Page 4 of 8
AN20.1-10 | General Features, Joints, radiographs & surface marking (Lower Limb) — SDL Guide (Part 4)
Development of the Lower Limb
AN20.10 — Lower Limb Development

Figure: Medial clear space

Figure: Tibiofibular clear space

Figure: Development of the Lower Limb
Timeline:
- Week 4 (day 28): Lower limb buds appear as lateral plate mesoderm outgrowths at L2-S2 spinal levels
- Week 5: Digital rays visible; limb rotates medially (opposite to upper limb which rotates laterally)
- Week 6: Interdigital notches form
- Week 8: All major segments defined; basic external appearance of limb
- Week 12: Ossification centres appear in long bones
Medial rotation (unique to lower limb):
The lower limb rotates ~90° medially during development. This is why:
- The great toe (homolog of thumb) is on the medial side
- The extensor muscles are on the front (anterior) of the leg (homologous to arm extensors which are posterior)
- Dermatomes spiral: L1-L4 are anterior; L5-S2 are posterior; S1 wraps under to the sole
Embryological basis of common anomalies:
- Club foot (talipes equinovarus): Arrested rotation + muscle imbalance during week 8-12
- Congenital dislocation of hip (DDH): Shallow acetabulum + ligamentous laxity, exacerbated by breech positioning; 6x more common in females
- Polydactyly: Extra digits from overdevelopment of digital rays
- Syndactyly: Failure of inter-digital apoptosis
- Limb reduction defects: Thalidomide (anti-nausea drug used in India in the 1960s) inhibited limb bud vasculature at weeks 4-6 → phocomelia (seal limbs)
