Page 8 of 15
CM11.5 | CM11.5 | Health Professional Occupational Disorders — SDL Guide
Learning Objectives
- Describe occupational disorders of health professionals and their prevention and management (CM11.5)
INSTRUCTIONS
Physicians, nurses, laboratory technicians, radiographers, anaesthetists, and every other healthcare worker are themselves workers exposed to occupational hazards — yet medical education rarely frames it this way. The hospital is one of the most hazardous workplaces: bloodborne pathogens, airborne tuberculosis, ionising radiation, anaesthetic gases, cytotoxic drugs, ergonomic overload, and psychosocial stress converge daily. This module builds your ability to recognise, prevent, and manage the occupational disorders specific to health professionals — starting from the needlestick that happens during your intern year.
References
- Park's Textbook of Preventive & Social Medicine, 26th ed. — Chapter: Occupational Health (textbook)
- WHO Post-Exposure Prophylaxis Guidelines 2014 (Supplement to 2013 ARV Guidelines) (guideline)
- NIOSH Alert: Preventing Occupational Exposures to Antineoplastic and Other Hazardous Drugs in Health Care Settings (2004) (guideline)
- AERB (Atomic Energy Regulatory Board) — Radiation Protection for Workers in Medical Facilities (guideline)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
It is 11 PM in the surgical ward. You are an intern assisting a senior resident in closing a post-appendicectomy wound. The suture needle slips. You feel a sharp prick through your glove — a classic needlestick injury. The patient is a 28-year-old intravenous drug user. No baseline serology is available. Your resident says, 'Wash it with soap, don't worry, these things happen.' You know they are wrong, but you don't know exactly what to do next or how quickly you need to act. This module ensures that when this moment arrives — and statistically it will — you know precisely what to do within the next 30 minutes, the next 2 hours, and the next 28 days.
WHY THIS MATTERS
Health professionals in India and globally suffer disproportionate rates of occupational illness — yet this is systemically under-recognised and under-reported. Globally, the WHO estimates that healthcare workers account for 37% of lower back injuries, 53% of needlestick injuries, and are 2–5 times more likely to develop occupational tuberculosis than the general population. Burnout among medical students and residents — increasingly recognised as an occupational disorder — affects 40–60% of trainees in studies from Indian medical colleges. CM11.5 asks you to understand these disorders as a future clinician who will one day work in (and be responsible for the health of) a team of healthcare workers. Preventing occupational TB in your ward, managing a needlestick according to protocol, and recognising burnout in yourself and colleagues are the direct applications of this competency.
RECALL
Recall from your Microbiology postings: the modes of transmission of HIV (bloodborne; sexual; vertical), hepatitis B (bloodborne, sexual, vertical — more stable on surfaces than HIV), and hepatitis C (primarily bloodborne). Recall from Pharmacology: antiretrovirals — the nucleoside reverse transcriptase inhibitors (NRTIs), non-nucleoside reverse transcriptase inhibitors (NNRTIs), and integrase strand transfer inhibitors (INSTIs) — used in HIV treatment. Recall from Preventive Medicine: the concept of standard precautions (formerly 'universal precautions') as the baseline infection control strategy. From Anatomy: the musculoskeletal anatomy of the lumbar spine, shoulder, and wrist — the sites most commonly affected by ergonomic hazards in health workers.
Health Workers as an Occupationally Exposed Population — Burden and Recognition
Healthcare workers (HCWs) — a group that includes doctors, nurses, paramedics, laboratory personnel, radiographers, anaesthesiologists, cleaners, laundry workers, and waste handlers in health facilities — constitute a distinct and highly exposed occupational population. Globally, WHO estimates there are approximately 43 million healthcare workers worldwide (2022 data), of whom a significant proportion work in low-resource settings with minimal occupational health protection.
