Page 9 of 27
CM10.4 | CM10.4 | Child Survival and Safe Motherhood Interventions — SDL Guide (Part 2)
Newborn Interventions: ENC, HBNC, SNCU
Newborn survival interventions follow a tiered continuum from the delivery room to the district hospital. Essential Newborn Care (ENC) — the package to be delivered at every birth, regardless of setting — comprises: (1) immediate warmth through skin-to-skin care with the mother (prevents hypothermia, the primary killer of small newborns); (2) early breastfeeding initiation within 1 hour (reduces all-cause neonatal mortality by 19-22%); (3) dry cord care — keeping the cord clean and dry, applying nothing to the stump (application of chlorhexidine 7.1% gel to the cord is recommended where neonatal tetanus risk is very high, as per WHO); (4) vitamin K injection (1 mg IM for all newborns, preventing vitamin K deficiency bleeding/haemorrhagic disease of the newborn); and (5) eye prophylaxis against neonatal conjunctivitis (tetracycline 1% eye ointment or 2.5% povidone iodine drops). Home-Based Newborn Care (HBNC): the ASHA makes 6 scheduled home visits — day 1 (within 24 hours of home delivery), days 3, 7, 14, 21, and 28 — using a structured checklist to assess feeding, temperature, jaundice, breathing, skin condition, and danger signs (not feeding, convulsions, fast breathing, severe jaundice, hypothermia, skin pustules). High-risk newborns (LBW, preterm, birth asphyxia) receive 7 visits including day 42. Newborn Stabilisation Units (NBSUs) at CHC level provide incubation, phototherapy (for jaundice), and oxygen therapy — for newborns who need facility support but not intensive care. Special Newborn Care Units (SNCUs) at district hospitals handle sick newborns requiring IV fluids, parenteral antibiotics, continuous monitoring, and management of birth asphyxia sequelae — they bridge the gap between level-2 and tertiary NICU care.
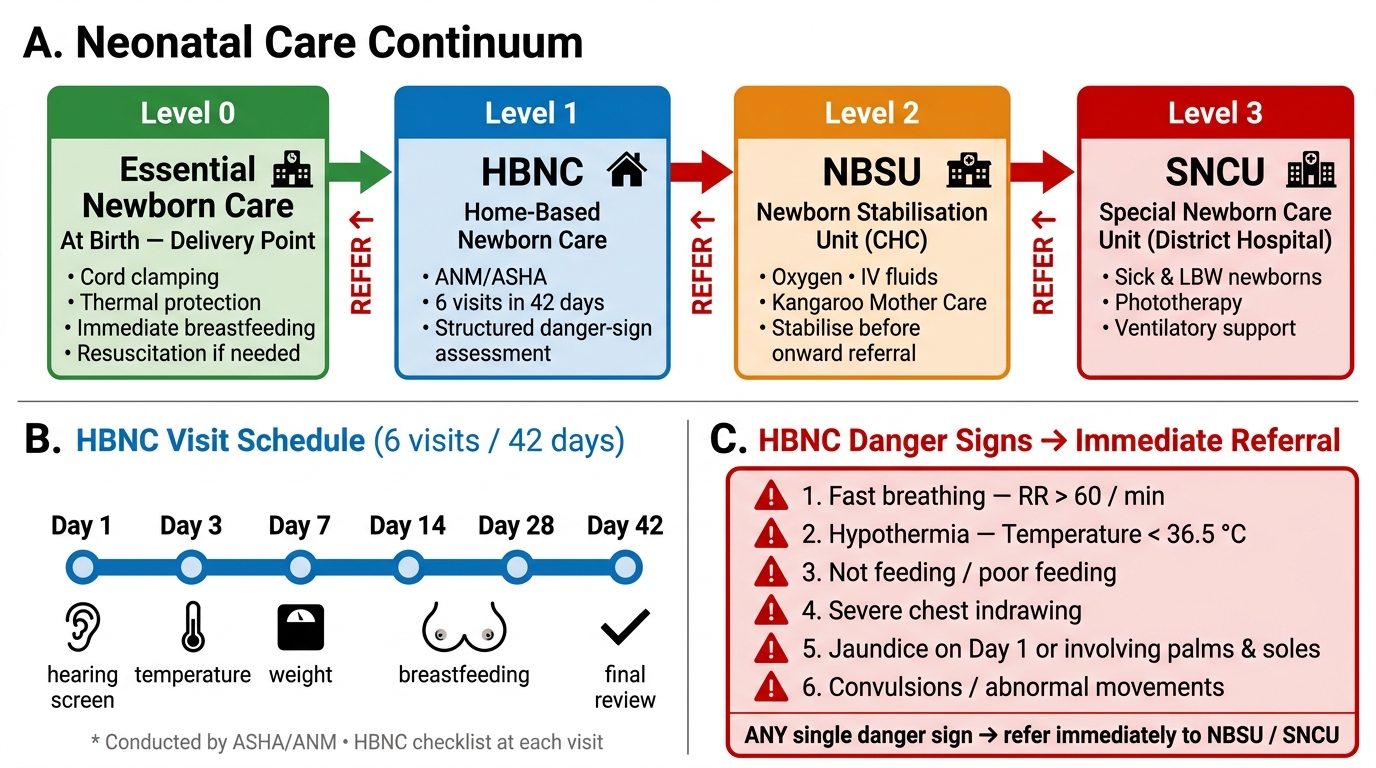
Neonatal Care Continuum: Levels 0–3 with HBNC Visit Schedule and Referral Triggers
SELF-CHECK
