Page 9 of 15
CM11.5 | CM11.5 | Health Professional Occupational Disorders — SDL Guide (Part 2)
Prevention and Control — Occupational Health Programmes for Health Workers
Prevention of occupational disorders in healthcare settings follows the same hierarchy of controls used in industrial settings, applied to the specific hazard landscape of hospitals and clinics.
Universal application of standard precautions — the institutional bedrock of biological hazard control in healthcare. The institution's infection control committee owns this programme: auditing glove use, hand hygiene compliance (with the WHO 5 Moments framework), sharps disposal compliance, and PPE availability. Standard precautions are equivalent to engineering controls in the industrial hierarchy — they are system-level, not individual-behaviour-dependent when implemented institutionally.
Safety-engineered sharps devices: safer needle systems with retractable tips, self-sheathing needles, and needleless IV systems reduce needlestick injuries by 60–80% in settings where they have been implemented. These devices are an engineering control within the hierarchy and are significantly more effective than PPE (gloves alone) for NSI prevention.
Vaccination as pre-exposure prophylaxis: All healthcare workers must receive:
- Hepatitis B vaccine (3-dose, 0-1-6 months schedule): mandatory for all HCWs in India before clinical posting; confirm immunity with anti-HBs at 4–8 weeks post-series. Non-responders: additional 3 doses + retest; if still non-responsive = HBIG-dependent protection only.
- Influenza vaccine: annual; reduces healthcare worker absenteeism and patient-to-worker transmission
- COVID-19 vaccine: institutional vaccination programme
- Typhoid, Hepatitis A: for food-handlers in hospital canteens; laboratory workers handling enteric specimens
Exposure response protocols — formalised, accessible, with designated officers:
- Written NSI/exposure protocol posted at every nursing station and OT
- Designated duty medical officer who can initiate HIV PEP at any hour
- Baseline serology (HBsAg, anti-HCV, HIV antibody) for both source and exposed worker, drawn within 2 hours of exposure
- Registry of all occupational exposures with follow-up tracking at 6 weeks, 12 weeks, and 6 months
Radiation safety programme: TLD (thermoluminescent dosimeter) badge monitoring for all radiation workers; quarterly dose review; dose limits per AERB (20 mSv/year average); lead-shielded procedure rooms; distance and time as primary controls (inverse-square law for radiation intensity).
Theatre anaesthetic gas monitoring: regular ambient N₂O and volatile agent measurements; maintain below NIOSH action levels; document scavenging system function.
Pre-employment and periodic health surveillance for HCWs:
- Pre-employment: HBV serostatus and vaccination if not immune; TB screening (TST/IGRA); baseline chest X-ray for TB-exposed workers; general health assessment
- Periodic: Annual TB screening for high-risk departments; annual TST or IGRA for all clinical staff in high-TB-burden settings; audiometry for ICU/NICU staff (alarm noise); radiation dosimetry review
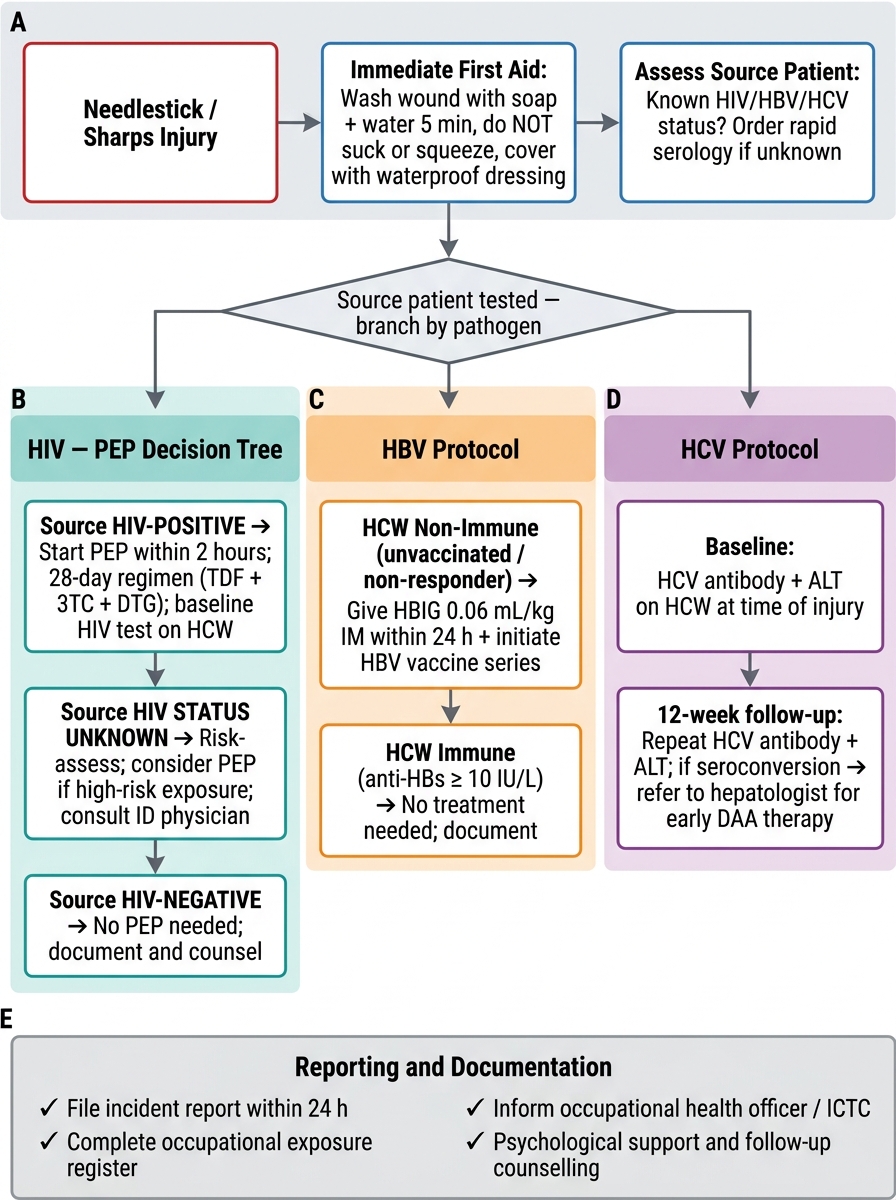
Post-Exposure Protocol After Needlestick / Sharps Injury
Psychosocial Hazards and Burnout — Evaluation and Monitoring
