Page 9 of 25
CM1.6 | CM1.6 | Health Promotion, IEC and BCC — SDL Guide
Learning Objectives
- Define health promotion and describe its scope using the Ottawa Charter framework
- Explain the five action areas and three strategies of the Ottawa Charter (1986)
- Describe health education, its principles, and its methods (individual, group, mass)
- Distinguish between IEC and BCC and explain the concept of Behaviour Change Communication
- Describe the steps in designing an effective health communication campaign
- Apply health promotion and IEC/BCC principles to clinical and community settings
INSTRUCTIONS
The gap between knowing what is healthy and actually doing it is one of the oldest puzzles in medicine. Millions of people know that smoking causes cancer — yet they continue smoking. Millions know they should vaccinate their children — yet vaccine hesitancy persists. Health promotion, IEC, and BCC are the sciences and arts of closing this gap. This module explores how public health communicates with individuals and communities to produce sustainable, healthy behaviour change. These are skills you will use every day as a clinician, not only in community outreach.
References
- Park's Textbook of Preventive and Social Medicine, 26th edition — Ch on Health Education, IEC and Communication (textbook)
- Ottawa Charter for Health Promotion, WHO, 1986 (document)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
In 2012, India launched a massive IEC campaign to promote hand hygiene with soap — simple messaging, wall paintings in villages, radio spots in regional languages. Within two years, measurable increases in self-reported hand-washing with soap were documented in targeted districts, and diarrhoeal disease notifications fell. No drug was prescribed. No surgery was performed. The intervention was information, communication, and community mobilisation — yet the health impact in terms of children's lives was comparable to a new vaccine. This is the power of health promotion and behaviour change communication, and why every doctor must understand it.
WHY THIS MATTERS
India's largest disease burdens — tuberculosis, malnutrition, vaccine-preventable diseases, and the rising tide of non-communicable diseases — share a common thread: they are all powerfully influenced by knowledge, attitudes, and behaviour at the individual and community level. A doctor who can prescribe anti-TB drugs but cannot communicate adherence importance, or who can diagnose malnutrition but cannot counsel a mother on complementary feeding, is equipped for only half the job. This module gives you the theoretical foundation and practical framework for the communication half — which, in public health terms, often generates more impact than the pharmacological half.
RECALL
You have already learned, in the earlier modules of this cluster, that the determinants of health (CM1.2) include behavioural and socioeconomic factors — and that primary prevention (CM1.5) includes health promotion as one of its two main modes (alongside specific protection). Recall that primary prevention acts during the prepathogenesis stage — before disease begins — which is precisely when behaviour change is most impactful and cost-effective. As you read this module, connect each concept back to those frameworks: health promotion and IEC/BCC are the mechanisms through which primary prevention's 'health promotion mode' actually works in practice.
The Burden of Preventable Behaviour-Related Disease
A substantial proportion of the global and Indian disease burden is attributable to modifiable behaviours — tobacco use, unhealthy diet, physical inactivity, alcohol consumption, unsafe sexual practices, and poor hygiene — rather than to factors outside an individual's control. The Global Burden of Disease studies consistently show that behavioural risk factors account for a larger share of disability-adjusted life years (DALYs) than any single pathogen. In India, tobacco alone is estimated to cause over one million deaths annually, and malnutrition driven partly by inadequate infant feeding practices contributes to approximately 45% of child deaths under age five.
Yet knowledge of these risks does not automatically translate to behaviour change. Research consistently shows that health knowledge alone is a weak predictor of health behaviour: people may know that tobacco is harmful but continue to smoke because of addiction, social norms, stress, and perceived invulnerability. This knowledge-action gap is the central problem that health promotion, health education, IEC, and BCC are designed to bridge. Approaches that simply provide information — awareness campaigns, pamphlets, lectures — have limited effectiveness when used alone, without addressing the deeper determinants of behaviour such as self-efficacy, social norms, perceived benefit, and structural access. This evidence-base is the rationale for moving from simple health education toward the broader, multi-pronged frameworks of health promotion and BCC.