The occupational burden in healthcare is substantial across multiple hazard categories:
- Approximately 2 million percutaneous injuries (needlestick and sharps injuries) occur among HCWs annually worldwide, exposing workers to bloodborne pathogens
- Healthcare workers account for roughly 37% of occupational lower back injuries globally — nurses and nursing aides have among the highest rates of musculoskeletal disorders of any occupational group
- Occupational tuberculosis: HCWs in high-TB-burden settings (India, South Africa, sub-Saharan Africa) have a 2–5× higher risk of TB than the general population; certain specialties (ENT, pulmonology, emergency medicine) carry even higher risk
- Burnout: Multiple Indian studies report 40–60% prevalence among medical residents and interns
Despite this burden, health professional occupational disorders are systematically under-recognised for several reasons: (1) medical culture of stoicism ('everyone gets needlesticks, it's part of the job'); (2) fear of stigma, particularly for bloodborne pathogen exposures; (3) poor reporting systems in many Indian hospitals; (4) absence of designated occupational health services for hospital staff in most district and sub-district hospitals. The result is that HCWs often manage their own occupational injuries — poorly, late, or not at all.
Recognising healthcare workers as a specific at-risk occupational group — with their own hazard profile, exposure mapping, and prevention needs — is the starting point for this SDL. The same preventive framework (hazard identification → exposure assessment → hierarchy of controls → surveillance) that applies to factory workers applies to healthcare workers; what differs is the specific hazard profile.
Biological Hazards in Healthcare — Bloodborne Pathogens and Airborne Infections
Biological hazards are the most dramatically recognised occupational risk for healthcare workers, though not necessarily the most prevalent. They divide into two main categories: bloodborne pathogens (transmitted via percutaneous or mucosal exposure to blood/body fluids) and airborne/droplet infections (transmitted via respiratory route).
Bloodborne Pathogens — Needlestick and Sharps Injuries:
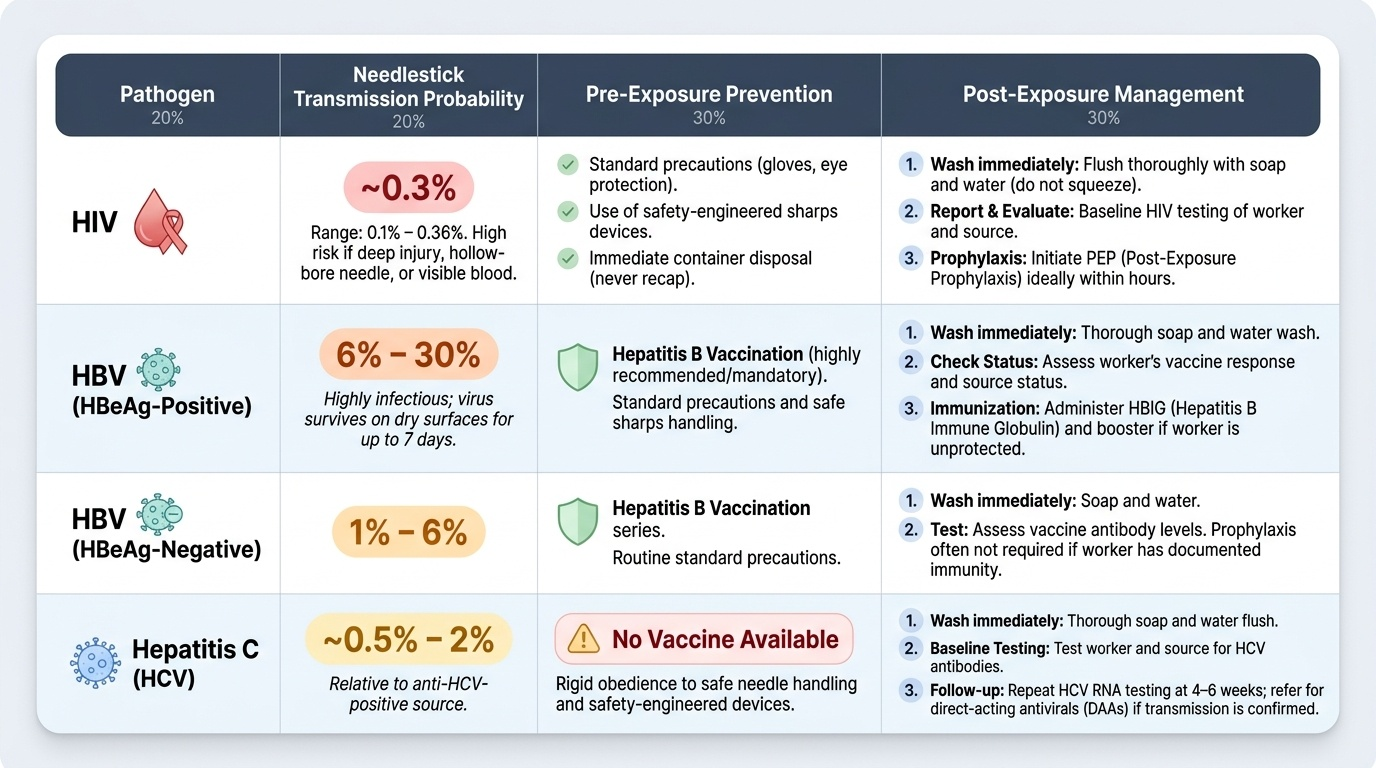
A needlestick injury (NSI) is the classic exposure event — but sharps injuries also occur from scalpels, broken glass, and IV cannulas. The transmission risk per percutaneous exposure from an infected source varies significantly by pathogen:
