Page 8 of 20
CM8.3 | CM8.3 | Disease-Specific National Health Programmes — SDL Guide (Part 2)
Programme Monitoring, Indicators, and Information Systems
Every national health programme has a defined set of monitoring indicators that measure programme performance at PHC, district, state, and national levels. Familiarity with these indicators helps the PHC physician understand what 'good performance' looks like and how their own data feed into national dashboards.
NTEP key indicators:
- Treatment success rate (TSR): percentage of new bacteriologically confirmed TB cases that are successfully treated (cured + completed). Target: ≥90%
- Loss to follow-up rate: percentage of patients who interrupt treatment for ≥2 consecutive months
- NIKSHAY: real-time web-based case registration, treatment monitoring, and outcome recording platform — PHC uploads case data, treatment dates, and outcomes
NVBDCP — Malaria indicators:
- ABER (Annual Blood Examination Rate): percentage of the population in an endemic area examined by blood smear or RDT per year; target ≥10% in high-endemic districts
- API (Annual Parasite Incidence): number of confirmed malaria cases per 1000 population per year; used to stratify districts (API <1 = low, API ≥1 = high)
- Slide Positivity Rate (SPR): percentage of tested blood slides/RDTs positive
NLEP key indicators:
- New Case Detection Rate (NCDR): new leprosy cases per 100,000 population per year; target is elimination (<1 per 10,000)
- Grade 2 Disability Rate (G2DR): percentage of new cases with grade 2 disability (visible deformity) at diagnosis — reflects late detection
- MDT completion rate: percentage completing prescribed MDT course
NACO key indicators:
- PLHIV on ART (Viral Suppression Rate): percentage of PLHIV on ART with undetectable viral load (<1000 copies/mL)
- PPTCT coverage: percentage of HIV-positive pregnant women receiving ART for PPTCT
- 90-90-90 targets (UNAIDS): 90% of PLHIV know their status; 90% of those diagnosed on ART; 90% of those on ART virally suppressed
Information systems:
- NIKSHAY: NTEP's dedicated TB case management system (web + mobile)
- HMIS (Health Management Information System): MoHFW's integrated platform aggregating all programme reports from PHC upward
- NVBDCP MIS: malaria/vector-borne disease reporting portal
- National AIDS Control Organisation (NACO) MIS: ICTC and ART centre reporting
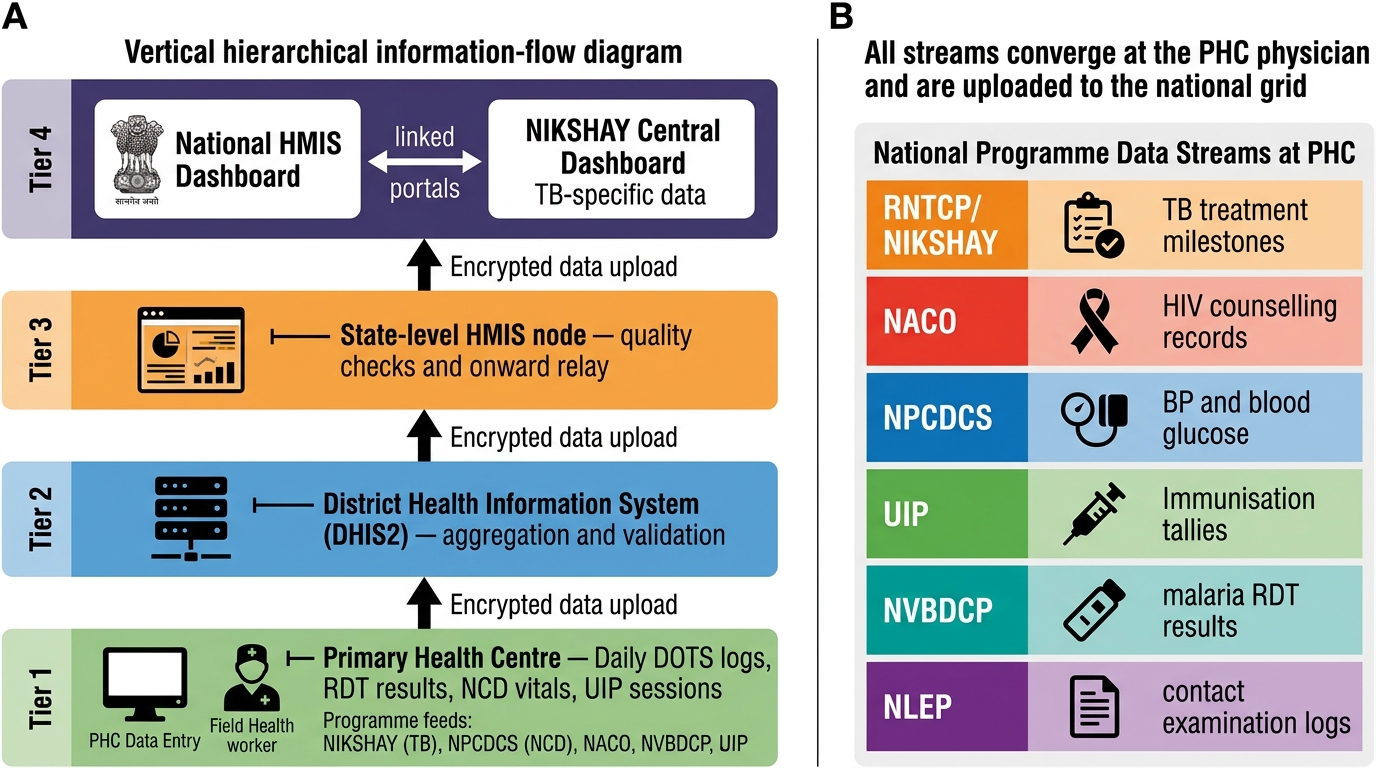
India's National Health Programme Information Flow: PHC to National HMIS and NIKSHAY
CLINICAL PEARL
A patient belongs to multiple programmes simultaneously. A 35-year-old man on DOTS for pulmonary TB who also has diabetes (NPCDCS) and whose wife is HIV-positive (NACO — PPTCT counselling needed) is one patient managed under three national programmes at once. The PHC physician must navigate all three simultaneously: TB treatment impacts glycaemic control (rifampicin induces cytochrome P450 and reduces plasma levels of oral hypoglycaemics); HIV status of a TB patient determines treatment urgency (HIV-TB co-infection requires ART initiation within 8 weeks of anti-TB treatment). Programme silos exist administratively — they cannot exist in the examining room.