Health Promotion — Concept and Ottawa Charter Framework
Health promotion is defined by the WHO as 'the process of enabling people to increase control over, and to improve, their health.' This definition, central to the Ottawa Charter for Health Promotion (1986), is deliberately empowerment-focused: health promotion does not do health for people — it builds the conditions and capabilities for people to make health-promoting choices. The Ottawa Charter emerged from the first International Conference on Health Promotion and remains the foundational global framework, adopted across WHO member states including India.
The Ottawa Charter articulates health promotion through five action areas:
1. Building healthy public policy: embedding health in the decisions of all sectors — not just health ministries — through legislation, taxation (e.g. tobacco tax), and regulations that make the healthy choice the easy choice.
2. Creating supportive environments: making physical and social environments conducive to health — clean air standards, sanitation infrastructure, safe workplaces, accessible recreational spaces.
3. Strengthening community action: empowering communities to set their own health priorities, make decisions, and plan and implement actions — rather than imposing top-down programmes.
4. Developing personal skills: providing health information and education that builds the knowledge, attitudes, and skills people need to make health-promoting choices.
5. Reorienting health services: shifting health services from a purely curative, disease-treatment orientation toward prevention, health promotion, and community engagement.
The Charter also articulates three strategies that underpin all five action areas: advocate (creating the social, political, and economic conditions for health — the 'preconditions'); enable (reducing inequities so that all people can reach their full health potential); and mediate (reconciling the interests of different sectors — commerce, media, government — in pursuit of health).
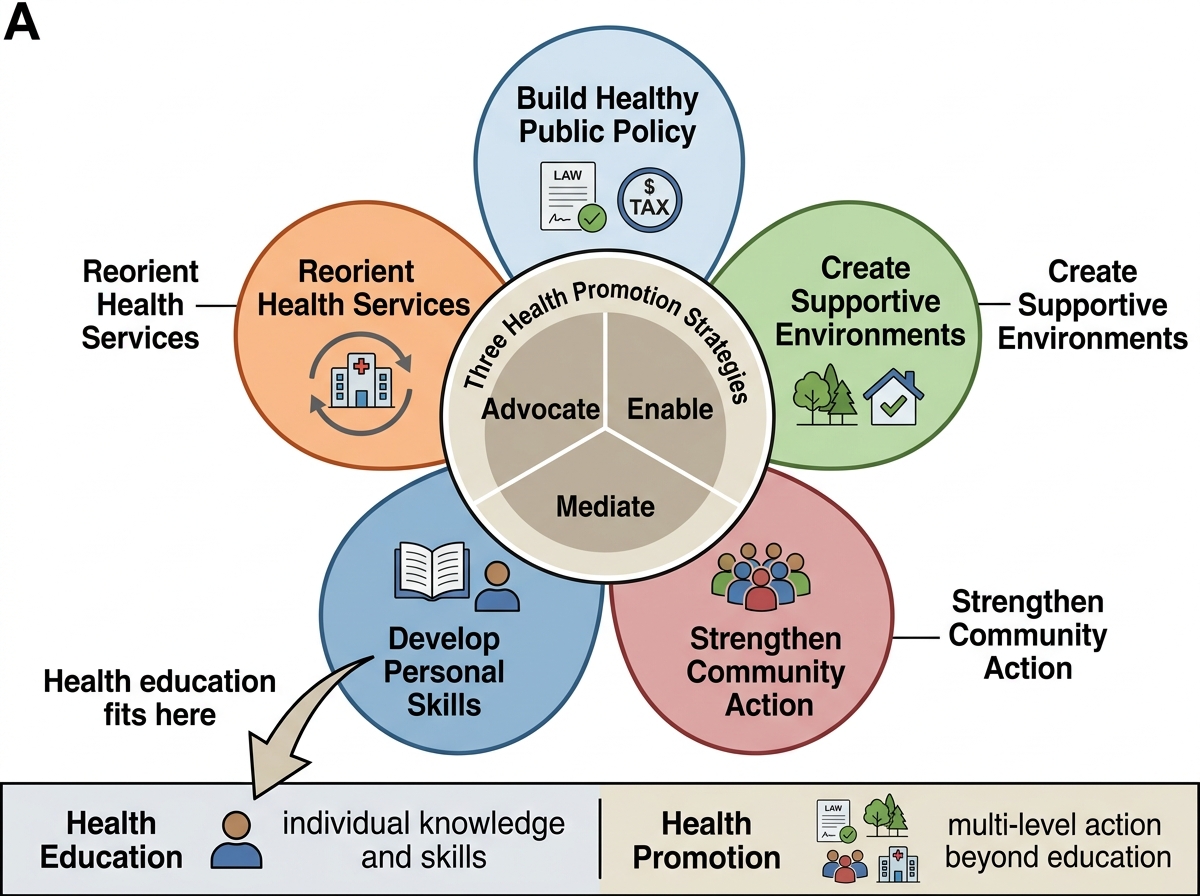
Ottawa Charter Framework for Health Promotion
Health promotion is critically distinct from health education: health education is a tool within health promotion (the 'developing personal skills' action area), but health promotion as a whole operates at the policy, environmental, community, and service levels simultaneously — far beyond the educational encounter between a provider and an individual.
SELF-CHECK
A state government enacts a law banning tobacco sales within 100 metres of schools and levies a 40% tax on tobacco products. This action exemplifies which Ottawa Charter action area?
A. Developing personal skills
B. Strengthening community action
C. Building healthy public policy
D. Reorienting health services
Reveal Answer
Answer: C. Building healthy public policy