Psychosocial hazards in healthcare represent an increasingly recognised occupational health crisis. Unlike chemical or biological hazards, psychosocial hazards are diffuse, normalised within medical culture, and resistant to simple engineering solutions. They cause measurable harm — in the form of burnout, moral injury, compassion fatigue, depression, substance misuse, and suicidality — at rates significantly higher than the general population.
Burnout is a work-specific syndrome defined by the Maslach Burnout Inventory (MBI) across three dimensions:
1. Emotional exhaustion: feeling depleted of emotional resources; the 'I have nothing left to give' dimension
2. Depersonalisation (cynicism): detached, callous, or impersonal attitude toward patients or colleagues; a psychological distancing response to exhaustion
3. Reduced personal accomplishment: a sense of inefficacy and lack of achievement, despite effort
In medical contexts, high emotional exhaustion + high depersonalisation + low personal accomplishment = classic burnout profile. Indian studies report burnout rates of 40–60% among residents and interns, with the highest rates in high-workload departments (emergency medicine, surgery, ICU, oncology). Burnout is directly associated with medical errors, suboptimal patient care, increased substance use, and suicidal ideation.
Moral injury — distinct from burnout — refers to the harm caused when a healthcare worker is required to act (or witnesses action) in ways that violate their moral code. Examples: being unable to provide adequate care due to resource constraints; following institutional directives that compromise patient welfare; witnessing corruption in healthcare. Moral injury is more corrosive than workload-driven burnout because it undermines the foundational values that drew the person to medicine.
Compassion fatigue is the secondary traumatic stress experienced by health workers repeatedly exposed to patient suffering — a gradual erosion of the capacity for empathy. It differs from burnout in having a trauma-related (rather than workload-related) aetiology.
Workplace violence against health workers is a specific psychosocial hazard with legislative relevance. Attacks on healthcare workers and destruction of hospital property — physically dangerous and psychologically traumatic — are an occupational risk in India, leading to the Protection of Healthcare Professionals Act provisions in multiple states. The institutional response must include: secure ward environments, security personnel, violence reporting mechanisms, and post-incident psychological support.
Monitoring and evaluation of psychosocial hazards:
- Maslach Burnout Inventory (MBI): validated 22-item tool measuring emotional exhaustion, depersonalisation, and personal accomplishment; used in research and institutional monitoring
- Copenhagen Burnout Inventory (CBI): 19-item tool; validated in healthcare
- Institutional measures: doctor-patient ratios, overtime hours, mandatory rest periods (Junior Doctors' Hours regulations in India are evolving), peer support programmes, counselling access
- Annual or biannual burnout screening for resident doctors and nurses in high-risk departments
- Post-incident debriefing (after patient deaths, violent incidents, or distressing events) as a mandatory institutional protocol
Psychosocial hazards are real occupational hazards: they satisfy the definition (the work environment causes the harm) and they are preventable with systematic institutional attention. Treating them as character weaknesses of individual workers — rather than as system-level occupational hazards — perpetuates the harm.