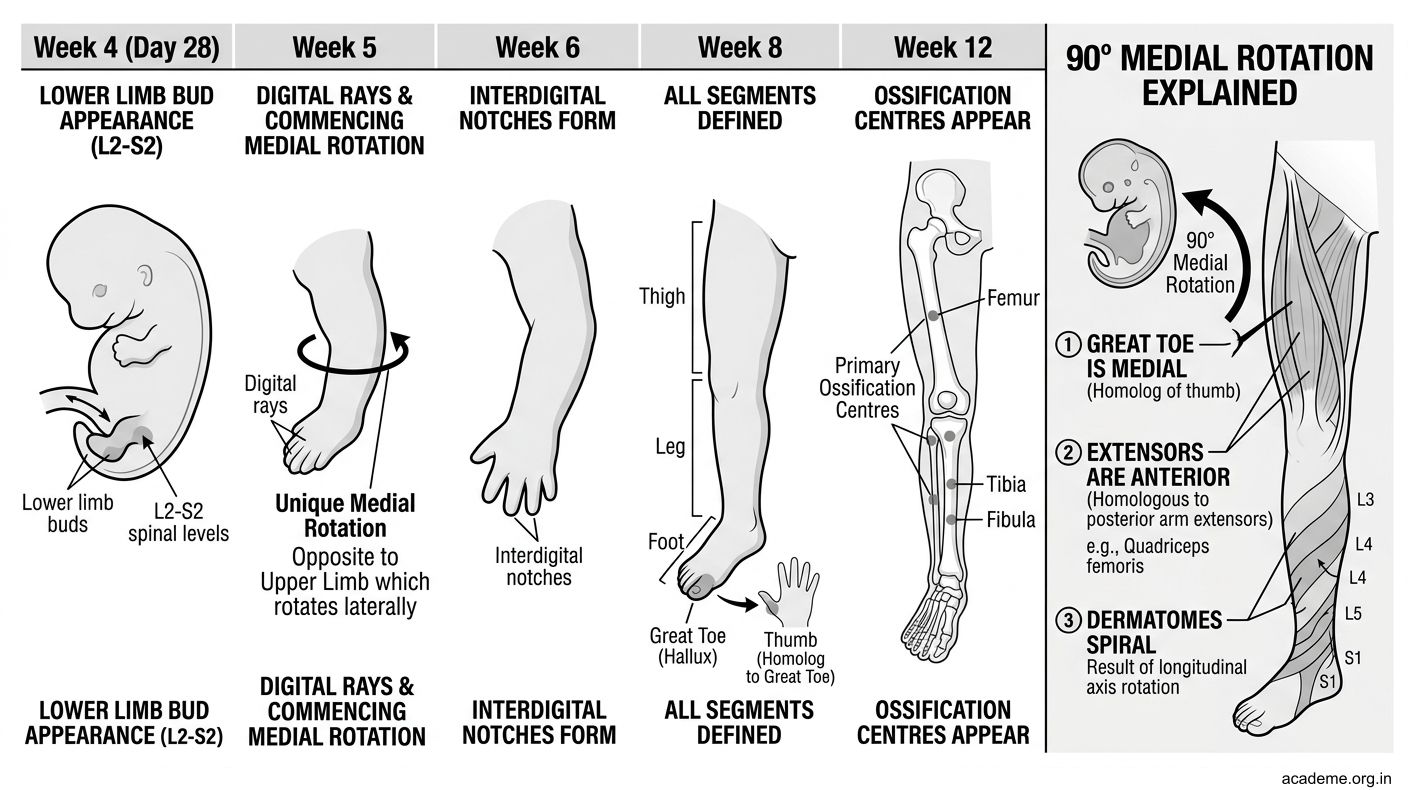
Figure: Development of the Lower Limb

Figure: Embryological basis of common anomalies
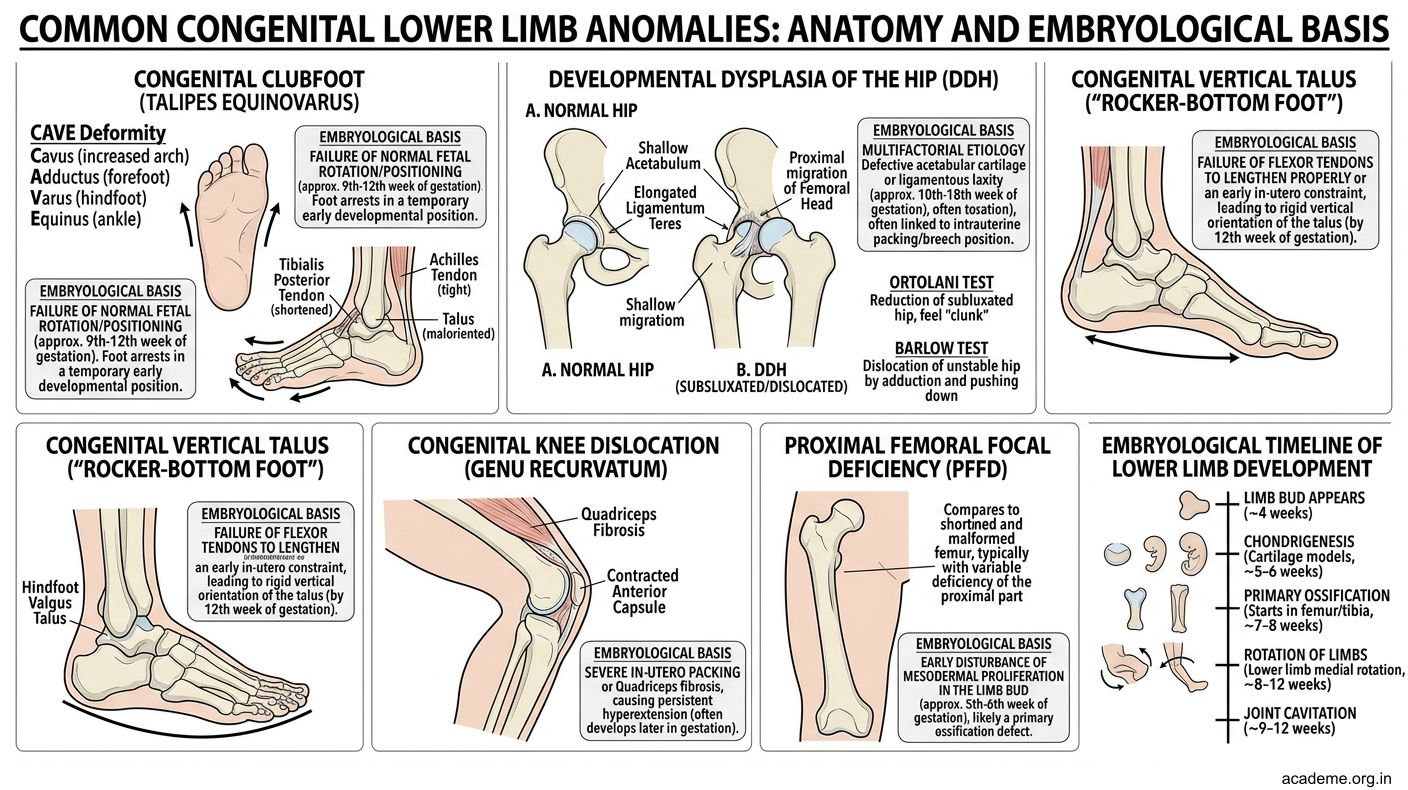
Figure: Embryological basis of common anomalies
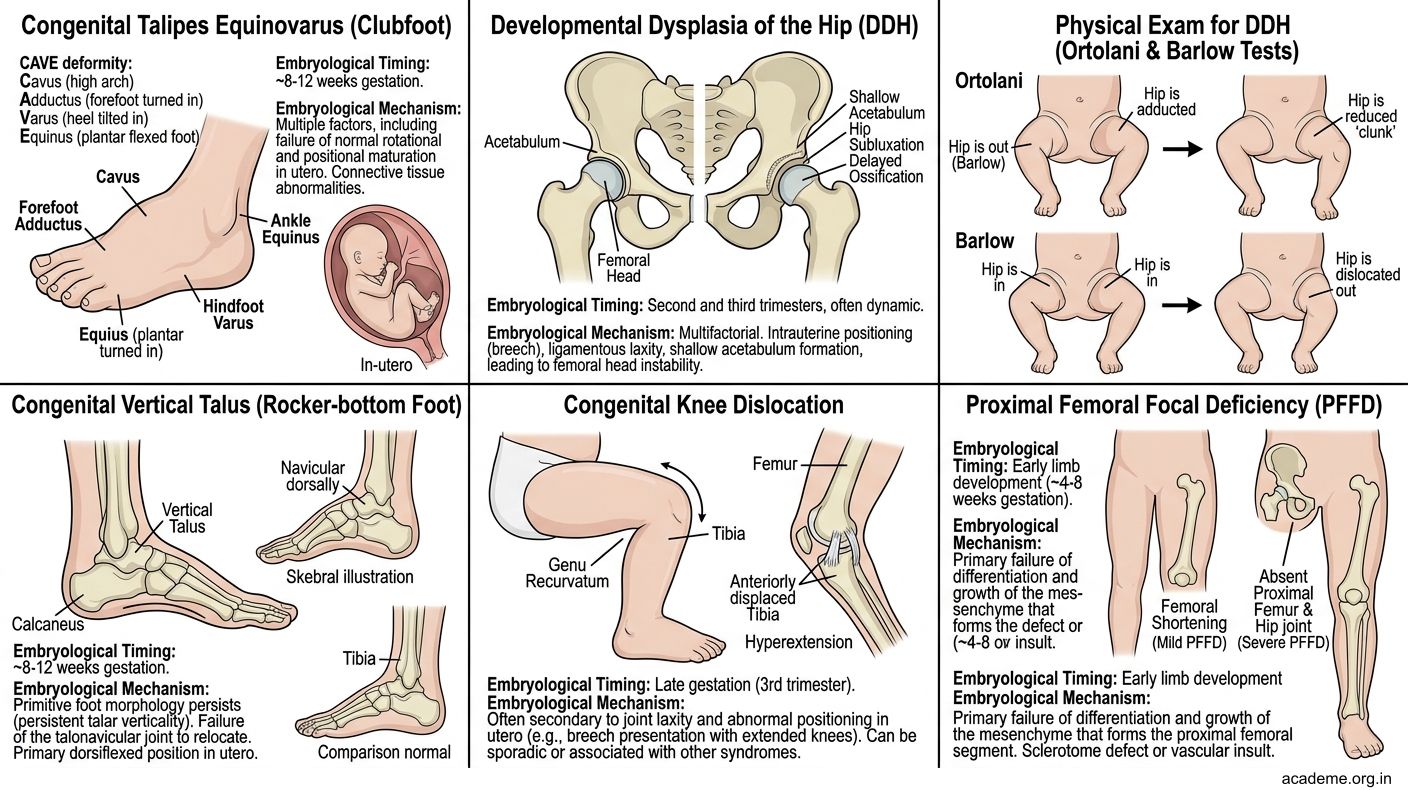
Figure: Embryological basis of common anomalies
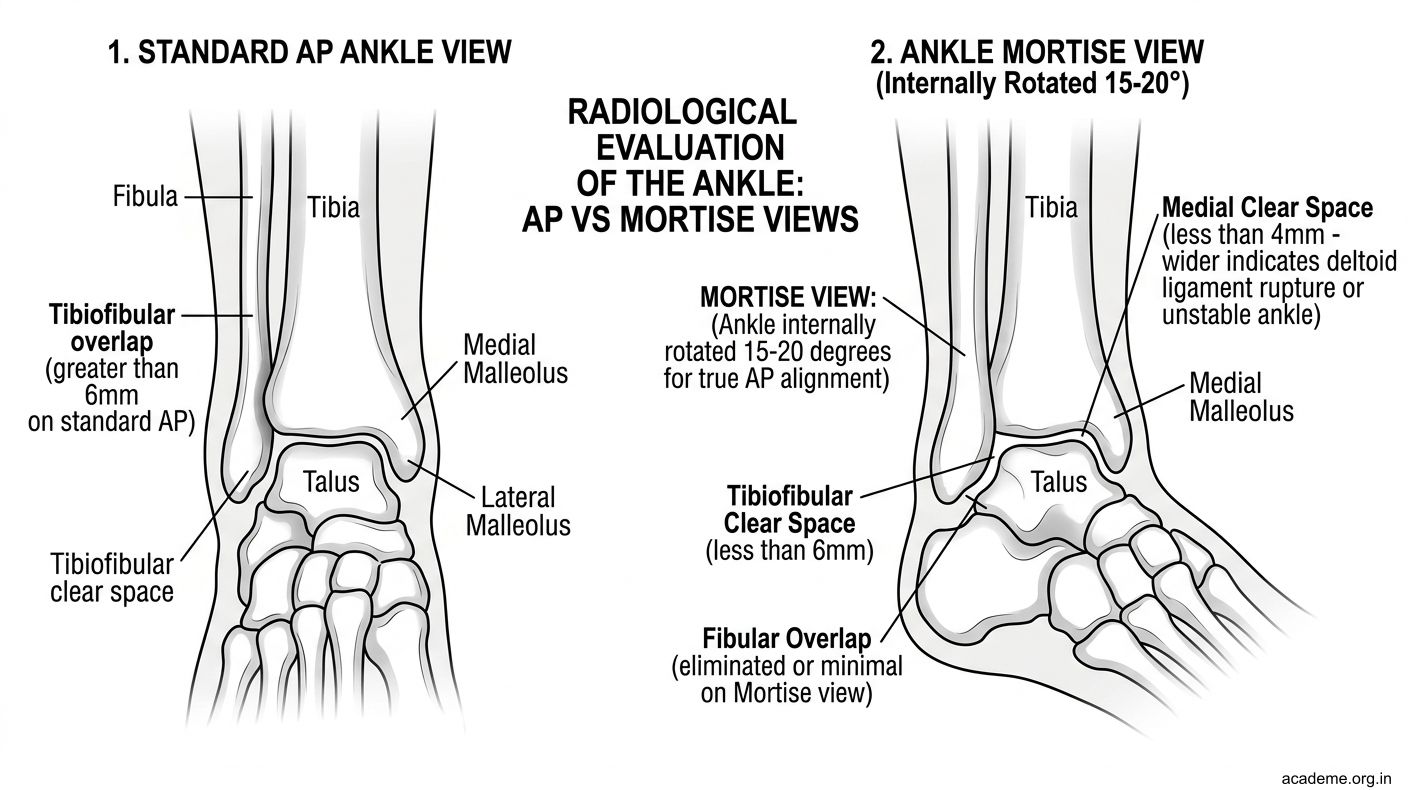
Figure: Tibiofibular clear space
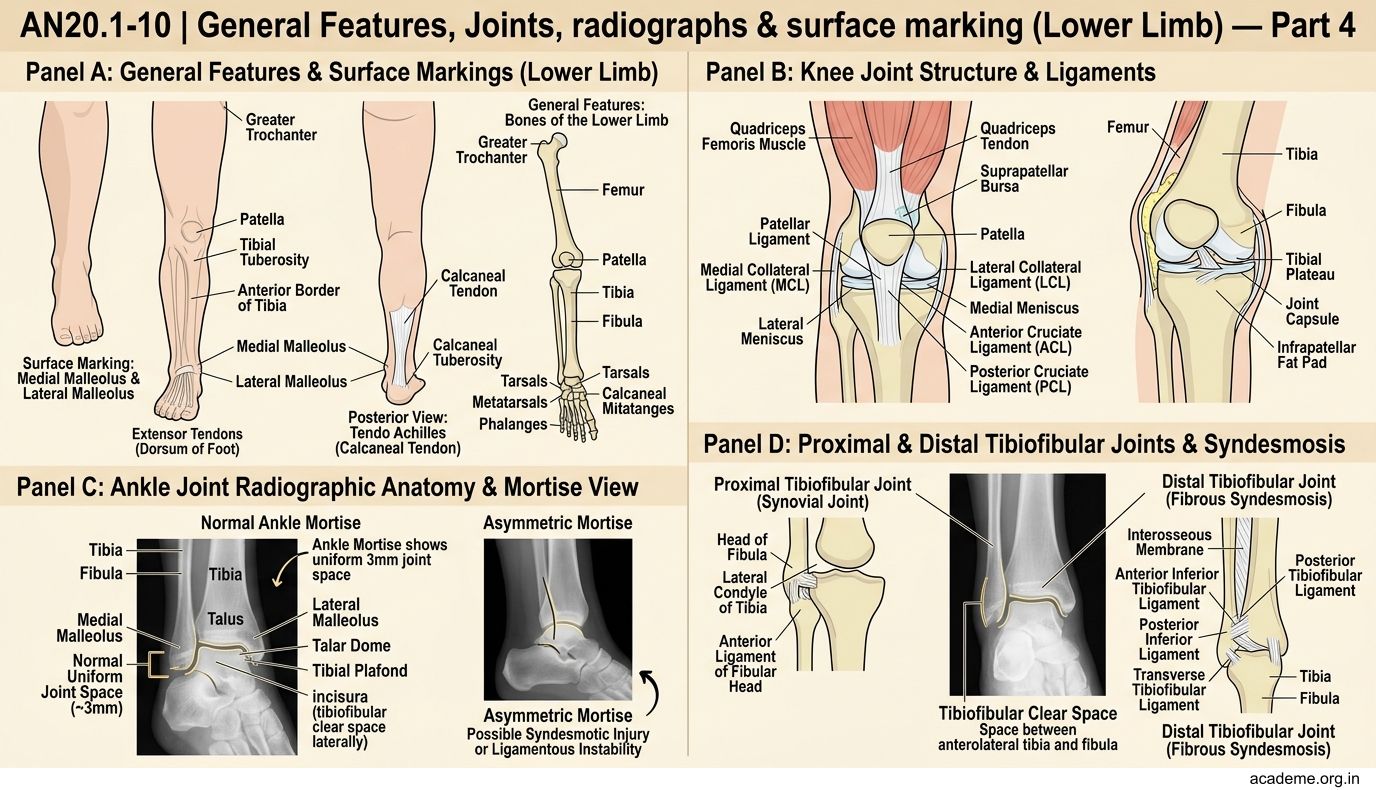
Figure: Medial clear space
CLINICAL PEARL
Standard ankle X-rays include AP, Mortise (15-20° internal rotation), and Lateral views.
The Mortise View (most important):
- Internal rotation of ~15° brings the ankle into true AP alignment (because the lateral malleolus is posterior to the medial)