Legislation and taxation that make tobacco use harder and more expensive are classic examples of building healthy public policy — embedding health considerations into governmental and institutional decisions. Developing personal skills would involve individual education; community action would involve community-initiated programmes; reorienting health services would involve changing the focus of the healthcare system itself.
Health Education — Principles, Methods, and KAP
Health education is a component of health promotion specifically directed at voluntary behaviour change by increasing health-related knowledge, changing attitudes (beliefs and values about health), and building practice (health skills). This KAP framework — Knowledge, Attitudes, and Practice — is the foundational theory underlying health education: the assumption is that informed individuals who hold positive attitudes toward healthy behaviour will adopt healthy practices. While this model is a simplification (attitude change does not always predict behaviour), it provides a practical structure for designing educational interventions.
Health education methods are classified by the size of the audience:
Individual-level methods: one-to-one communication between health provider and patient/client. Examples include patient counselling at the outpatient clinic, home visits by ASHAs, and bedside teaching. Advantages: personalised, interactive, responsive to individual questions and concerns. Limitations: time-intensive, reaches only one person at a time, not scalable for population-level change.
Group-level methods: directed at small to medium groups. Examples include health talks at PHC waiting areas, village meetings (gram sabha), mothers' group sessions, and school health education classes. Advantages: peer interaction promotes discussion and social norm influence; more efficient than one-to-one; allows question-and-answer and demonstration. Limitations: requires facilitation skills; more difficult to tailor to individual needs.
Mass-level methods: broadcast or print media directed at large audiences. Examples include television and radio public service announcements, newspaper campaigns, internet/social media, posters, and billboards. Advantages: reaches large numbers simultaneously, cost-effective per person reached. Limitations: non-interactive, difficult to tailor; message comprehension depends on audience literacy and media access; limited evidence for behaviour change without reinforcing personal contact.
| Method Level | Examples | Advantages | Limitations |
|---|---|---|---|
| Individual | Patient counselling, home visits | Personalised, interactive | Not scalable, time-intensive |
| Group | PHC talks, village meetings, school sessions | Peer interaction, discussion | Needs facilitation, moderate reach |
| Mass | TV/radio PSA, posters, social media | Large reach, cost-effective | Non-interactive, passive reception |
Research on health education effectiveness consistently shows that combined methods — personal contact reinforced by mass media — achieve the best results. Mass media creates awareness and sets the social agenda; face-to-face contact provides the personalised motivation, skills, and support needed for actual behaviour change.