Page 8 of 27
CM10.4 | CM10.4 | Child Survival and Safe Motherhood Interventions — SDL Guide
Learning Objectives
- Describe the reproductive, maternal, newborn and child health (RMCH) interventions for child survival and safe motherhood under the RMNCH+A framework
- Differentiate between the JSY and JSSK programme entitlements and describe the components of antenatal care, skilled birth attendance, essential newborn care, and child survival packages
INSTRUCTIONS
India has assembled one of the world's most comprehensive packages of maternal and child survival interventions — yet implementation gaps mean those packages are not reaching the women and children who need them most. This module maps every major RMCH intervention onto its target population, delivery platform, and measurable indicator, giving you the analytical framework to diagnose coverage gaps at the PHC level and the vocabulary to communicate with programme managers, district CMOs, and community health workers.
References
- Park's Textbook of Preventive and Social Medicine, 26th ed., Ch 11 (Reproductive and Child Health) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
Two women in the same district delivered in the same week. The first, a BPL card-holder in a rural area, received Rs 1,400 under JSY, delivered at a sub-centre with a trained SBA, got vitamin K for her baby, and had her high-risk newborn transferred to the SNCU at the district hospital within 4 hours. Three weeks later, both mother and baby are thriving. The second, also BPL, delivered at home because she did not know about JSY, her cord was cut with a kitchen knife, and she haemorrhaged at 36 hours postpartum. She died before reaching the PHC. Both women lived in the same village. What intervention gaps explain the different outcomes?
WHY THIS MATTERS
The RMNCH+A strategic framework is India's integrated response to maternal and child mortality — and you, as a community medicine practitioner and future PHC medical officer, are its ground-level implementation agent. Understanding every component — from the Rs 1,400 JSY cash transfer to the 12-step HBNC protocol to the four disease domains of RBSK — is not bureaucratic knowledge. It is the operational vocabulary you need to audit your facility's programme performance, identify which intervention is leaking coverage, and mobilise the right corrective response.
RECALL
Recall the five RMNCH mortality indicators and India's current values from the previous module: MMR 97 (SRS 2018-20), IMR 35.2, NMR 24.9, U5MR 41.9 (NFHS-5). Recall the 3-delays model: delay in recognition, delay in decision, delay in reaching care — RMCH interventions are designed to eliminate each delay. Also recall the high-risk screening categories (obstetric, medical, sociodemographic) that determine who needs a higher level of care, and the MUAC thresholds for malnutrition screening (SAM <11.5 cm, MAM 11.5-12.4 cm in children 6-59 months).
Burden of Preventable Maternal and Child Deaths
The compelling case for RMCH intervention investment rests on a fundamental epidemiological observation: the overwhelming majority of maternal and neonatal deaths are preventable with existing, low-cost interventions. Globally, approximately 75% of maternal deaths are attributable to five direct causes — haemorrhage, sepsis, hypertensive disorders, obstructed labour, and unsafe abortion — all of which are manageable with basic emergency obstetric care if the woman reaches a functioning facility in time. In India, the leading proximate cause of maternal death is haemorrhage (accounting for roughly 38% of maternal deaths in the RGI survey), followed by hypertensive disorders and sepsis. For neonatal deaths, 75% occur in the first week of life, with prematurity/LBW (35%), birth asphyxia (25%), and sepsis (25%) accounting for the vast majority — all preventable with essential newborn care at delivery and skilled management in the first 28 days. The 3-delays model provides the structural framework: an effective intervention package must address delay in recognition (community awareness and ASHA surveillance), delay in decision (financial and social barriers — addressed by JSY cash transfer and JSSkK entitlements), and delay in reaching care (transport systems, 108 ambulance network, delivery points at sub-centre level). Programme design that does not address all three delays will leave a structural gap that clinical excellence at the facility level cannot compensate for.
