Page 10 of 25
CM1.6 | CM1.6 | Health Promotion, IEC and BCC — SDL Guide (Part 2)
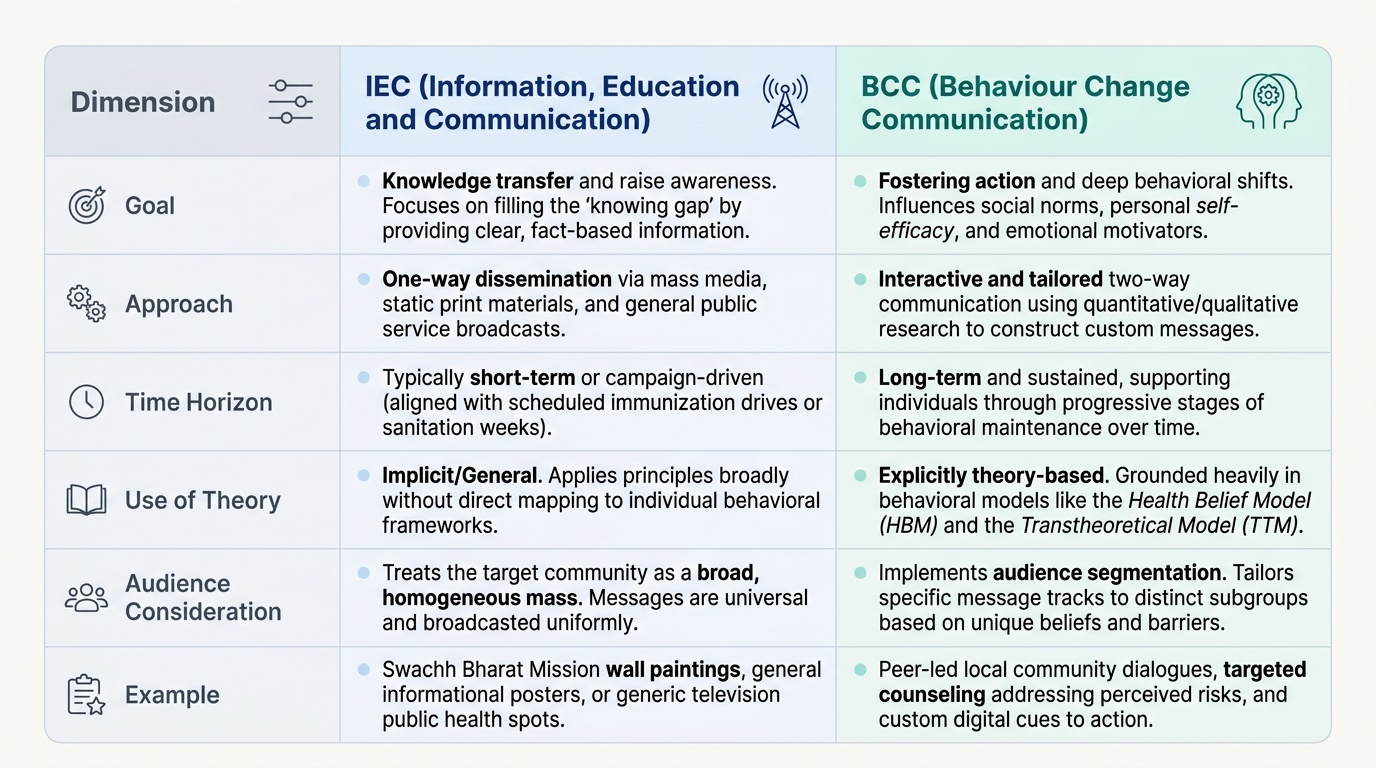
IEC and BCC — From Information to Behaviour Change
IEC (Information, Education and Communication) refers to the systematic and planned use of communication strategies, channels, and media to provide information and promote behaviour change in support of public health goals. IEC encompasses health education methods (individual, group, mass) and is applied widely in Indian national health programmes — immunisation drives, sanitation campaigns, nutrition promotion, and HIV awareness. The Swachh Bharat Mission's wall painting and inter-personal communication campaigns are a large-scale recent example.
BCC (Behaviour Change Communication) is a more evolved framework that goes beyond information delivery. While IEC primarily aims at knowledge transfer (addressing the 'knowing' gap), BCC explicitly addresses the deeper determinants of behaviour — social norms, self-efficacy, perceived risk, emotional motivators, and environmental barriers. BCC uses formative research (qualitative and quantitative investigation of the target audience's beliefs, norms, and barriers before designing messages), audience segmentation (recognising that different sub-groups need different messages and channels), and theory-based design (applying behavioural change models to message construction).
Provided image
Key behavioural models that underpin BCC:
Health Belief Model (HBM) — Rosenstock (1966, revised by Becker 1974): a person is more likely to take a health action if they perceive: (a) susceptibility to the condition, (b) severity of the condition, (c) benefits of the action outweighing (d) barriers to taking it, with a cue to action (trigger) present and adequate self-efficacy (confidence in ability to act). IEC messages that create perception of risk (susceptibility + severity) and demonstrate benefits while addressing barriers are grounded in the HBM.
Transtheoretical Model (TTM / Stages of Change) — Prochaska & DiClemente (1982): behaviour change is not a binary event but a journey through stages: precontemplation (no intention to change), contemplation (considering change), preparation (planning to change), action (making the change), and maintenance (sustaining the change). BCC strategies must match the message to the audience's current stage — there is no point providing skills-training to someone in precontemplation who does not yet see a reason to change.
