Page 2 of 25
CM1.1-2 | CM1.1-2 | Public Health and Holistic Health — SDL Guide (Part 2)
Defining Health — WHO Definition and Its Critique
Health is defined by the World Health Organization in its 1948 Constitution Preamble as 'a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity.' This was a revolutionary and deliberately positive definition at its time: it rejected the purely negative conceptualisation of health as 'absence of disease' and insisted on well-being as a positive, multidimensional state. The inclusion of mental and social well-being alongside physical was a major advance — it embedded Community Medicine's holistic perspective into international health policy from the outset.
However, the WHO definition has attracted well-founded criticism over subsequent decades. First, the word 'complete' sets an unrealistically high standard — very few people at any moment would meet a standard of complete physical, mental, and social well-being; the definition effectively classifies most of the world's population as unhealthy at most times. Second, the definition is static — it describes health as a state rather than a dynamic adaptive process. Third, it is difficult to operationalise for measurement or research: what exactly constitutes 'complete well-being' across cultures? These critiques led to subsequent reformulations: Huber et al. (2011) proposed redefining health as 'the ability to adapt and self-manage in the face of social, physical, and emotional challenges,' emphasising resilience and function over a static end-state.
For the NMC MBBS curriculum, the WHO definition remains the standard reference. The key point is to know it precisely and understand both its positive contribution and its limitations.
Holistic and Multidimensional Health — Physical, Mental, Social, Spiritual
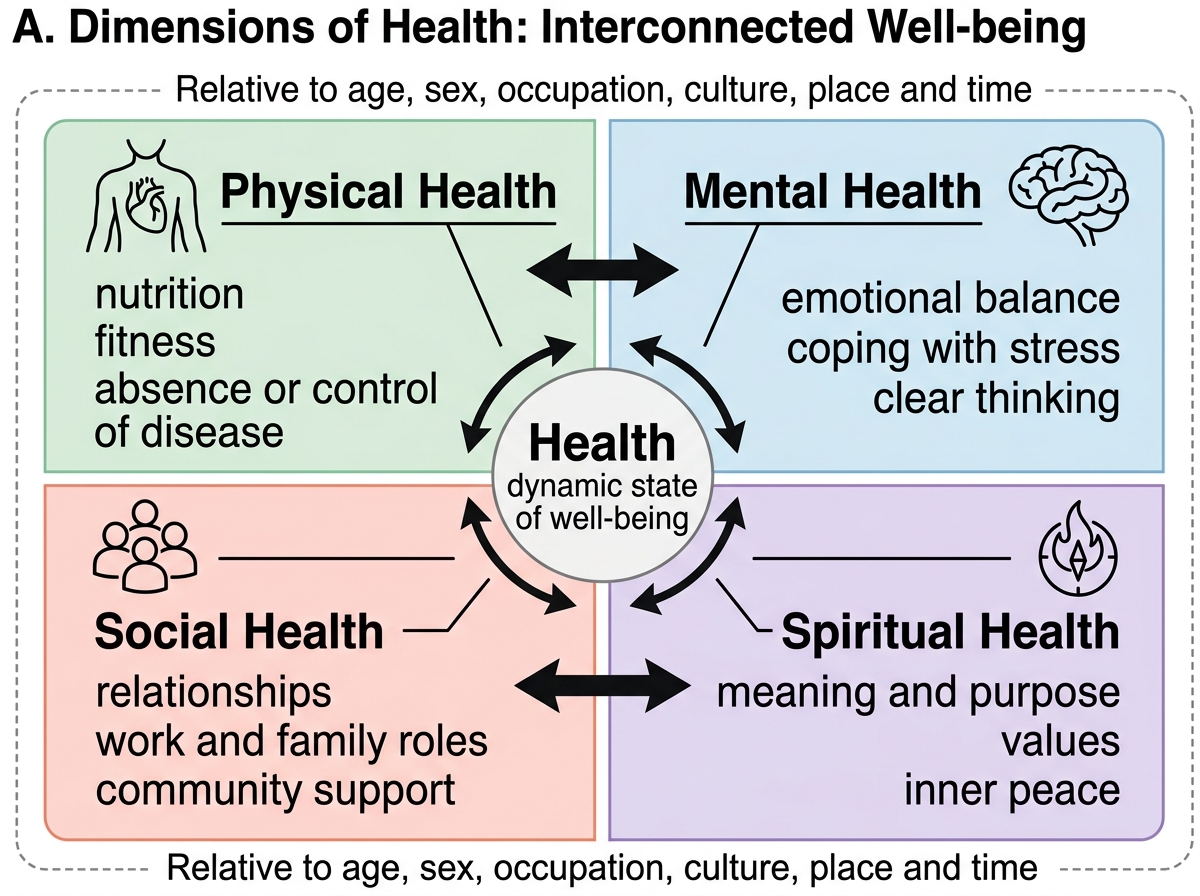
The holistic model of health views the human being as an integrated whole — not merely a biological organism but a psychological, social, and spiritual entity. While the 1948 WHO definition named three dimensions, the concept has since been expanded, particularly in the Indian and global wellness literature, to include a spiritual dimension.