An ANM visits a 3-day-old home-born infant and finds respiratory rate of 72/minute, temperature of 36.1°C, and the baby is not feeding. Which of the following is the correct management under the HBNC protocol?
A. Reassure the mother; fast breathing is normal in newborns
B. Identify as a danger sign, provide skin-to-skin care for warmth, and refer immediately to NBSU or SNCU
C. Administer oral amoxicillin from the ASHA drug kit and review in 48 hours
D. Record in the HBNC register and escalate to the PHC Medical Officer at the next morning OPD
Reveal Answer
Answer: B. Identify as a danger sign, provide skin-to-skin care for warmth, and refer immediately to NBSU or SNCU
This infant has three HBNC danger signs simultaneously: respiratory rate >60/minute (fast breathing — normal newborn RR is 30-60), temperature borderline low at 36.1°C (hypothermia defined as <36.5°C), and not feeding. Any single danger sign on the HBNC checklist mandates immediate referral, not watchful waiting. The correct action is: (1) wrap the baby skin-to-skin with the mother (Kangaroo Mother Care) to correct hypothermia during transport, and (2) refer immediately to the NBSU at the CHC or SNCU at the district hospital. Option C is wrong — the ASHA drug kit does not contain antibiotics for infants, and home oral treatment for a neonate with multiple danger signs is unsafe.
Child Survival Interventions: IYCF, Vitamin A, IMCI/IMNCI, RBSK
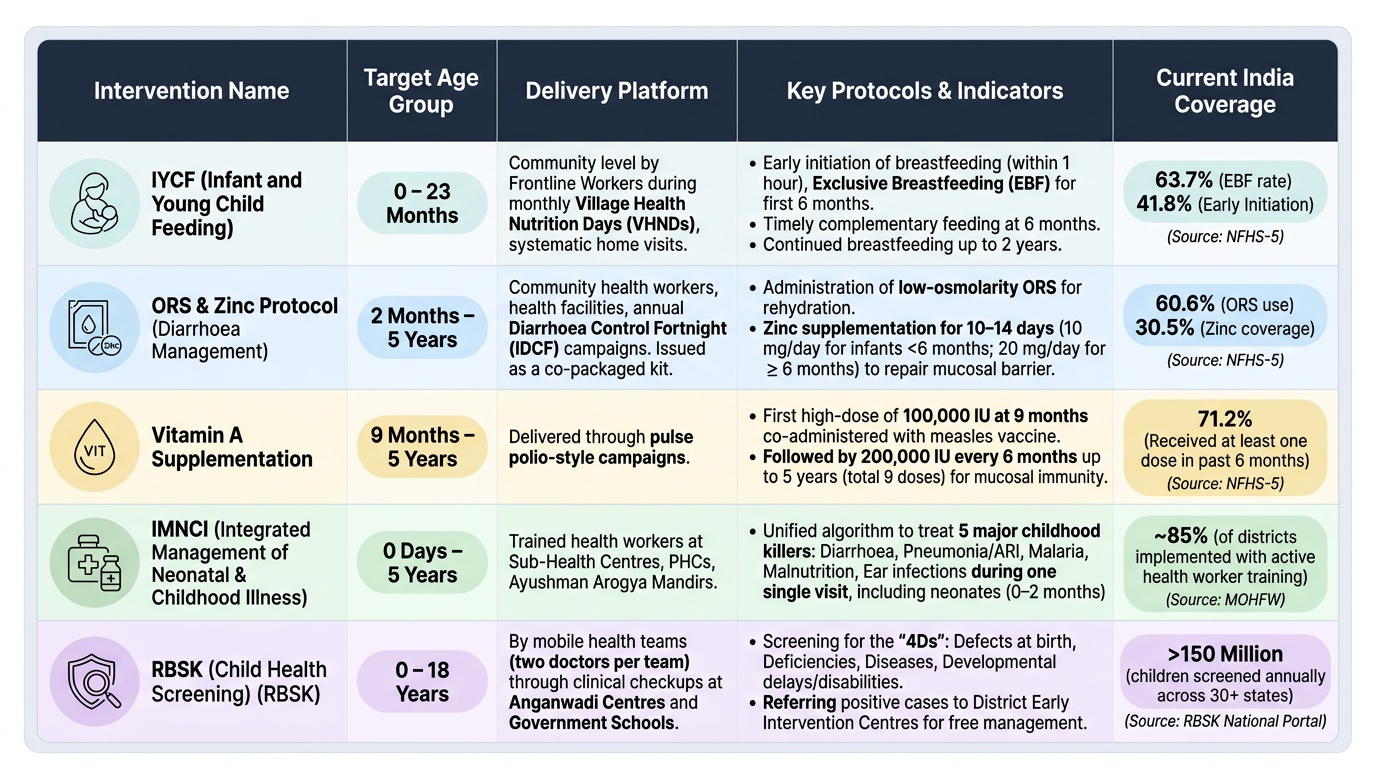
Child survival interventions extend beyond the neonatal period to address the major killers of children aged 1 month to 5 years: diarrhoea, pneumonia, malaria, malnutrition, and vaccine-preventable diseases. ORS and Zinc protocol for diarrhoea: WHO and UNICEF recommend low-osmolarity ORS (sodium 75 mEq/L, glucose 75 mmol/L) for rehydration and 10-14 days of zinc supplementation (10 mg/day for infants <6 months; 20 mg/day for children ≥6 months). The zinc shortens diarrhoeal duration, reduces stool output, and — importantly — reduces diarrhoeal episodes in the subsequent 2-3 months because it corrects the mucosal