Page 1 of 14
CM17.1-2 | CM17.1-2 | Community Health Care and Community Diagnosis — SDL Guide
Learning Objectives
- Define healthcare to the community and explain its philosophical basis
- Describe the concept of a 'community' in the public health context
- Define community diagnosis and distinguish it from clinical diagnosis
- Outline the steps and tools used to conduct a community diagnosis
- Explain how community diagnosis findings guide health programme planning
INSTRUCTIONS
India's healthcare system faces a paradox: thousands of highly skilled clinicians treating individual patients while preventable diseases devastate entire villages. This module explains why 'the community' — not just the patient — must be the unit of care, and equips you with the community diagnosis framework that every future medical officer, district health officer, and public health practitioner uses to identify where interventions are needed most.
References
- Park's Textbook of Preventive & Social Medicine, 27th ed., Ch. 1 & 14 (Community Health, Community Diagnosis) (textbook)
- WHO Alma-Ata Declaration, 1978 — Primary Health Care (policy)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Dr Priya, a newly posted medical officer at a Primary Health Centre in rural Maharashtra, notices something alarming in her first week: the same families return month after month with diarrhoeal illness, malnutrition, or skin infections — only to be treated and sent home, then return again. The individual prescriptions are correct. Yet the cycle never breaks. She realises she is treating the same problem repeatedly at the patient level while the root causes — a contaminated hand-pump, poor sanitation, low vaccination uptake in a specific hamlet — remain untouched at the community level. To fix the pattern, she must first understand the health status of her entire community: who is falling ill, why, where, and how often. This is the starting point of community medicine.
WHY THIS MATTERS
As a future MBBS graduate you will work in settings — PHCs, CHCs, urban health posts, district hospitals — where your decisions affect hundreds or thousands of people simultaneously, not just the patient in front of you. Community health competencies (CM17.1–17.2) underpin your role as a Medical Officer responsible for population health: you must be able to define health problems in the community you serve, prioritise them, and plan interventions. These skills are tested in MCI competency-based assessments and are directly applied in the NEET-PG practical and community field postings.
RECALL
Before we proceed, recall two prior concepts from your Community Medicine and Epidemiology sessions:
- Epidemiology is the study of the distribution and determinants of health and disease in populations — the scientific foundation of community medicine.
- Social determinants of health — income, education, housing, water supply, sanitation, and social support systems — often explain why communities (not just individuals) experience poor health. These are the upstream factors that community diagnosis seeks to quantify.
The Burden of Poor Community Health — Why Populations, Not Just Patients
A community, in the public health sense, is a group of people who share a common geography, culture, occupation, or interest and interact with each other over time. The term is not limited to villages: an urban slum, a tribal cluster, a factory workforce, or a school population can each constitute a community for health purposes. What matters is that they share health risks and are amenable to collective interventions.
Community health refers to the health status of a defined population as a whole — it is more than the sum of individual health conditions. When individual clinical care cannot reach the scale of a health problem, community-level action becomes essential. India's disease burden illustrates this starkly: according to the Global Burden of Disease study, communicable diseases including tuberculosis, diarrhoeal illness, and malaria continue to account for a disproportionate burden among rural populations, while non-communicable diseases are rising rapidly in urban areas. A medical practitioner focusing only on individual patients cannot reverse these trends; systematic, population-oriented healthcare delivery is required.
The philosophical basis of healthcare to the community rests on five components of care:
- Promotive care: improving the general level of health and wellbeing (nutrition education, sanitation promotion)
- Preventive care: specific protection against disease (immunisation, vector control, antenatal care)
- Curative care: treatment of established illness (OPD, indoor care, essential medicines)
- Rehabilitative care: restoring function after illness or injury (physiotherapy, prosthetics, community-based rehabilitation)
- Palliative care: relief of suffering in terminal illness
All five components must be available and accessible to a community for healthcare to be truly comprehensive. In India, the Sub-Centre → PHC → CHC → District Hospital hierarchy is designed to deliver this spectrum.