The four recognised dimensions are: (1) Physical health — the body's capacity for normal physiological function, absence of disease or disability, adequate nutrition and fitness; (2) Mental health — emotional stability, psychological resilience, cognitive function, and the capacity to cope with life's stressors; (3) Social health — the capacity to interact meaningfully with others, fulfil social roles, and participate in community life; and (4) Spiritual health — a sense of purpose, meaning, inner peace, and connection to values or a higher purpose, which Halbert Dunn (who coined the term 'high-level wellness' in 1959) identified as integral to full human flourishing. The spiritual dimension does not require religious adherence; it refers to the subjective experience of meaning and coherence in one's life.
Dimensions and Relativeness of Health
Relativeness of health is an equally important concept: health is not an absolute, universal standard but is relative to the individual's age, sex, occupation, and cultural context, as well as the geographic and temporal setting. A blood pressure considered hypertensive in a 25-year-old may be physiologically appropriate in an elderly person with arterial stiffening; a dietary pattern considered unhealthy in urban Mumbai may be the only available option in a remote tribal district. Health standards evolve over time: smoking was once considered medically neutral; infectious diseases once uniformly fatal are now treatable. Recognising relativeness prevents the ethnocentrism of imposing a single 'healthy norm' across diverse populations.
SELF-CHECK
The WHO 1948 definition of health has been criticised primarily because:
A. It focuses only on physical health and ignores mental and social dimensions
B. It sets an unrealistically high standard of 'complete' well-being, making it non-operational
C. It was developed without input from developing countries
D. It defines health negatively as the absence of disease
Reveal Answer
Answer: B. It sets an unrealistically high standard of 'complete' well-being, making it non-operational
The main critique is that 'complete physical, mental and social well-being' sets an impossibly high bar — most people would fail to meet it at most times. The definition is actually positive (not merely 'absence of disease'), and mental/social dimensions ARE included. The development process critique is historically accurate but not the primary substantive criticism.
Applying Public Health Principles — From Concept to Practice
Understanding the definitions and determinants of health would be academic exercise without translation into action. Public health converts conceptual knowledge into organised programmes that act on the determinants of health at scale. In India, this happens through a layered system: national health programmes target major disease burdens (e.g., the National Tuberculosis Elimination Programme, the National Vector Borne Disease Control Programme, the Reproductive and Child Health programme); state governments adapt and implement these; and district health systems deliver services through the Health and Wellness Centres, Primary Health Centres, and Community Health Centres of the Ayushman Bharat Health and Wellness Centre (AB-HWC) network.
Health promotion is the public health strategy that enables individuals and communities to increase control over the determinants of their health. It is broader than health education (giving information) and includes policy changes, supportive environments, community action, and personal skill development — the five action areas of the Ottawa Charter (1986). Information, Education and Communication (IEC) and Behaviour Change Communication (BCC) are specific tools within this broader strategy, covered in depth in CM1.6.
The practical application of this module's concepts is most visible when a doctor encounters a patient with a preventable condition. A child with recurrent diarrhoeal disease reflects not only a clinical problem but a failure of water sanitation, hand hygiene practices (behavioural determinant), and possibly poverty (socioeconomic determinant). The public-health-minded doctor reports the cluster of cases (surveillance), refers the family for safe water intervention, and advocates at the PHC level for a sanitation drive — acting simultaneously as clinician and community health resource. This dual role is the signature contribution of Community Medicine to medical education.