Applying Programme Knowledge at the PHC
Operationalising multiple national health programmes simultaneously at a PHC requires systematic organisation of daily, weekly, and monthly responsibilities.
Daily responsibilities: DOTS supervision for TB patients on treatment; management of walk-in malaria suspects (RDT and treatment per NVBDCP protocol); management of NCD patients on NPCDCS follow-up (BP, blood glucose recording).
Weekly responsibilities: Fixed-day sub-centre immunization sessions (UIP); NLEP contact examination follow-ups; data upload to NIKSHAY for newly diagnosed or treatment-milestone TB patients.
Monthly responsibilities: NLEP MDT monthly supervised dose for MB and PB patients; monthly immunization session at PHC level; HMIS monthly report submission (covering all programme indicators); NVBDCP malaria weekly case reporting consolidated to monthly district report; NPCDCS screening data consolidation.
Integration across programmes — the PHC physician must:
1. Maintain disease-specific registers: TB register (NIKSHAY), leprosy register, malaria register, NCD register (NPCDCS), immunization register (UIP)
2. Know which ASHA worker is responsible for each patient's adherence monitoring under each programme
3. Identify patients eligible for multiple concurrent programmes (TB+HIV co-management, TB+diabetes protocol, leprosy with ENL requiring corticosteroids alongside MDT)
4. Submit accurate and timely programme reports — data integrity at PHC level determines whether national elimination targets appear achievable or are artificially inflated
A practical operational tool: the PHC MO should maintain a weekly programme calendar listing: DOTS session days and patients, immunization session dates and target infants, NLEP contact examination schedule, NVBDCP malaria active case search (if in endemic area), NPCDCS screening session dates. This transforms abstract programme knowledge into operational delivery — the only form that reduces disease burden.
SELF-CHECK
A PHC medical officer discovers a 45-year-old HIV-positive man has just been diagnosed with smear-positive pulmonary tuberculosis. Under current NACO and NTEP co-management guidelines, when should ART be initiated?
A. After completing the full 6-month TB treatment course
B. Simultaneously with anti-TB treatment from day 1
C. Within 8 weeks of starting anti-TB treatment
D. Only when CD4 count falls below 200 cells/µL
Reveal Answer
Answer: C. Within 8 weeks of starting anti-TB treatment
Current HIV-TB co-management guidelines recommend initiating ART within 8 weeks of starting anti-TB treatment in all HIV-positive TB patients, regardless of CD4 count. For patients with CD4 <50 cells/µL (very advanced HIV), ART should be initiated within 2 weeks of anti-TB treatment. This is a critical integration point between NTEP and NACO protocols.