Page 7 of 20
CM8.3 | CM8.3 | Disease-Specific National Health Programmes — SDL Guide
Learning Objectives
- Explain the rationale for disease-specific national programmes and how they differ from general health system delivery
- Identify the epidemiological determinants that shaped the design of NTEP, NVBDCP, NLEP, NACO, NPCDCS, and NHM programmes
- Describe programme-specific interventions, case management protocols, and PHC-level delivery responsibilities
- Recognise key programme monitoring indicators and the information systems used to track them
- Apply integrated knowledge of multiple national programmes to the practical context of PHC-level clinical care
INSTRUCTIONS
India runs over twenty national health programmes simultaneously, each targeting a specific disease or health challenge with standardised protocols, dedicated funding, and defined roles for every level of the health system. You, as a PHC physician, are the critical last-mile delivery point for most of these. This module maps the key programmes, explains the logic behind each, and builds your working knowledge of what you must actually do — deliver DOTS, dispense MDT, notify TB cases on NIKSHAY, conduct immunization sessions, and report programme data — as part of a typical week at any PHC in India.
References
- Park's Textbook of Preventive and Social Medicine, 26th ed., Ch. 6 (National Health Programmes) (textbook)
- MoHFW India: Programme Guidelines — NTEP, NVBDCP, NLEP, NACO, NPCDCS (latest editions) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is Monday morning at a busy rural PHC. The roster for the week lists: a TB DOTS session for three patients on day 3 of intensive phase treatment; an NLEP contact examination for the household of a newly diagnosed leprosy patient; an immunization session (pentavalent, PCV, OPV) for seven infants; a malaria rapid test for two febrile patients from a border district; and the monthly NIKSHAY data upload. The PHC physician is implementing five national health programmes simultaneously — without knowing them deeply, she cannot execute any of them safely.
WHY THIS MATTERS
National health programmes represent decades of investment, scientific evidence, and public health planning. Their protocols are not arbitrary — every decision about DOTS frequency, MDT duration, immunization schedule, and ART eligibility reflects accumulated evidence about what actually reduces disease burden at population scale. For the PHC physician, knowing these programmes deeply serves two practical purposes: first, it enables correct case management (the right drug, the right dose, the right duration for the right patient); second, it enables accurate programme reporting, which is how India tracks whether it is on course to meet its disease-elimination targets. Deviation from programme protocols — however well-intentioned — undermines both patient outcomes and national data.
RECALL
From earlier in this cluster, recall:
- NTEP, NVBDCP, NLEP, NACO — the four major communicable disease control programmes discussed in SDL 1; their names, target diseases, and basic strategies.
- NPCDCS — the NCD umbrella programme from SDL 2; targets cancer, diabetes, CVD, and stroke.
- UIP (Universal Immunization Programme) — the vaccine schedule for children from birth through adolescence.
This SDL deepens your knowledge of each programme's specific case management protocols, monitoring indicators, and PHC-level implementation responsibilities — moving from 'what exists' to 'exactly how you implement it'.
Scale of National Health Programmes: Why Vertical Programmes Exist
The existence of disease-specific vertical programmes — with dedicated staff, budgets, supply chains, and protocols — rather than simply folding all disease management into a general primary care system is a deliberate epidemiological choice. Vertical programmes exist because the evidence from low- and middle-income country experience consistently shows that high-burden diseases with complex case management, long treatment durations, and significant transmission consequences require: (1) standardised protocols that eliminate variation-driven failures (a district TB officer cannot individually design 50 different treatment regimens — NTEP's standardised 6-month regimen eliminates this variation); (2) dedicated supply chains ensuring medicines are consistently available (MDT blister packs for NLEP, DOTS medicines for NTEP); (3) programme-specific training for health workers who must perform specialised tasks (slit-skin smear reading, DOTS supervision, VIA technique); and (4) programme accountability — measurable targets and indicators that create pressure for results.
