Page 4 of 11
CM4.3-4 | CM4.3-4 | Health Education Session Design and Evaluation — SDL Guide
Learning Objectives
- Describe and demonstrate the steps in evaluating a health promotion and education programme (CM4.3)
- Plan and conduct a health education session for community awareness in a simulated environment, FAP, or clinical posting (CM4.4)
- Apply Bloom's taxonomy to write clear, measurable objectives for a health education session
- Use appropriate evaluation tools — KAP questionnaires, observation checklists, and programme indicators — to assess session and programme effectiveness
INSTRUCTIONS
You will conduct your first real health education session in the Field Practice Area before your MBBS final examinations. This module gives you the blueprint for doing it well: how to identify what a community actually needs to know, how to design a session that matches that need, how to facilitate it in a way that actually changes practice — and crucially, how to evaluate whether it worked. Evaluation is not an optional academic exercise; it is the mechanism by which every health programme learns and improves. This is your opportunity to think like a public health professional rather than just a knowledge-provider.
References
- Park K. Park's Textbook of Preventive and Social Medicine, 27th ed. Ch. 18 — Health Education and Promotion (textbook)
- Kirkpatrick DL & Kirkpatrick JD. Evaluating Training Programs: The Four Levels, 3rd ed. (2006) (framework)
- Green LW & Kreuter MW. PRECEDE-PROCEED Model for Health Program Planning and Evaluation (1991) (model)
- Bloom BS. Taxonomy of Educational Objectives: The Classification of Educational Goals (1956); revised by Anderson & Krathwohl (2001) (taxonomy)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
At a district health review meeting, the Chief Medical Officer presents data: over the past year, health workers in the district conducted 2,400 health education sessions — one at every Village Health and Nutrition Day across all sub-centres. Yet the full immunisation coverage in the district remained unchanged at 62%, and open defecation declined by only 2%. The CMO turns to the assembled medical officers and asks: 'What happened?' An audit reveals that almost no session had a written session plan, almost none used a pre-post knowledge test, and virtually all sessions consisted of the health worker reading from a pamphlet to a group of women who nodded politely. A lot of activity. Almost no learning. Zero practice change. This is the problem that session design and evaluation exist to solve.
WHY THIS MATTERS
Session design and evaluation are the competencies that distinguish a health worker who conducts activities from one who achieves outcomes. These are directly assessed in your MBBS examinations: CM4.3 requires you to 'demonstrate and describe the steps in evaluation of a health promotion and education program' — tested via Written examination, Viva voce, Skill Assessment, and OSCE. CM4.4 requires you to 'conduct a health education session for community awareness in a simulated environment/FAP/clinical posting' — observed and marked in your Field Practice Area. In your career as a Medical Officer at a PHC, you will be responsible for training ASHAs and ANMs to conduct sessions, reviewing their session plans, and interpreting HMIS data on programme outcomes. This module gives you the conceptual and practical tools for all of these roles.
RECALL
Connect to your earlier learning before we move to session design:
From the Methods of Health Education module (CM4.1/4.2): The three-tier method classification (individual/group/mass) is your method menu — session design is the process of selecting and organising methods from this menu. The KAP framework (Knowledge → Attitude → Practice) defines what a session is trying to change at each level.
From general education theory: You have encountered Bloom's Taxonomy in your study skills orientation. It classifies learning objectives into: cognitive (knowing), psychomotor (doing), and affective (feeling/valuing). Health education sessions aim to change all three domains — but most sessions only address the cognitive, which is why practice change is rare.
From your FM/PSM orientation: Recall the Epidemiological Triad — host, agent, environment. A needs assessment for session design asks: what host-level behaviours (knowledge gaps, risky practices), agent-level threats, or environmental barriers need to be addressed?