SELF-CHECK
A second-year resident in the oncology department reports feeling emotionally empty, describing her patients as 'just cases' rather than people, and doubting whether her work makes any difference. She has worked 80-hour weeks for 8 months. The Maslach Burnout Inventory domains best describing her presentation are:
A. Moral injury and compassion fatigue — distinct from burnout
B. High emotional exhaustion, high depersonalisation, and reduced personal accomplishment
C. High personal accomplishment but low depersonalisation — consistent with occupational stress, not burnout
D. Low emotional exhaustion only — burnout requires all three domains to be simultaneously abnormal
Reveal Answer
Answer: B. High emotional exhaustion, high depersonalisation, and reduced personal accomplishment
The classic triad of burnout on the Maslach Burnout Inventory is: (1) emotional exhaustion ('feeling emotionally empty'), (2) depersonalisation/cynicism ('patients as just cases'), and (3) reduced personal accomplishment ('doubting whether work makes any difference'). All three dimensions are present in this resident's description. Moral injury (values violation) and compassion fatigue (secondary trauma from patient suffering) are related but distinct constructs. Burnout does not require all three dimensions to be simultaneously extreme — any two with the third present creates the syndrome — but all three are clinically significant in this case.
Application — Managing a Needlestick Exposure and Designing a Health Worker Surveillance Programme
Applying the knowledge from this SDL requires both individual action (managing an exposure in real time) and institutional action (designing systems that prevent occupational illness). Both are expected competencies for a CM11.5 graduate.
Step-by-step Needlestick Management Protocol (applicable from intern year onward):
Immediate (0–30 minutes):
1. Wash wound with soap and water for ≥2 minutes (do not squeeze, suck, or apply bleach)
2. For mucosal splash: irrigate eyes or mouth with copious clean water for 15 minutes
3. Assess the exposure: hollow-bore vs solid needle? depth? visible blood in needle? source patient HIV/HBV/HCV status?
4. Report to the duty medical officer, charge nurse, or designated exposure officer immediately
Within 2 hours:
5. Draw baseline blood from the exposed worker: HIV ELISA, HBsAg, anti-HCV, LFTs, haematology
6. Assess source patient: request HIV, HBsAg, anti-HCV with consent; document source status
7. Initiate HIV PEP if indicated (high-risk exposure, HIV-positive or unknown source in high-prevalence setting): prescribe TDF + FTC + dolutegravir (preferred regimen) × 28 days
8. HBV management: check exposed worker's vaccination status and anti-HBs level; administer HBIG if non-immune
Days 1–28:
9. Ensure PEP adherence (28-day complete course); side effect monitoring (nausea, headache — common but manageable)
10. Formally document incident in the hospital exposure registry
Follow-up:
11. HIV testing at 6 weeks, 12 weeks, 6 months post-exposure
12. HCV: anti-HCV at 6 weeks and 12 weeks
13. HBV: if HBIG given, anti-HBs at 3 months to confirm seroconversion
14. Psychological support: needlestick is a traumatic event; brief counselling should be offered
Designing an Occupational Health Surveillance Programme for Hospital Staff:
A hospital occupational health service (equivalent to the factory health service described in CM11.6) should include:
New employee assessment:
- HBV vaccination status + anti-HBs titre; vaccinate if unprotected
- TB screening (TST/IGRA); chest X-ray for high-risk departments
- Document any pre-existing latex allergy, respiratory conditions, musculoskeletal disorders
- Departmental-specific baseline (e.g., baseline PFT for theatre staff in ICU near N₂O, baseline audiometry for NICU/PICU staff)
Ongoing surveillance:
- Annual TB screening for all clinical staff
- Annual influenza vaccination campaign
- Biannual ergonomic assessment of nursing stations, OT tables, ward lifting practices
- Quarterly review of radiation dosimetry reports (TLD badge data) for radiology/cardiology/OT staff
- Biannual burnout screening (MBI) for high-risk departments
- Monthly review of occupational exposure registry
Response mechanisms:
- NSI/exposure protocol, available 24 hours
- PEP starter pack accessible in casualty at all times
- Counselling service for burnout and post-incident distress
- Return-to-work programme for HCWs recovering from occupational illness
Reporting and notification:
- Occupational TB in healthcare workers: notifiable under State TB Control Programme
- Significant radiation overexposure: reportable to AERB
- HIV seroconversion post-occupational exposure: reportable to institution's ethics and medical committees
- Annual occupational health report to hospital management committee
The physician's dual role: As a healthcare worker you are both potentially exposed AND, in future roles, potentially responsible for the occupational health of the team around you. The CME11.5 competency asks you to understand both perspectives. When you are the junior doctor at a needlestick at 11 PM, you need the self-management protocol. When you are the medical superintendent at 45, you need the institutional programme design.
CLINICAL PEARL
The 72-Hour Window — and Why It Is Frequently Missed: Multiple studies from Indian medical institutions show that a significant proportion of healthcare workers who sustain high-risk needlestick injuries do not initiate HIV PEP — most commonly because they present after hours when PEP starter packs are not accessible, they are afraid of stigma from their peers, or they underestimate the risk ('the patient doesn't look like they have HIV'). The 72-hour window sounds generous, but in practice the barriers reduce it drastically. The institutional solution is a PEP starter pack (a 72-hour supply of TDF+FTC+dolutegravir) kept in the casualty department 24/7, so PEP can be initiated before the duty doctor has confirmed source serology. A 3-day starter pack is far cheaper than the psychological and financial consequences of occupational HIV seroconversion. Advocate for this in every hospital you work in.