- A normal ankle mortise shows a uniform 3mm joint space between the talar dome and the tibial plafond (above), medial malleolus (medially), and the 'incisura' (tibiofibular clear space laterally)
- Asymmetric mortise → syndesmotic injury or ligamentous instability
Tibiofibular clear space: On the mortise view, the space between the anterolateral tibia and the fibula should be <6 mm. Wider → syndesmotic (high ankle) sprain.
Medial clear space: Space between the medial border of the talus and the medial malleolus should be <4 mm. Wider = deltoid ligament rupture or unstable ankle.
Bohler's angle on lateral X-ray of calcaneus: Draw a line from posterior facet to tuberosity, and another from anterior process to posterior facet. Normal angle = 20-40°. Reduced → calcaneal fracture (typical in falls from height — road construction workers, suicides).
SELF-CHECK — 3
A right-handed orthopaedic surgeon performing intramedullary nailing of the femur identifies the iliac crest as a landmark. The highest point of the iliac crest corresponds to which vertebral level?
A. L2
B. L3
C. L4
D. L5
Reveal Answer
Answer: C. L4
The medial rotation of the lower limb during fetal development explains which anatomical arrangement?
A. The great toe is on the lateral side
B. The extensor muscles are anterior to the leg
C. The flexor muscles are anterior to the thigh
D. The peroneal nerve is medial to the fibula
Reveal Answer
Answer: B. The extensor muscles are anterior to the leg