Page 5 of 11
CM4.3-4 | CM4.3-4 | Health Education Session Design and Evaluation — SDL Guide (Part 2)
Conducting a Health Education Session: Facilitation Skills and Practical Steps
Conducting a health education session (CM4.4) is a distinct competency from designing one. The same session plan can produce very different outcomes depending on facilitation quality. The following steps describe how to conduct a session effectively in a FAP, clinical, or simulated environment.
Step 1 — Introduction and rapport (5 minutes): Welcome participants by name or group title, introduce yourself (role, not just name — 'I am your medical student from the community medicine posting; I am here to learn with you and share some health information'), and establish ground rules — it is a discussion, all questions are welcome, there are no wrong answers. If the group is new to you, use an icebreaker activity (ask each person their name and one health question they came with) to reduce power distance between facilitator and community.
Step 2 — Needs check and recall (3–5 minutes): Administer the pre-test (a short 5–10 item KAP questionnaire, or a verbal quiz) to establish baseline. Ask two or three open questions about existing practices: 'When your child had diarrhoea last monsoon, what did you give first?' These baseline answers shape the emphasis of the session in real time.
Step 3 — Content delivery using selected method (15–20 minutes): Deliver the pre-planned content using the selected method. For a demonstration: show the skill step-by-step, name each step, check for understanding, then ask a participant to repeat (return demonstration). For a group discussion: pose an open question, facilitate contributions, draw out the key teaching points from participants' answers before adding to them. Never lecture without interaction — pause for questions, use show-of-hands, call on participants by name.
Step 4 — Interactive reinforcement (10 minutes): Pose a scenario-based question, run a brief role play, or use a pictorial quiz to consolidate learning. This is the step most often skipped due to time pressure — and the most important for practice-level change. Research consistently shows that active learning (doing, applying) produces stronger retention than passive exposure.
Step 5 — Summary and call to action (5 minutes): Recap the three key messages of the session (no more than three — memory research shows recall drops sharply beyond this). Give a clear call to action: 'From today, when your child has diarrhoea, the first thing you will do is prepare ORS. Here is a packet to take home and practice with.' Where possible, leave a take-home material (a pictorial card, a pamphlet) that reinforces the message.
Step 6 — Post-test and close (5 minutes): Administer the same questionnaire as the pre-test (or a parallel form). Thank participants. Inform them of the follow-up plan. Document attendance and observations immediately — memory fades within hours.
Documentation of an observed session should include: venue, date, number and composition of attendees, methods used, pre-test and post-test scores, participant questions raised, and facilitator's self-assessment of what went well and what would be improved next time.
CLINICAL PEARL
The three-message rule. Research in cognitive psychology (Miller's Law — seven, plus or minus two; working memory capacity studies since Cowan) consistently shows that participants in a health education session remember a maximum of three key messages. Not five. Not seven. Three. Yet the average health education session covers between eight and fifteen points, and participants leave remembering none of them distinctly. When you design your FAP session, identify the three most important messages for your specific audience and ensure that every teaching activity, every image, and every interactive question reinforces one of those three. Write them on a card, post them on the flip chart, and summarise them explicitly at the end. Your participants will leave with those three messages; everything else is supporting detail.
Evaluation of Health Promotion and Education Programs
Evaluation is the step that converts a health education activity into a health education programme — one that learns, improves, and demonstrates accountability. CM4.3 specifically requires students to 'demonstrate and describe the steps in evaluation,' tested in both Written and OSCE formats. This heading covers the complete evaluation framework.
Types of evaluation are classified by timing and purpose: (a) Formative evaluation — conducted before or during programme design to inform planning (equivalent to needs assessment); identifies gaps, tests materials, pilots the session with a small group; (b) Process evaluation — measures whether the planned activities were delivered as intended: sessions held, attendance, facilitators trained, materials distributed; (c) Outcome evaluation — measures whether the programme changed knowledge, attitudes, or practices in the target population; uses pre-post KAP questionnaires, observation checklists, or focused group discussion; (d) Impact evaluation — measures change in disease or health outcome indicators attributable to the programme: immunisation coverage, ODF village status, tobacco cessation rates, maternal mortality; measured over a longer time horizon.
The KAP survey is the most common outcome evaluation tool in community health education. A structured questionnaire with five to ten items is administered before the session (establishing baseline) and after (measuring change). Items must match the session objectives: if the objective was 'participants will be able to list three danger signs of severe dehydration,' the post-test must ask exactly that. The percentage change in correct responses from pre to post is the primary outcome metric.