- HIV: approximately 0.3% (range 0.1–0.36%) per needlestick from an HIV-positive source. Risk is higher with deep injuries, hollow-bore needles, visible blood in the needle, and when the source has high viral load (end-stage AIDS or acute seroconversion).
- Hepatitis B virus (HBV): 6–30% per needlestick from an HBeAg-positive source (highly infectious); 1–6% from HBeAg-negative source. HBV is far more transmissible than HIV per event — it survives on surfaces for up to 7 days.
- Hepatitis C virus (HCV): approximately 0.5–2% per needlestick from an anti-HCV-positive source. No vaccine available (2024).
These probabilities reinforce why vaccination (for HBV) and post-exposure protocols (for all three) are mandatory, not optional, in healthcare.
Standard Precautions — The First Line of Prevention:
Standard precautions (the evolved form of universal precautions) apply to ALL patients regardless of known or suspected infection status. They include:
- Hand hygiene: the single most effective infection control measure (5 WHO moments of hand hygiene)
- Gloves: for any anticipated contact with blood, body fluids, mucous membranes, or non-intact skin
- Masks, eye protection, face shields: for procedures likely to generate splashes or sprays of blood
- Gowns/aprons: for procedures with exposure risk
- Safe needle and sharps handling: never recap needles two-handed; use safety-engineered devices; immediate disposal in puncture-resistant sharps containers
- Respiratory hygiene and cough etiquette
Post-Exposure Management — Immediate Steps:
When a needlestick or mucosal exposure occurs:
1. Immediately: wash the wound thoroughly with soap and water (do not squeeze or suck); for mucosal splash: irrigate eye/mucosa with copious water
2. Do not: apply bleach, disinfectants directly to the wound, or squeeze the site (increases HIV transmission risk)
3. Assess the exposure: hollow-bore needle? depth of penetration? source patient status?
4. Report immediately to the designated infection control officer or medical superintendent
Post-Exposure Prophylaxis (PEP) for HIV:
HIV PEP is a 28-day course of antiretroviral therapy. The key constraint is time: PEP must be initiated within 72 hours, with every hour of delay reducing efficacy. Initiation within 1–2 hours is optimal. Standard PEP regimen (WHO 2013 guidelines, updated 2016): tenofovir disoproxil fumarate (TDF) + emtricitabine (FTC) ± a third agent (dolutegravir preferred; lopinavir/ritonavir or atazanavir/ritonavir as alternatives). PEP is recommended for: (a) high-risk exposures from HIV-positive or unknown-status sources in high-prevalence settings; (b) not recommended for low-risk exposures (e.g., splash to intact skin from HIV-negative source).