The Gap Between Intent and Impact in Health Education
The public health literature consistently documents a large gap between the number of health education activities conducted and measurable changes in community health behaviour. India's National Health Mission supports lakhs of community-level interactions per year — VHND sessions, school health talks, anganwadi group meetings, ANC health education at sub-centres — yet behaviour change indicators (institutional delivery, full immunisation, ODF village status, tobacco cessation) often lag far behind the volume of activity.
The root cause of this gap, as documented in field evaluations, is the absence of systematic session design and evaluation. Sessions conducted without a written session plan tend to drift — the health worker covers topics they are comfortable with rather than what the audience needs. Sessions conducted without a pre-test miss the baseline — the health worker cannot know what changed. Sessions conducted without audience interaction confirm no learning — participants may have understood nothing but never said so.
This gap is not unique to India. Kirkpatrick's foundational research on training effectiveness demonstrated that the majority of organisational training programs in the United States were evaluated only at the Reaction level (did participants like the session?) and almost never at the Learning, Behaviour, or Results levels. The same pattern applies to health education globally: smiley-face feedback forms replace KAP measurement, and no one asks whether the group that attended the session actually changed their practices compared to a group that did not.
Understanding this gap is the motivation for the structured approach to session design and evaluation that this module teaches. Every step in the process exists because an unstructured alternative has been shown, in practice, to fail.
SELF-CHECK
A PHC Medical Officer reviews VHND registers and finds that all 12 monthly sessions on breastfeeding were conducted last quarter, with an average attendance of 15 mothers each. However, the sub-centre's exclusive breastfeeding rate at 6 months remains unchanged at 38%. Which type of evaluation finding most directly explains this discrepancy?
A. The process evaluation shows high session completion, but outcome evaluation is absent
B. The impact evaluation shows poor health outcomes at district level
C. The formative evaluation was not conducted before session design
D. The output evaluation shows inadequate attendance
Reveal Answer
Answer: A. The process evaluation shows high session completion, but outcome evaluation is absent
Session completion rates (all 12 sessions conducted) represent process evaluation — activities delivered as planned. The absence of outcome evaluation (no pre-post KAP measurement, no follow-up on behaviour change) means we cannot tell whether the sessions achieved any learning or practice change. This is the classic 'activity trap': strong process data with no outcome data, making programme improvement impossible. Option B (impact evaluation at district level) is a longer-term, population-level metric. Option C (formative evaluation) refers to the pre-design needs assessment phase. Option D (attendance) is actually adequate at 15 mothers per session.
Determinants of an Effective Health Education Session
An effective health education session does not happen by accident. Six determinants govern whether a session achieves its intended KAP change, and a systematic session design process addresses each one explicitly.
The first determinant is needs assessment quality. A session designed for a general 'community audience' without a specific needs assessment will be neither relevant nor useful. The facilitator must know, before designing the session: what is the specific health problem? Who is the target group (age, gender, occupation, literacy)? What do they already know, believe, and practise? What barriers prevent the desired behaviour? A rapid needs assessment — structured observation, focused group discussion, or a short five-question KAP pre-test — takes thirty minutes but determines the entire session direction.
The second determinant is objective clarity. Sessions designed around vague intentions ('to improve maternal health awareness') produce vague outcomes. Sessions designed around SMART objectives — Specific, Measurable, Achievable, Relevant, Time-bound — produce measurable outcomes. A SMART objective for a breastfeeding session might read: 'After this session, at least 80% of attending mothers will be able to correctly demonstrate the positioning and latch technique for breastfeeding (psychomotor domain, Bloom's application level).'
The third determinant is method–audience fit — whether the chosen method (demonstration, group discussion, drama, lecture) matches the audience's literacy level, size, preferred learning style, and the complexity of the behaviour being targeted. This is the same determinant framework from the previous module, applied specifically to session planning.
The fourth determinant is facilitator skill: the health worker's ability to establish rapport, ask questions that stimulate discussion, manage group dynamics, correct misconceptions without embarrassing participants, and keep the session to time. Facilitation skill is distinct from content knowledge — a doctor who lectures brilliantly may be a poor health education facilitator, while a well-trained ASHA with moderate content depth may produce excellent KAP change through skilled facilitation.