Determinants of Intervention Success and Failure
RMCH intervention coverage is shaped by both supply-side and demand-side determinants that a programme manager must assess separately. Supply-side determinants include: facility readiness (functional labour room, 24/7 delivery services, blood storage, skilled birth attendant on duty); drug availability (oxytocin, MgSO4 for eclampsia, antibiotics for sepsis, ORS and Zinc); equipment functionality (neonatal resuscitation bag, radiant warmer, pulse oximeter); and human resource presence and competency (SBA-trained ANM, MBBS doctor for CEmOC, specialist at district hospital). Supply-side gaps are diagnosed through HMIS data (facilities reporting zero deliveries despite being a declared delivery point) and facility assessments (LaQshya audit scores for labour rooms). Demand-side determinants include: awareness of entitlements (many eligible women do not know about JSY or JSSK), distance to the nearest delivery facility, transport access (the 108 ambulance system covers urban areas reliably but is sparse in tribal and hilly areas), perceived quality of care (past negative experiences with facility staff discourage future visits), and cultural factors (home delivery preference in some communities, elder-family authority over delivery decisions). Gender-related determinants are cross-cutting: a woman who cannot independently decide to go to a facility — who requires permission from her husband or mother-in-law — faces a systematic delay regardless of supply-side readiness. Interventions that only strengthen facilities without addressing these demand barriers will plateau at modest coverage gains.
SELF-CHECK
Which of the following is a JSSK entitlement but NOT a JSY entitlement?
A. Cash incentive of Rs 1,400 for rural BPL mothers
B. Free institutional delivery including drugs, diagnostics, and diet
C. Additional cash incentive for ASHAs who escort women to delivery
D. Increased incentive for deliveries in high-priority states
Reveal Answer
Answer: B. Free institutional delivery including drugs, diagnostics, and diet
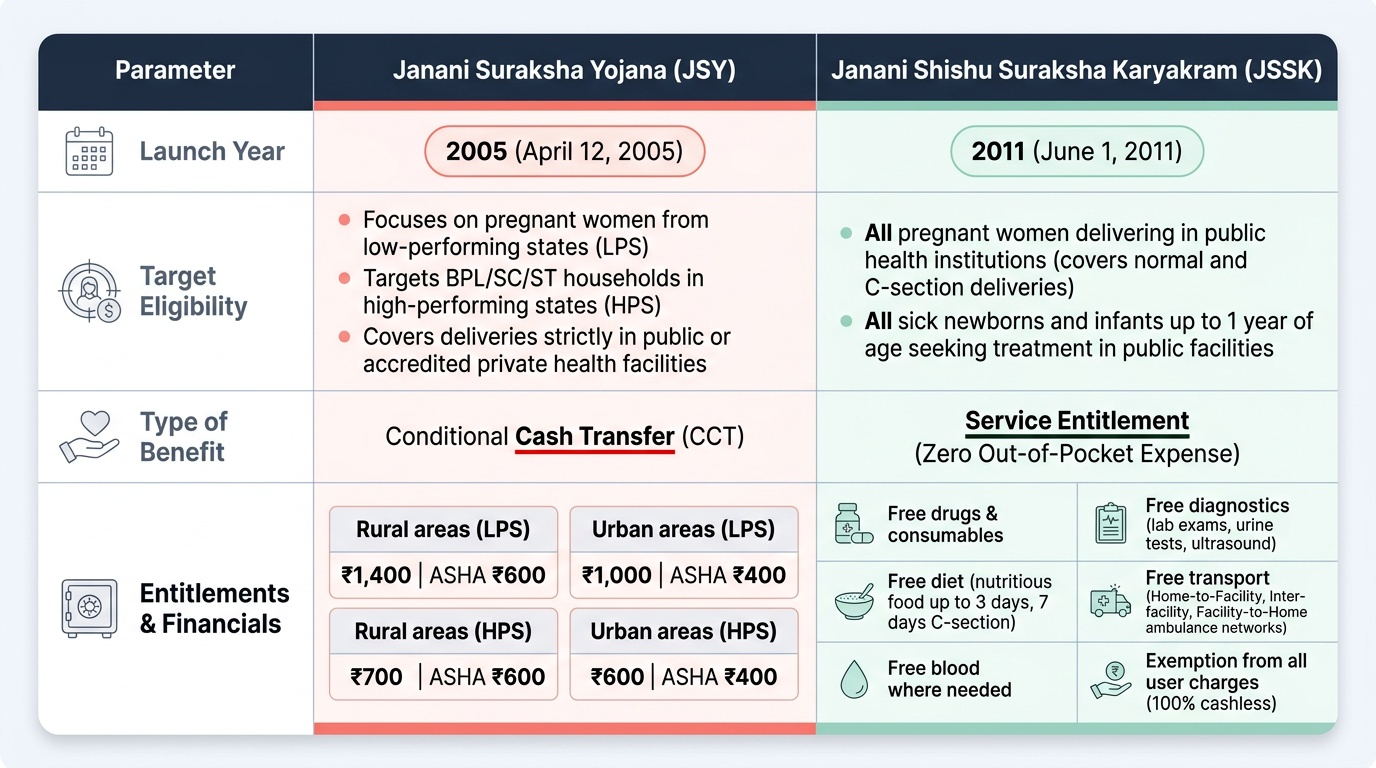