Post-Exposure Management for HBV:
- HCW not previously vaccinated OR non-responder (anti-HBs <10 mIU/mL): receive hepatitis B immunoglobulin (HBIG) + initiate HBV vaccine series immediately
- HCW vaccinated with confirmed immunity (anti-HBs ≥10 mIU/mL): no additional action required
- HCW vaccinated but immunity unknown: test anti-HBs; if ≥10 mIU/mL = protected; if <10 = give HBIG + booster dose
Post-Exposure Management for HCV:
No post-exposure prophylaxis available. Baseline HCV testing at exposure + follow-up testing at 6 weeks and 12 weeks. If HCV seroconversion detected: refer to hepatologist; direct-acting antivirals (DAAs) achieve >95% cure rates for acute HCV, so early detection enables early treatment.
Occupational Tuberculosis:
Healthcare workers in India face a substantially elevated risk of occupational TB because: (1) India has the highest absolute TB burden globally; (2) many hospitals lack adequate ventilation and negative-pressure isolation; (3) procedures such as sputum induction, bronchoscopy, intubation, and ENT surgery generate high-risk aerosols. At-risk specialties: pulmonology, ENT, emergency medicine, microbiology lab personnel, infection control nurses.
Prevention: N95 respirators (not surgical masks) for all aerosol-generating procedures; upper-room UVGI (ultraviolet germicidal irradiation) in high-risk areas; annual tuberculin skin test (TST/Mantoux) or IGRA screening for all HCWs; isoniazid preventive therapy (IPT) for latent TB in HCWs in endemic settings.
Other biological hazards: COVID-19 (healthcare worker deaths were significant globally 2020–2021; aerosol precautions in addition to droplets); MRSA and C. diff (contact precautions); rabies (veterinarians, laboratory workers handling specimens); viral haemorrhagic fevers (Ebola, Crimean-Congo — full PPE, airborne isolation).
Provided image
SELF-CHECK
An intern sustains a needlestick from a hollow-bore needle used on an HIV-positive patient with a high viral load. She is vaccinated against hepatitis B (anti-HBs = 45 mIU/mL) and not on HIV PEP. It is currently 3 PM. She presents to the casualty at 11 PM the same day. Which statement is MOST accurate regarding HIV PEP?
A. PEP can no longer be offered as more than 6 hours have passed
B. PEP should be started immediately — 8 hours is within the 72-hour window; begin TDF+FTC ± dolutegravir
C. PEP is contraindicated in vaccinated healthcare workers
D. PEP is only for mucosal (splash) exposures, not needlestick injuries
Reveal Answer
Answer: B. PEP should be started immediately — 8 hours is within the 72-hour window; begin TDF+FTC ± dolutegravir
HIV PEP must be started within 72 hours of exposure — 8 hours is well within the window, though earlier initiation (within 1–2 hours) is ideal. The standard PEP regimen is TDF + FTC (as a fixed-dose combination, e.g. Truvada) with dolutegravir as the preferred third agent (WHO 2016 update). PEP is indicated for high-risk exposures (hollow-bore needle, HIV-positive source with high viral load) regardless of HBV vaccination status. Her HBV immunity (anti-HBs 45 mIU/mL, well above the ≥10 mIU/mL threshold) is protective and no HBV-related action is needed — but this does not affect the HIV PEP decision.
Chemical, Physical, and Ergonomic Hazards in Healthcare Settings
Beyond biological hazards, healthcare workers face a range of chemical, physical, and ergonomic hazards that are less acutely dramatic but cumulatively responsible for a substantial burden of chronic occupational morbidity.
Chemical Hazards:
Anaesthetic gas exposure affects operating theatre staff, anaesthesiologists, surgeons, and scrub nurses who work in theatres without adequate scavenging systems. The principal agents of concern are nitrous oxide (N₂O) and halogenated volatile agents (halothane, isoflurane, desflurane, sevoflurane). Nitrous oxide is particularly hazardous: it irreversibly inactivates methionine synthase, an enzyme essential for vitamin B₁₂ metabolism and DNA synthesis. Chronic occupational exposure is associated with megaloblastic changes, reproductive toxicity (increased spontaneous abortion risk in theatre nurses and female anaesthesiologists), and peripheral neuropathy. The NIOSH action level for N₂O in operating theatres is 25 ppm time-weighted average. Prevention requires: modern scavenging systems that capture exhaled anaesthetic gas, regular air monitoring, and minimising theatre time in poorly scavenged areas.