Determinants of Community Health Status
Community health status does not arise from chance — it is shaped by a web of interacting determinants that operate at multiple levels. Understanding these determinants is the first step toward changing them.
Park classifies determinants of health into four broad groups:
- Biological determinants: age, sex, genetic endowment, and physiological states (pregnancy, immunity). These are largely fixed at the individual level but create predictable patterns at the population level (e.g., under-5 children have higher vulnerability to diarrhoeal disease; post-menopausal women have higher cardiovascular risk).
- Behavioural and lifestyle determinants: diet, physical activity, tobacco use, alcohol consumption, sexual behaviour, and healthcare-seeking behaviour. These are modifiable and are the primary targets of health promotion programmes (e.g., NPCDCS lifestyle modification campaigns, tobacco control under NTCP).
- Environmental determinants: physical environment (air quality, water supply, sanitation, housing), biological environment (disease vectors, reservoirs), and social environment (poverty, social cohesion, crime). Environmental factors explain geographic clustering of disease — diarrhoeal illness clusters around contaminated water sources; malaria clusters in vector-breeding habitats.
- Socioeconomic and health-system determinants: income, education, employment, social support, access to healthcare, quality of services, and health policies. These operate as upstream drivers — low income reduces access to nutritious food, safe housing, and timely care, amplifying all other risk factors.
A hallmark of community medicine is that these determinants interact: poverty → poor sanitation → increased infection risk → malnutrition → further vulnerability. Effective community health programmes must address multiple determinants simultaneously rather than targeting a single risk factor in isolation. This multi-determinant view is what separates a public health perspective from a purely clinical one.
SELF-CHECK
A 32-year-old woman in a village returns to the PHC for the third time in six months with acute diarrhoea. Each time she was treated and recovered. From a community health perspective, what is the MOST appropriate next step for the medical officer?
A. Prescribe a longer course of antibiotics at this visit
B. Refer her to a district hospital for specialist evaluation
C. Initiate a community diagnosis to identify the source and extent of diarrhoeal illness in the village
D. Advise her to boil water and improve personal hygiene only
Reveal Answer
Answer: C. Initiate a community diagnosis to identify the source and extent of diarrhoeal illness in the village
Repeated cases of the same illness in a geographic cluster signal a community-level problem (likely contaminated water or poor sanitation) rather than a purely individual issue. The correct response is community diagnosis — identifying the problem at the population level, its magnitude, distribution, and cause — so that a targeted intervention (e.g., repairing the hand-pump, promoting sanitation) can break the cycle. Treating individuals in isolation and advising only personal hygiene does not address the upstream environmental determinant.
Community Diagnosis — Concept, Objectives, and Methods
Community diagnosis is the process of describing the health status of a community, identifying its health problems, and determining the priority order for addressing them, using epidemiological methods and community data. The term was popularised by Kark and Cassel in the 1950s and is now a core competency for medical officers in India under NMC's CBME framework.
The analogy with clinical diagnosis is intentional and instructive. Just as a clinician takes a history, examines the patient, orders investigations, and arrives at a diagnosis before prescribing, a community physician takes a 'history' of the community (demographic, socioeconomic, environmental data), 'examines' it (surveys, field observations), analyses 'investigations' (vital statistics, morbidity records), and arrives at a community diagnosis before planning programmes.