Social Cognitive Theory (Bandura, 1977): emphasises self-efficacy (belief in one's own ability to perform a behaviour) and observational learning (modelling — seeing respected others perform the behaviour) as the most powerful predictors of behaviour change. BCC campaigns that use community 'role models' — respected local figures demonstrating hand-washing, breastfeeding, or exercise — apply social cognitive theory.
SELF-CHECK
A mother of a 6-month-old knows breast milk is best but is not breastfeeding exclusively because she believes she does not have enough milk. According to the Health Belief Model, this barrier is best described as low:
A. Perceived susceptibility
B. Perceived severity
C. Self-efficacy
D. Cues to action
Reveal Answer
Answer: C. Self-efficacy
The mother's belief that she 'doesn't have enough milk' is a belief that she CANNOT successfully breastfeed — this is low self-efficacy (confidence in the ability to perform the behaviour). Perceived susceptibility refers to perceived risk of a disease; perceived severity is the perceived seriousness of that disease; cues to action are triggers prompting the health behaviour. The BCC response would be to address self-efficacy through lactation counselling, peer support, and role-model demonstrations.
Designing Effective Health Communication Campaigns
Effective health communication does not happen by chance — it follows a systematic design process. The most widely used framework in Indian public health, consistent with WHO and Ministry of Health guidance, involves the following steps:
Step 1 — Problem Analysis: Define the specific health problem, its magnitude and distribution, and the behaviours most closely associated with it. Which behaviours, if changed, would have the greatest impact on the disease burden?
Step 2 — Formative Research: Conduct qualitative (focus groups, in-depth interviews, community observation) and quantitative (KAP surveys) research with the target audience to understand their current knowledge, beliefs, perceived barriers, social norms, and preferred communication channels. This step is non-negotiable in BCC design — messages designed without formative research frequently miss the mark.
Step 3 — Audience Segmentation: Divide the target population into sub-groups with similar characteristics, needs, and barriers. A TB adherence campaign needs different messaging for a young urban professional vs a migrant labourer vs a tribal woman — their barriers, communication channels, and social norms differ significantly.
Step 4 — Message Development and Pretesting: Develop draft messages using the insights from formative research and behavioural theory. Pretest messages with representative samples of the target audience and revise based on comprehension, acceptability, and persuasiveness feedback.
Step 5 — Channel Selection: Match channels to audiences — health workers for interpersonal communication; community radio for rural populations; social media for urban youth; wall paintings for low-literacy settings. Multi-channel strategies are most effective.
Step 6 — Implementation and Monitoring: Roll out the campaign with a process monitoring system (tracking activities, coverage, and reach) to identify implementation gaps in real time.
Step 7 — Outcome Evaluation: Measure changes in KAP (knowledge, attitudes, practice) using KAP surveys with pre/post or control-comparison designs. The ultimate evaluation is change in health outcome (morbidity, mortality), though this requires longer follow-up and is harder to attribute to communication alone.
Evaluating Health Promotion and IEC/BCC Programmes
Evaluation of health promotion and communication programmes uses a framework that distinguishes between different types of outcomes at different time points. The four evaluation categories are:
Process evaluation assesses whether the programme was implemented as planned — number of sessions conducted, materials distributed, health workers trained, communities reached. It answers: 'Did we do what we said we would do?' Process data come from programme records, supervision reports, and activity logs.
Output evaluation measures the immediate, direct products of the programme — for example, the number of immunisation sessions held, IEC materials produced, or individuals counselled. Outputs are necessary but not sufficient: high outputs do not guarantee behaviour change.
Outcome evaluation measures changes in the intermediate variables that the programme targeted — usually KAP (knowledge, attitudes, and practices), service utilisation (immunisation uptake, antenatal visit rates, hand-washing frequency). These are measured through KAP surveys — pre/post surveys using validated questionnaires administered to representative samples of the target population before and after the programme.
Impact evaluation measures changes in the ultimate health outcome — disease incidence, mortality rates, nutritional status. Impact evaluation requires longer timeframes (often years), control comparison groups, and careful attribution — since many factors beyond the communication programme influence health outcomes simultaneously.
For the NMC MBBS curriculum, students should understand the KAP survey as the primary evaluation tool for health education and IEC programmes: it directly measures the programme's stated objectives (change in knowledge, change in attitudes, change in practices), and its design (sampling, baseline, follow-up, control comparison) is a standard subject of community medicine practical exercises.
SELF-CHECK
A district conducts a KAP survey before and after a 6-month IEC campaign on hand hygiene. The survey finds a 30% increase in 'intention to wash hands with soap' but only a 12% increase in actual observed hand-washing. What does this most likely reflect?
A. The campaign was poorly implemented and should be repeated
B. Attitude change does not automatically translate to behaviour change — barriers beyond intention must be addressed
C. The KAP survey methodology was flawed and results are unreliable
D. IEC is inherently ineffective for hygiene promotion
Reveal Answer
Answer: B. Attitude change does not automatically translate to behaviour change — barriers beyond intention must be addressed
The gap between stated intention and actual observed behaviour is the classic 'intention-behaviour gap' — a well-documented phenomenon in health behaviour research. Intention to change (attitude) is a necessary but not sufficient predictor of actual behaviour change. Structural barriers (soap availability, water access), social norms, and habitual behaviours moderate the intention-behaviour link. This is exactly why BCC, which addresses these deeper determinants rather than just providing information, is more effective than simple IEC for sustained behaviour change.