Antineoplastic (cytotoxic) drug exposure affects pharmacy staff, oncology nurses, and occasionally physicians handling chemotherapy agents. Cytotoxic drugs are carcinogenic, mutagenic, and teratogenic — the same properties that make them effective against cancer make them dangerous to health workers. Routes of exposure include inhalation of aerosolised drug during preparation, skin absorption during administration, and ingestion via contaminated surfaces. Prevention: biological safety cabinets (class II type B) for preparation; closed-system drug transfer devices; chemotherapy-grade gloves and protective gowns; dedicated staff training.
Latex allergy affects HCWs who use latex gloves frequently. Two immunological forms: Type I (IgE-mediated) — immediate hypersensitivity, can cause urticaria, angioedema, bronchospasm, and anaphylaxis; most dangerous. Type IV (T-cell mediated) — delayed-type hypersensitivity, causes contact dermatitis (itching, redness, vesicles on the hands after glove removal). Sensitisation risk correlates with frequency of use. Prevention: substitution with latex-free nitrile gloves (elimination of the causal agent — highest tier of control hierarchy).
Glutaraldehyde and disinfectants: used for high-level disinfection of endoscopes; glutaraldehyde is a respiratory sensitiser and skin irritant. Engineering control: enclosed automated disinfection systems; PPE (nitrile gloves, face shield, chemical-resistant apron).
Physical Hazards:
Ionising radiation is an occupational hazard for radiologists, cardiologists performing fluoroscopy-guided procedures, interventional radiologists, nuclear medicine physicians, and operating theatre staff using C-arm fluoroscopy. India's occupational dose limit for radiation workers is 20 mSv per year (average over 5 years, with no single year exceeding 50 mSv) — set by the Atomic Energy Regulatory Board (AERB). Prevention: maximum distance from the X-ray source; lead aprons, thyroid shields, and lead glasses for fluoroscopy workers; thermoluminescent dosimeter (TLD) badges for dose monitoring; limiting cumulative exposures through rotation.
Ergonomic Hazards — Musculoskeletal Disorders (MSDs) in Health Workers:
MSDs are the most prevalent occupational disorder in nursing, surgery, and dentistry. Major patterns:
- Low back pain and lumbar disc disease: nurses and ward attendants involved in manual patient handling (lifting, repositioning, transferring), and surgeons who stand for prolonged periods
- Shoulder pathology (rotator cuff disorders): anaesthesiologists (sustained shoulder abduction during intubation), surgeons using laparoscopic ports at non-ergonomic heights
- Carpal tunnel syndrome: surgeons performing laparoscopic/robotic procedures with repetitive wrist movements; laboratory personnel using pipettes
- Cervical spondylosis: dentists (sustained neck flexion), microsurgeons, pathologists
- Knee injuries: operating theatre staff standing on hard floors for extended procedures
Prevention: patient handling equipment (mechanical hoists, slide sheets, transfer boards) for nurses; ergonomically designed operating tables at appropriate heights; anti-fatigue mats; brief stretching breaks between surgical cases; regular ergonomic assessment of workstations (RULA for upper limbs).
SELF-CHECK
An anaesthesiologist working in an old theatre without gas scavenging reports three spontaneous abortions among the female theatre nurses and herself over two years. The most likely occupational chemical responsible is:
A. Isoflurane — causes endocrine disruption directly
B. Nitrous oxide — inactivates methionine synthase, causing reproductive toxicity
C. Propofol — absorbed through skin contact during drug preparation
D. Ketamine — CNS depressant causing foetal growth restriction
Reveal Answer
Answer: B. Nitrous oxide — inactivates methionine synthase, causing reproductive toxicity
Nitrous oxide irreversibly inactivates methionine synthase — an enzyme critical for DNA synthesis and normal cell division. Chronic occupational exposure of theatre staff to nitrous oxide (in theatres without scavenging) is associated with increased rates of spontaneous abortion and reproductive toxicity. This is the classic occupational hazard of unscavenged anaesthetic theatre environments. The NIOSH action level is 25 ppm. Isoflurane and halogenated agents are also volatile anaesthetic hazards, but the reproductive mechanism of nitrous oxide via methionine synthase is the most well-established and directly relevant.