The fifth determinant is material quality: whether the IEC materials (flip charts, models, samples, demonstration kits) are locally appropriate, visually clear, at the right literacy level, and physically available and functional at the time of the session.
The sixth determinant is follow-up mechanism: whether the session is a one-off event or part of a series with home visit follow-up, a peer accountability structure, or a referral pathway that supports the behaviour change after the session ends. Single-session interventions have limited sustained impact; longitudinal follow-up is what converts knowledge into lasting practice.
Designing a Health Education Session: The Step-by-Step Process
A well-designed health education session follows a systematic five-step process that is directly assessable in OSCEs. The mnemonic NAPED captures all five steps and is easy to reproduce under examination conditions.
N — Needs Assessment: Before planning begins, conduct a rapid needs assessment to identify: (a) the health problem (What disease or risk behaviour is the priority?); (b) the target audience (Who will attend? What are their age, gender, literacy level, occupation, existing KAP?); (c) the contextual barriers (What prevents the desired behaviour? Is it lack of knowledge, a cultural belief, an access problem, or a social norm?). Tools include: key informant interviews with ANM/ASHA, focused group discussion with community members, a brief pre-test questionnaire, or review of HMIS data and previous session records.
A — Aims and Objectives: Write clear, measurable session objectives using Bloom's Taxonomy of educational objectives. Bloom's three domains apply to health education: (a) Cognitive domain — the knowledge the participant should gain (e.g., 'List the five danger signs of dehydration'); (b) Psychomotor domain — the skill the participant should be able to perform (e.g., 'Demonstrate correct ORS preparation'); (c) Affective domain — the attitude or value the participant should develop (e.g., 'Express willingness to use ORS for their child before seeking a doctor'). A well-written objective uses an action verb from the correct Bloom's level: remember, understand, apply, analyse, evaluate, create.
P — Planning: Prepare the session plan (lesson plan) which specifies: title, date/venue/time, target audience, objectives (from step A), content outline with time allocation, methods and materials for each segment, facilitator assignments, and evaluation tools. A standard 45-minute group session might be structured as: introduction/rapport (5 min) → recall/hook (5 min) → main content via demonstration or group discussion (20 min) → interactive Q&A + return demonstration (10 min) → summary + call to action (5 min). Materials are prepared in advance: demonstration kits, flip charts, pre-test and post-test questionnaires.
E — Execution (Implementation): Conduct the session as planned, with active facilitation — see the following heading for the conduct steps. Document attendance, participation, and any deviations from the session plan.
D — Documentation and Follow-up: Immediately after the session, record: attendance register, pre-test and post-test scores (if used), key questions raised by participants, any referrals made, and facilitator observations. Schedule follow-up: home visits within two to four weeks to reinforce the session message and observe behaviour change; re-entry in the next VHND register.