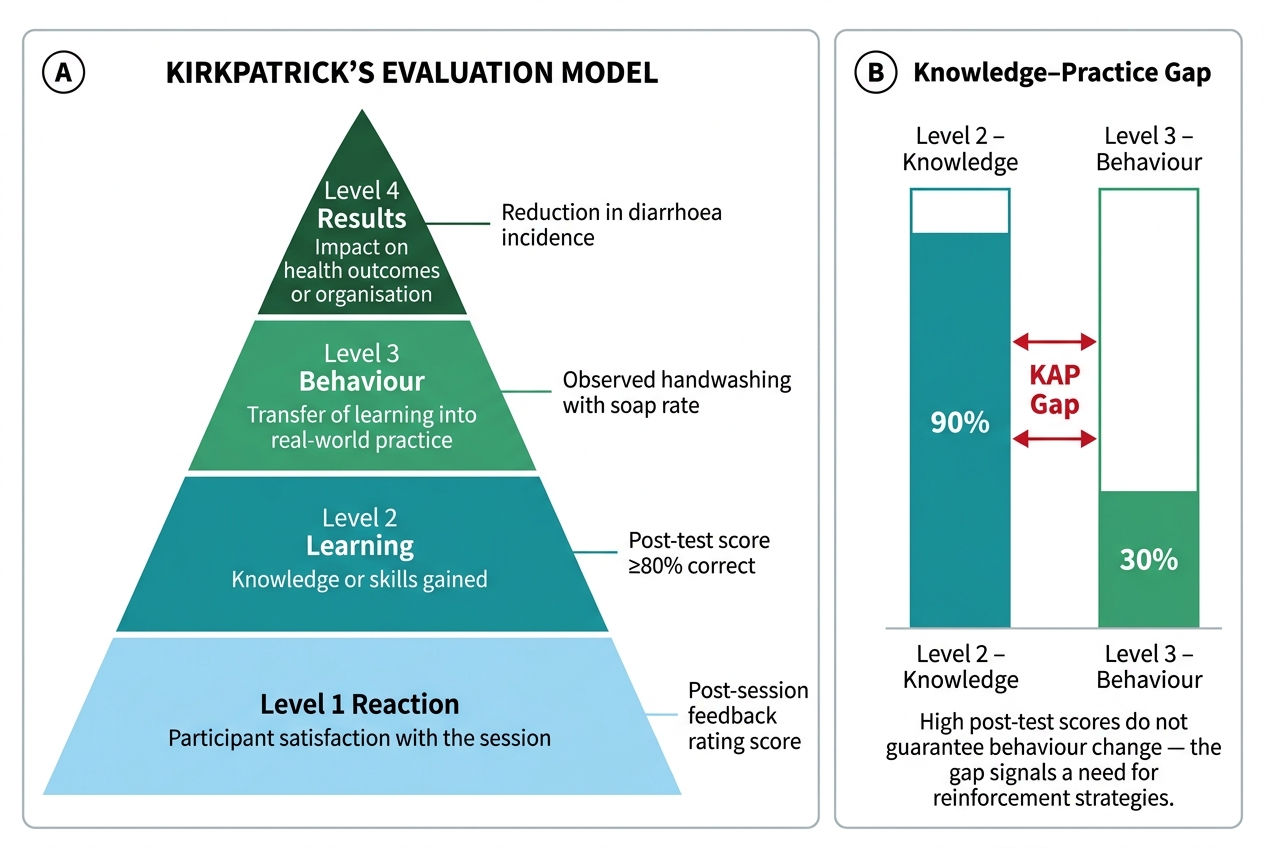
Kirkpatrick's Four-Level Evaluation Model, originally developed for training programme evaluation, maps directly onto health education: Level 1 = Reaction (did participants find the session useful and relevant? — measured by a brief feedback form immediately after the session); Level 2 = Learning (did participants gain knowledge or skills? — measured by the post-test); Level 3 = Behaviour (did participants actually change their practice? — measured by home visit observation or follow-up survey two to four weeks later); Level 4 = Results (did the programme achieve its health outcome? — measured by district/sub-centre health indicators three to six months later). Most health education sessions in India are evaluated only at Level 1 (a smiley-face register) — the reason for the gap documented at the start of this module.
The PRECEDE-PROCEED Model (Green and Kreuter) provides a broader framework for health programme planning and evaluation. PRECEDE (the diagnostic phase) works backwards from the desired health outcome to identify behavioural determinants, educational needs, and resource availability. PROCEED (the implementation and evaluation phase) works forward from policy/environmental/educational interventions to measured outcomes. For a Medical Officer planning a district-level health promotion programme, this model provides the full diagnostic-to-evaluation structure needed for a Programme Implementation Plan (PIP) submission.