Provided image
India's national health architecture places the Ministry of Health and Family Welfare (MoHFW) at the apex, with the National Health Mission (NHM) providing the structural and financial framework within which disease-specific programmes operate. The District Health and Family Welfare Society (DHFWS) manages programme implementation at district level, coordinating with PHCs, CHCs, district hospitals, and medical colleges. The PHC sits at the delivery end — it is where programmes meet patients.
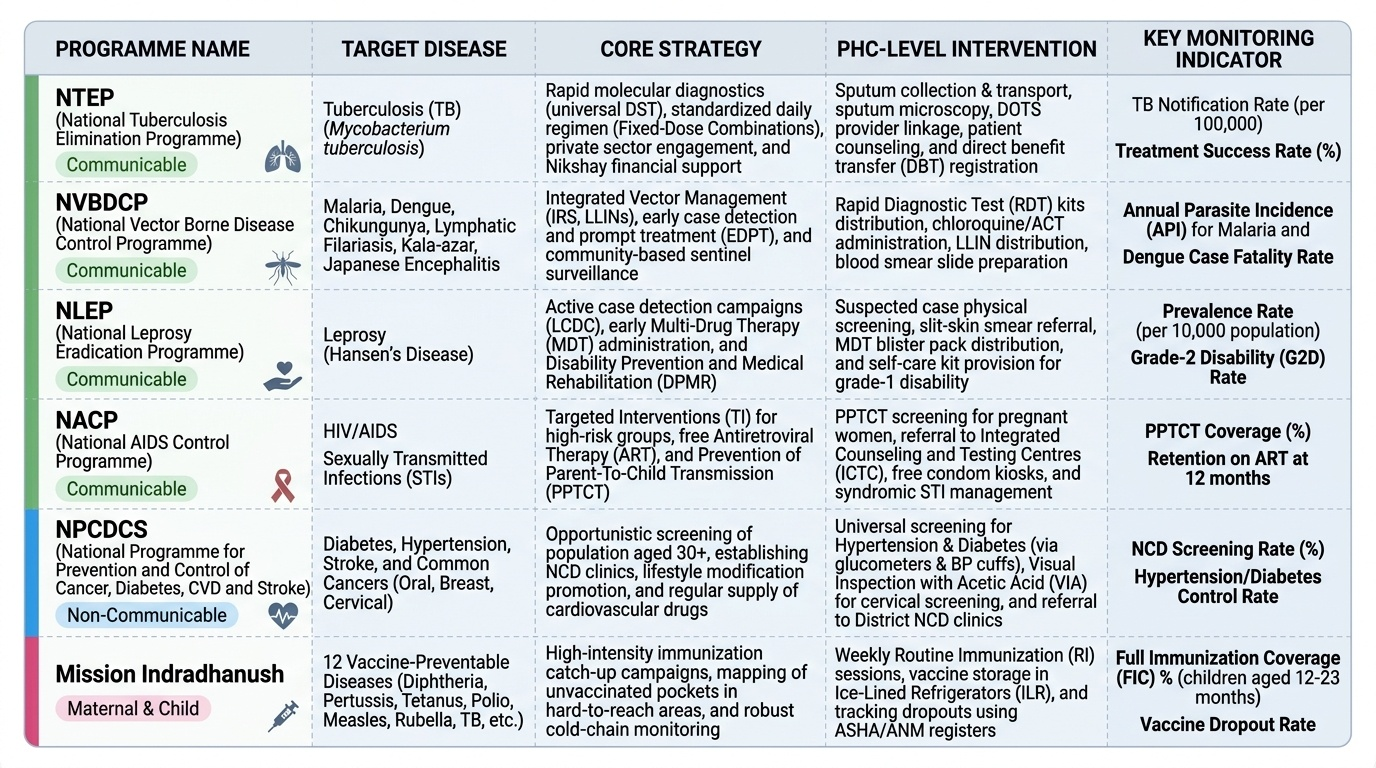
India's major disease-specific national health programmes currently active at PHC level include:
- Communicable diseases: NTEP (tuberculosis), NVBDCP (vector-borne diseases), NLEP (leprosy), NACO (HIV/AIDS), National Programme for Control of Blindness & Visual Impairment (NPCBVI)
- Non-communicable diseases: NPCDCS (cancer, diabetes, CVD, stroke), National Tobacco Control Programme (NTCP), National Oral Health Programme
- Maternal and child health under NHM: Janani Suraksha Yojana (JSY), Janani Shishu Suraksha Karyakram (JSSK), Mission Indradhanush (immunization), Pradhan Mantri Matru Vandana Yojana (PMMVY), Poshan Abhiyan (nutrition)
- Mental health: National Mental Health Programme (NMHP), DMHP at district level
SELF-CHECK
Which administrative body coordinates national health programme implementation at the district level in India?