JSSK (Janani Shishu Suraksha Karyakram, 2011) provides free, entitlement-based services: free delivery, free drugs and consumables, free diagnostics, free diet during stay, and free transport — all without any cash changing hands. JSY (Janani Suraksha Yojana, 2005) is a cash transfer scheme: it gives cash incentives to BPL mothers (Rs 1,400 rural, Rs 1,000 urban) and to ASHAs who escort women. The two programmes are complementary: JSY reduces the financial barrier to going to a facility; JSSK ensures there are no charges once she arrives.
Maternal Interventions: ANC, Skilled Birth Attendance, EmOC
The safe motherhood intervention package operates across four time points: antenatal, intrapartum, postpartum, and between pregnancies. Antenatal care (ANC): the GOI standard for full ANC includes at minimum 4 visits (first before 12 weeks, second at 14-26 weeks, third at 28-34 weeks, fourth at 36 weeks onwards), registration and issuing of the MCP card, at least 180 iron-folic acid tablets, 2 tetanus toxoid injections, measurement of weight-height-BP-haemoglobin at each visit, one ultrasound before 20 weeks, and high-risk screening. NFHS-5 reports that 58.1% of Indian women received ≥4 ANC visits. The Pradhan Mantri Surakshit Matritva Abhiyan (PMSMA) supplements routine ANC with a comprehensive package on the 9th of every month at government facilities — with specialist examination available. Skilled Birth Attendance (SBA): a skilled birth attendant is defined as a health professional (midwife, nurse, or doctor) who can provide basic maternal and neonatal care and manage or refer complications. India's NFHS-5 institutional delivery rate is 88.6%, a substantial rise from 38.7% in NFHS-3 — largely attributable to JSY. Emergency Obstetric Care (EmOC): Basic EmOC (BEmOC) at CHC level provides: administration of parenteral uterotonics (oxytocin), antibiotics, and anticonvulsants (MgSO4); manual removal of placenta; assisted vaginal delivery (vacuum/forceps); and resuscitation of the newborn. Comprehensive EmOC (CEmOC) at district hospital adds: caesarean section and blood transfusion. The WHO standard is one CEmOC facility per 150,000 population and one BEmOC per 30,000. Postpartum care (PNC): the first PNC contact occurs within 48 hours of delivery (whether home or facility) — the ANM assesses uterine involution, lochia, breastfeeding establishment, and puerperal fever. Two additional PNC contacts occur at day 3-7 and at 42 days; the 42-day visit incorporates postnatal counselling on contraception, IUD insertion if desired, and review of the immunisation record.
Provided image