Observation checklists are used specifically for skill-based outcomes (CM4.4) — evaluating whether a health worker correctly demonstrates a procedure (ORS preparation, hand-washing technique, counselling steps) or whether a community member correctly returns a demonstration. A standard observation checklist has ten to fifteen binary (yes/no) or rated (1–4) items corresponding to the key steps of the skill, with a minimum passing score.
Kirkpatrick's Four-Level Evaluation Model and the Knowledge–Practice Gap
SELF-CHECK
A medical student conducts a health education session on handwashing and collects a post-test showing 90% correct knowledge scores. Two weeks later, an ASHA reports that observed handwashing with soap practice in the village is still below 30%. Which Kirkpatrick evaluation level is the 90% post-test score measuring, and at which level is the ASHA's observation finding?
A. Post-test = Level 1 (Reaction); ASHA observation = Level 2 (Learning)
B. Post-test = Level 2 (Learning); ASHA observation = Level 3 (Behaviour)
C. Post-test = Level 3 (Behaviour); ASHA observation = Level 4 (Results)
D. Post-test = Level 4 (Results); ASHA observation = Level 1 (Reaction)
Reveal Answer
Answer: B. Post-test = Level 2 (Learning); ASHA observation = Level 3 (Behaviour)
In Kirkpatrick's model, Level 2 (Learning) measures whether participants actually gained knowledge or skills — exactly what a post-test knowledge questionnaire measures. Level 3 (Behaviour) measures whether participants transferred that learning into actual practice — which is what the ASHA's direct observation of handwashing practice captures. The gap between Level 2 (high knowledge) and Level 3 (low practice) is the classic knowledge-practice gap described in the KAP framework, and it signals that the intervention must now address the attitude or practice-level barriers, not repeat the knowledge-level session.
Applying Session Design and Evaluation in a Field Posting
Your Field Practice Area (FAP) posting at the sub-centre or Urban Health Training Centre will include an assessed health education session under CM4.4. This section translates the theoretical framework into a practical preparation guide for that experience.
Preparation (one week before): Confirm the topic with your faculty or PHC Medical Officer — choose based on a real seasonal or community need (monsoon = dengue/diarrhoea; winter = ARI; ongoing = immunisation; persistent = tobacco/alcohol in men; antenatal group = breastfeeding). Conduct a brief needs assessment: ask the ANM or ASHA what the community's most common questions or misconceptions are on this topic. Prepare your session plan (NAPED) in writing, including three SMART objectives, a 45-minute timeline, the methods you will use, the materials you need, and your pre-test and post-test questionnaires.
During the session: Follow the six facilitation steps (Introduction, Needs check, Content delivery, Interactive reinforcement, Summary + call to action, Post-test and close). Use the language of the community — if the local term for diarrhoea is different from textbook terminology, use both. Address the specific misconceptions the ANM flagged during your needs assessment. If you are conducting a demonstration, prepare your materials (ORS, measuring jug, clean water, salt, sugar) and rehearse before the session.
Immediately after the session: Score the pre-tests and post-tests. Calculate percentage correct change (e.g., pre-test 45% correct, post-test 80% correct = 35 percentage point improvement). Complete your documentation: attendance, key questions asked, any referrals made. Write a reflective one-page session report to submit to your faculty.
OSCE rubric orientation: Health education session OSCEs are typically assessed on: (a) appropriateness of method to audience (10 marks); (b) rapport and communication style (10 marks); (c) content accuracy (20 marks); (d) use of educational materials (10 marks); (e) participant interaction and active learning (20 marks); (f) summary and call to action (10 marks); (g) documentation/post-test (10 marks); (h) overall organisation within time (10 marks). Total 100 marks. The most common reason for marks deduction in CBME OSCEs is: one-way lecturing with no audience interaction, and failure to conduct or score a post-test.
Worked example: A batch of five students is posted at the sub-centre in October, monsoon season. The ANM reports high dengue case load. Needs assessment confirms: mothers know dengue is spread by mosquitoes (high knowledge) but few know that Aedes breeds in clean stored water indoors (low knowledge — a common misconception that it only breeds in dirty water). Session design: objective 1 = identify indoor breeding sites of Aedes mosquito (cognitive, knowledge level); objective 2 = demonstrate correct disposal of stored water containers (psychomotor); objective 3 = express commitment to a weekly dry-day practice at home (affective). Method: start with a pre-test (5 questions), show actual Aedes larvae in a small jar of clean water (demonstration to challenge the 'dirty water only' misconception), group discussion on where water accumulates at home, return demonstration of tipping out and turning over containers, post-test. Materials: larva jar, flip chart, pre-post test forms. Evaluation plan: post-test immediately, home visit in 2 weeks to observe container practices.