A. PHC Medical Officer
B. District Health and Family Welfare Society (DHFWS)
C. State Surveillance Unit
D. National Health Mission headquarters
Reveal Answer
Answer: B. District Health and Family Welfare Society (DHFWS)
The District Health and Family Welfare Society (DHFWS) coordinates programme implementation at the district level, managing budget allocation, supply chain, personnel, and reporting for all national health programmes operating within the district. The PHC is the delivery point; the DHFWS is the district coordinator.
Disease-Specific Determinants Driving Programme Design
Each national programme's design reflects the specific epidemiological determinants of its target disease. Understanding this logic transforms rote protocol memorisation into principled understanding — making it far easier to recall, adapt, and communicate to patients and health workers.
NTEP (TB): TB is transmitted by airborne droplet nuclei. The most powerful determinant of ongoing transmission is the infectious period — an untreated smear-positive patient remains infectious for months. NTEP's DOTS strategy directly attacks this determinant: supervised daily treatment reduces the infectious period from months to 2–4 weeks. The monitoring system (NIKSHAY) tracks every patient to ensure no one is lost to follow-up and remains infectious without treatment. Multidrug regimens prevent drug resistance from emerging.
NVBDCP (Vector-borne diseases): Malaria, dengue, and filariasis transmission requires a live arthropod vector — Anopheles mosquitoes for malaria, Aedes aegypti for dengue, Culex quinquefasciatus for filariasis. The programme therefore targets both the vector (IRS, larval source reduction, insecticide-treated bednets/LLINs) and the human host (early treatment to shorten the period when parasites are in the blood, reducing transmission to mosquitoes; annual mass drug administration for filariasis). The endemic geography drives programme intensity — high-burden districts receive more IRS rounds and more active surveillance.
NLEP (Leprosy): Leprosy transmission requires prolonged close contact with an infectious multibacillary case. The programme targets this by: (a) early case detection (to reduce the infectious period); (b) contact examination of all household members; (c) MDT (which renders patients non-infectious within 72 hours of the first rifampicin dose). The low infectivity of paucibacillary cases means PB MDT is shorter (6 months).
NACO (HIV): HIV is transmitted through specific routes — sexual contact, parenteral (needles, transfusions), and vertical (mother to child). Each route has a targeted intervention: condom promotion + key population targeted services for sexual transmission; needle exchange + opioid substitution therapy (OST) for injecting drug users; PPTCT (Prevention of Parent-to-Child Transmission) for vertical transmission. The Test and Treat policy (ART for ALL PLHIV regardless of CD4 count) both treats the individual and reduces transmission (undetectable = untransmittable, U=U).
NPCDCS (NCDs): NCDs share modifiable risk factors (tobacco, diet, inactivity) and are detected early through screening — the programme therefore mandates systematic opportunistic screening at PHCs and sub-centres for adults ≥30 years.
