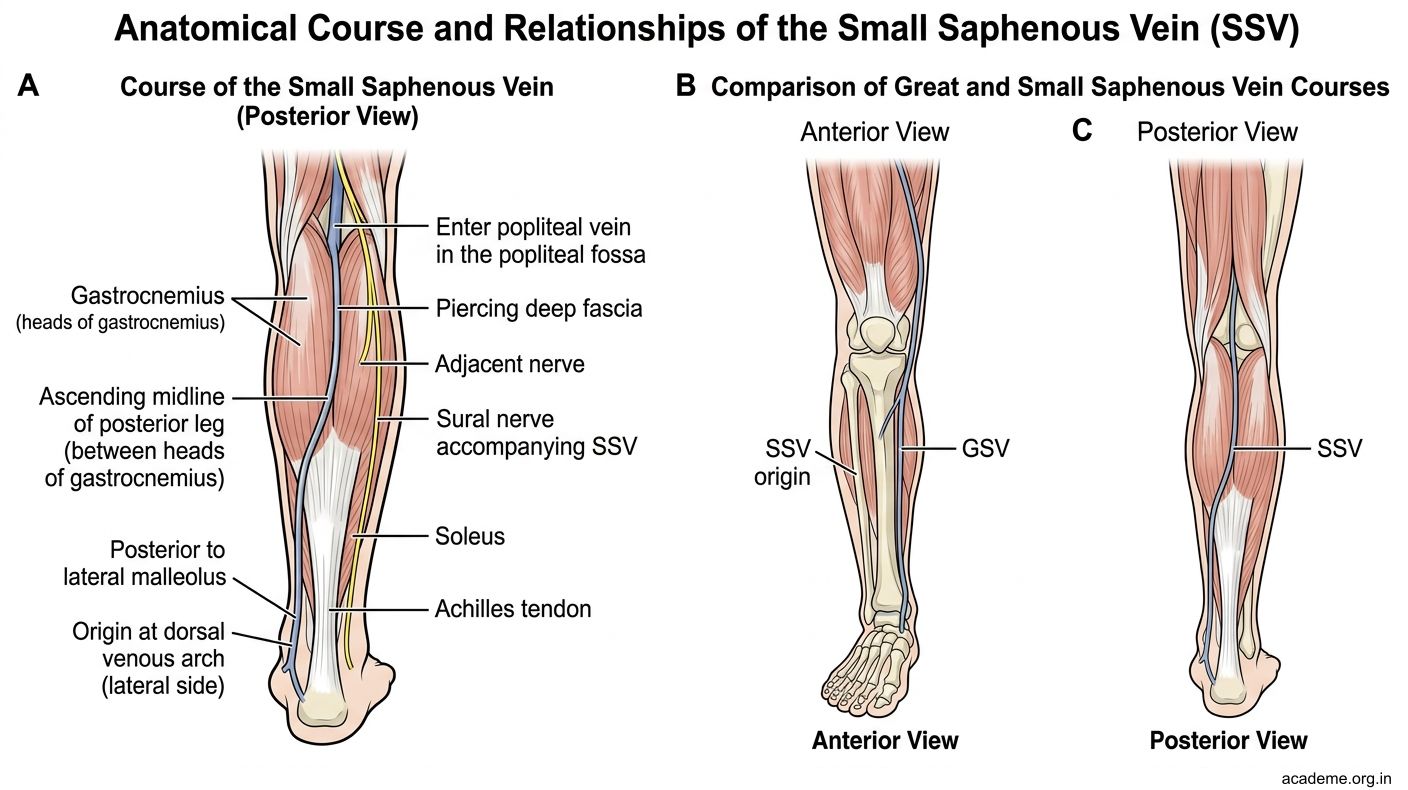
Figure: Small Saphenous Vein (SSV)
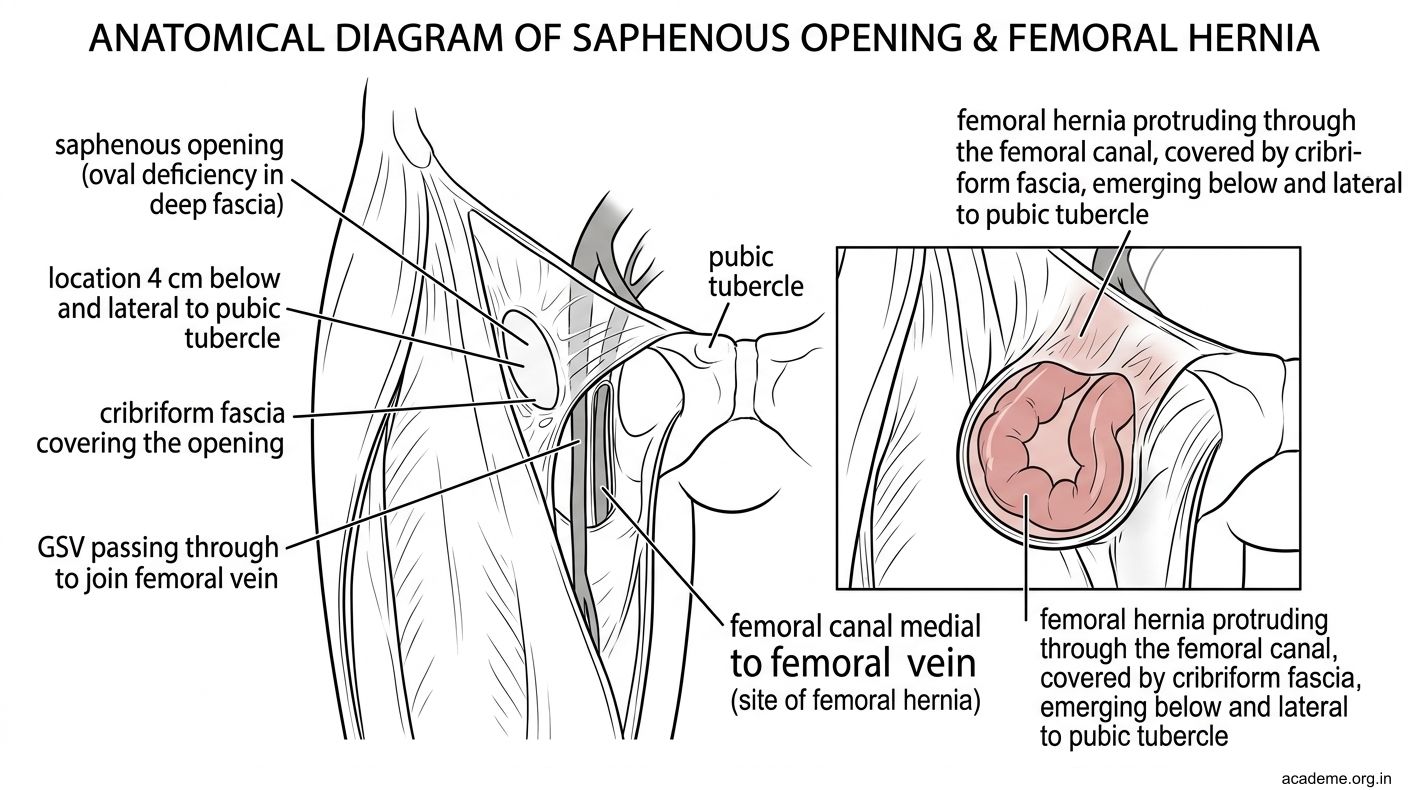
Figure: Saphenous Opening (Fossa Ovalis)
SELF-CHECK — 2
A 55-year-old man presents with foot drop after prolonged sitting with his right leg crossed over the left knee. Which structure is compressed at the fibula neck?
A. Tibial nerve
B. Sciatic nerve at the sciatic notch
C. Common peroneal nerve
D. Femoral nerve
Reveal Answer
Answer: C. Common peroneal nerve
Carcinoma of the scrotum most commonly metastasizes first to which lymph node group?
A. Para-aortic (lumbar) lymph nodes
B. Internal iliac lymph nodes
C. Superficial inguinal lymph nodes
D. Deep inguinal lymph nodes
Reveal Answer
Answer: C. Superficial inguinal lymph nodes
The dorsalis pedis artery is the continuation of which vessel?
A. Posterior tibial artery
B. Peroneal artery
C. Anterior tibial artery
D. Popliteal artery
Reveal Answer
Answer: C. Anterior tibial artery