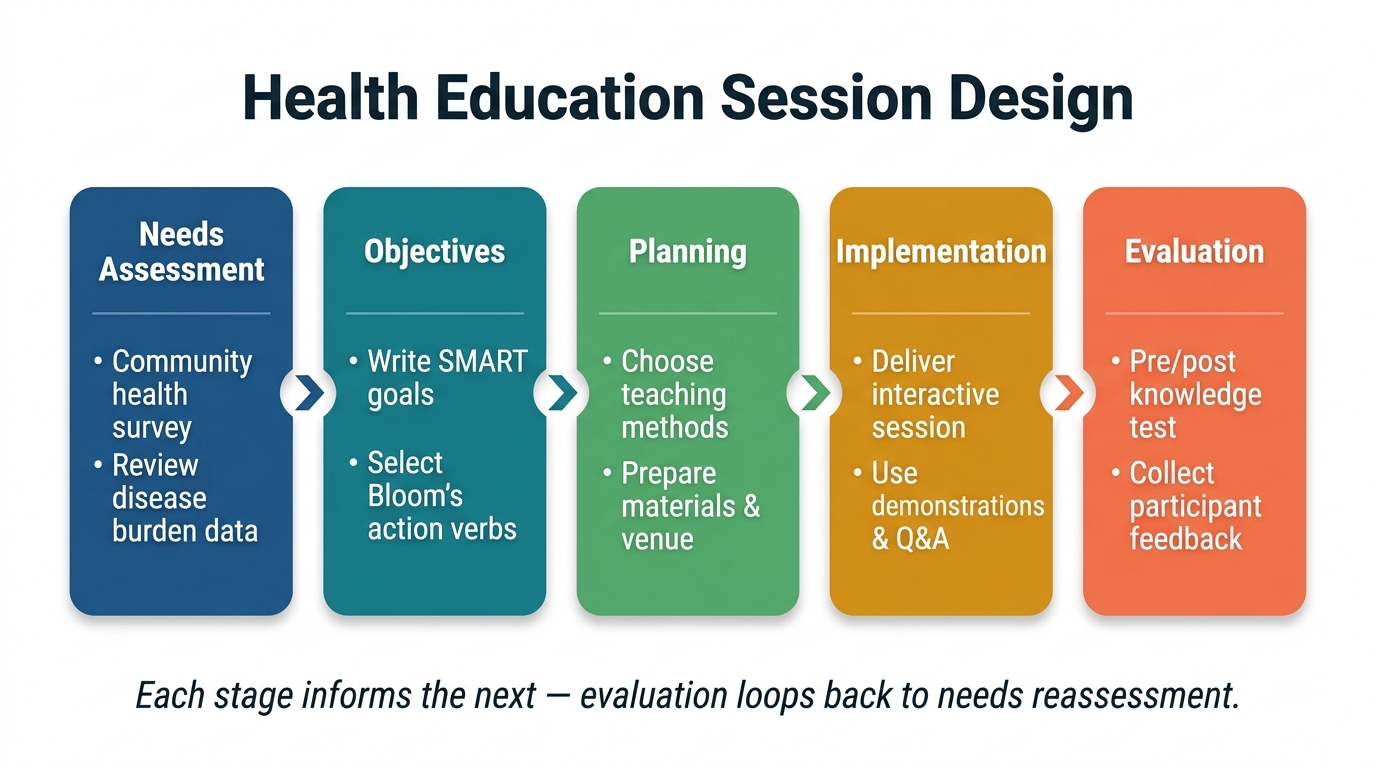
The Five-Stage Health Education Session Design Process
SELF-CHECK
A medical student is planning a health education session on dengue prevention for 15 school children aged 10–12. She writes the following objective: 'Children will know about dengue.' Using Bloom's Taxonomy, what is wrong with this objective, and which revision is MOST appropriate?
A. It targets the wrong audience; school children do not benefit from health education
B. It is not specific or measurable; a better objective is 'After the session, at least 80% of children will be able to describe three breeding sites of the Aedes mosquito'
C. It addresses the psychomotor domain; it should address the affective domain instead
D. It is too specific; a broader objective covers more learning needs
Reveal Answer
Answer: B. It is not specific or measurable; a better objective is 'After the session, at least 80% of children will be able to describe three breeding sites of the Aedes mosquito'
The objective 'Children will know about dengue' fails two SMART criteria: it is not Specific (which aspect of dengue?) and not Measurable (how do you determine if they 'know'?). A well-written objective uses a Bloom's action verb (describe, list, demonstrate, identify) at a specific cognitive/psychomotor/affective level, with a measurable threshold (at least 80%). Option B corrects both problems: it specifies the content (three breeding sites), uses a Bloom's verb (describe — comprehension level), and includes a measurable standard (80% of children). Option A is incorrect — school children benefit greatly from health education. Option C mismaps the domain — describing mosquito breeding sites is cognitive, not psychomotor. Option D reverses the principle — specificity is a virtue, not a fault.