Programme-Specific Interventions, Case Management, and PHC-Level Delivery
The following describes the core case management protocols and PHC physician responsibilities for each major programme:
NTEP — National Tuberculosis Elimination Programme:
- Register all presumptive TB patients on NIKSHAY
- Order CBNAAT/TrueNAT for all presumptive cases; sputum smear as backup
- All new TB cases: daily HREZ (Isoniazid + Rifampicin + Ethambutol + Pyrazinamide) × 2 months intensive phase, then daily HR × 4 months continuation phase (total 6 months)
- Provide Nikshay Poshan Yojana (Rs 500/month nutritional support) to all notified patients
- Refer rifampicin-resistant cases (on CBNAAT) to DR-TB centre immediately
- DOTS: supervised treatment — ideally daily observation at PHC or home by ASHA
NVBDCP — Malaria:
- Test all fever cases with RDT; treat P. falciparum with ACT (artemether-lumefantrine, weight-based); treat P. vivax with chloroquine (3 days) + primaquine (14-day radical cure; check G6PD status before primaquine)
- Report all malaria cases to district; maintain case register
- IRS (indoor residual spraying) in endemic areas; distribute LLINs (long-lasting insecticide-treated nets)
- Annual Blood Examination Rate (ABER) ≥10% target in endemic districts
NVBDCP — Dengue:
- No antiviral; supportive treatment; refer severe dengue (dengue with warning signs)
- Vector surveillance: weekly Aedes larval survey in endemic areas; fogging (space spraying) during outbreak only
- Case notification to District Vector Control Officer
NVBDCP — Filariasis (Lymphatic Filariasis):
- Annual MDA (mass drug administration): single-dose DEC 6 mg/kg + albendazole 400 mg to all eligible persons in endemic districts (National Filaria Day)
- Morbidity management and disability prevention (MMDP) for chronic lymphoedema patients
NLEP — National Leprosy Eradication Programme:
- Diagnose on three cardinal signs: hypopigmented/erythematous skin lesion with loss of sensation; thickened peripheral nerve; skin smear positive for acid-fast bacilli
- Classify: PB (1–5 lesions, negative smear) vs MB (>5 lesions or positive smear)
- Dispense MDT blister packs: PB — 6 monthly packs (rifampicin 600 mg monthly supervised + dapsone 100 mg daily); MB — 12 monthly packs (rifampicin 600 mg monthly supervised + clofazimine 300 mg monthly supervised + clofazimine 50 mg daily + dapsone 100 mg daily)
- Examine ALL household contacts; refer nerve function impairment for physiotherapy
NACO — HIV/AIDS:
- Refer to Integrated Counselling and Testing Centre (ICTC) for HIV counselling and testing
- Initiate ART for ALL PLHIV regardless of CD4 count (Test and Treat policy since 2017)
- PPTCT: test all pregnant women at ANC; give ART to HIV-positive mothers from 14 weeks of pregnancy
- Refer advanced disease (WHO stage 3/4, or CD4 <200) to ART centre
UIP — Immunization:
- Conduct fixed-day immunization sessions at sub-centres on scheduled dates
- Cold chain management: maintain 2–8°C for all vaccines (OPV at -15 to -25°C)
- Record all vaccinations in mother-child tracking system; follow up defaulters through ASHA
- Mission Indradhanush/IMI: intensified campaigns to reach unimmunized and partially immunized children
SELF-CHECK
Under current NTEP guidelines, what is the treatment regimen for a newly diagnosed drug-sensitive tuberculosis case?
A. 2 months HREZ + 4 months HR (daily, 6 months total)
B. 2 months HRZ + 4 months HR (thrice weekly, 6 months total)
C. 6 months HREZ (daily continuous)
D. 2 months HR + 4 months HE (daily, 6 months total)
Reveal Answer
Answer: A. 2 months HREZ + 4 months HR (daily, 6 months total)
Under current NTEP guidelines, new drug-sensitive TB cases receive daily 2HREZ + 4HR — 2 months of Isoniazid (H) + Rifampicin (R) + Ethambutol (E) + Pyrazinamide (Z) in the intensive phase, followed by 4 months of Isoniazid + Rifampicin in the continuation phase. The old thrice-weekly regimen has been replaced by daily dosing under NTEP (important difference from RNTCP era).