Provided image
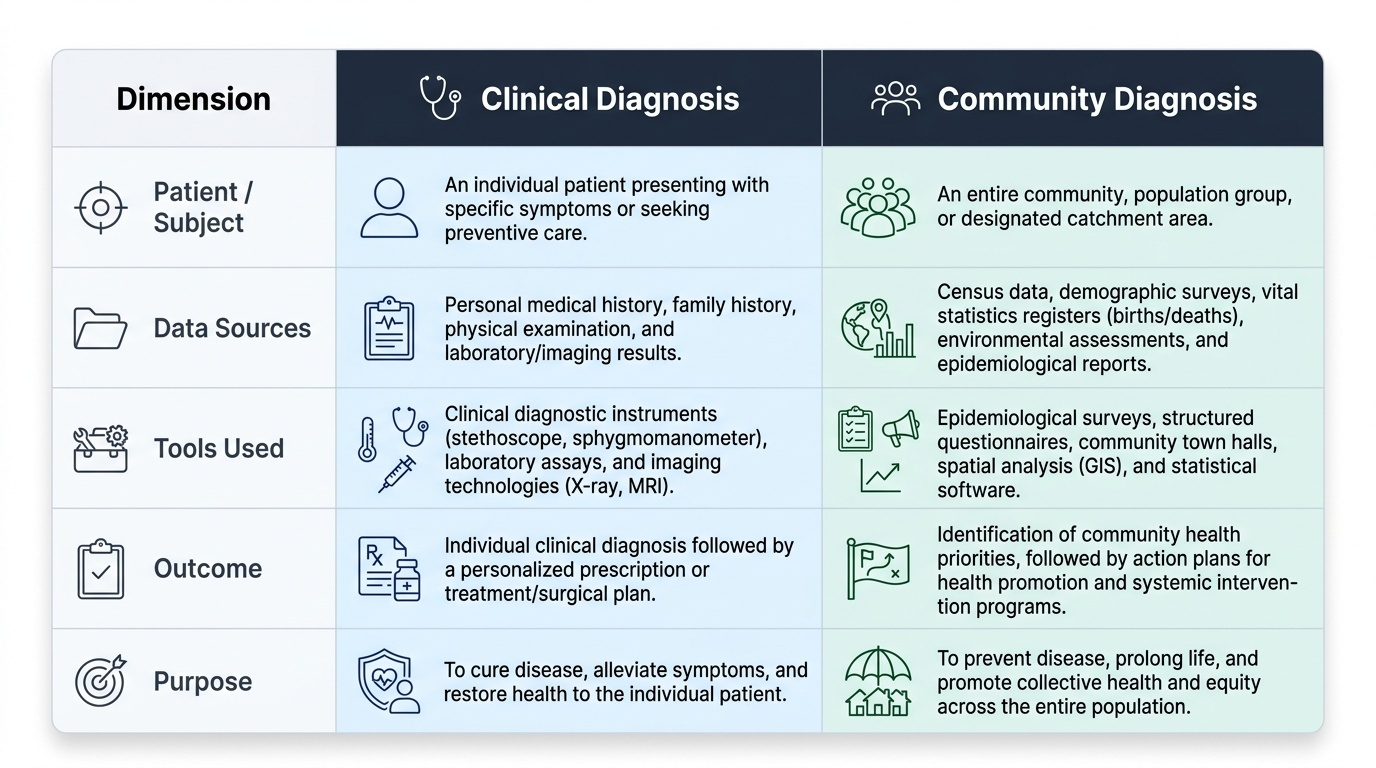
| Dimension | Clinical Diagnosis | Community Diagnosis |
|---|---|---|
| Subject | Individual patient | Defined community/population |
| Data sources | History, examination, lab tests | Vital statistics, surveys, disease registries |
| Tools | Physical examination, imaging | Epidemiological methods, health indices, GIS |
| Outcome | Diagnosis of a disease | Identification of priority health problems |
| Purpose | Treat the patient | Plan community health programmes |
Objectives of community diagnosis:
1. To describe the health status of the community (morbidity, mortality, disability profile)
2. To identify the major health problems and their distribution across age, sex, geography
3. To identify the health determinants (risk factors, social conditions) responsible for the problems
4. To set priorities for action based on magnitude, severity, community concern, and feasibility of intervention
5. To provide a baseline for monitoring the effect of interventions over time
Key data sources used in community diagnosis:
- Census data (population structure, literacy, housing)
- Vital registration system (birth rate, death rate, cause-specific mortality)
- Notifiable disease records (from PHC/district)
- Hospital records (OPD attendance patterns, admission diagnoses)
- National health surveys (NFHS-5 for India: maternal health, child nutrition, anaemia prevalence)
- Special epidemiological surveys (household surveys, outbreak investigations)
- HMIS (Health Management Information System) data from PHC