barrier zinc deficit. India's Diarrhoea Control Fortnight campaigns promote ORS-Zinc as a package; the two must not be separated. Vitamin A supplementation: a single high-dose vitamin A supplement every 6 months, beginning at 9 months, reduces all-cause under-5 mortality by 12-24% by restoring mucosal immunity and anti-infective defences. The schedule: 100,000 IU at 9 months (with measles vaccine), then 200,000 IU every 6 months up to 5 years. Delivered through pulse polio-style campaigns. Integrated Management of Childhood Illness (IMCI) / Integrated Management of Neonatal and Childhood Illness (IMNCI): a case-management protocol that trains health workers to simultaneously assess, classify, and treat the five major childhood illness categories (diarrhoea, respiratory infection, malaria, malnutrition, ear infection) in a single integrated visit — reducing fragmented care. IMNCI extends this to neonates (0-2 months). Rashtriya Bal Swasthya Karyakram (RBSK): the GOI child health screening programme targeting children aged 0-18 years for four disease domains: 4Ds — Defects at birth, Deficiencies (nutritional and micronutrient), Diseases (including anaemia, dental caries, skin conditions), and Developmental delays/disabilities. Mobile health teams (two doctors per team) screen children at Anganwadi centres and schools; positives are referred to District Early Intervention Centres (DEICs) for diagnostic workup and management.
Provided image
Monitoring RMCH Intervention Coverage
Monitoring whether interventions are reaching the intended population requires a multi-layer surveillance architecture. The Mother and Child Tracking System (MCTS) — now integrated into the Reproductive and Child Health portal (RCH portal) — is a name-based tracking system that registers every pregnant woman by name, assigns a unique ID, and tracks her ANC visits, delivery, postnatal contacts, and infant immunisation schedule. A pregnant woman who misses her scheduled 28-week visit automatically generates an alert for the ASHA or ANM to make a home visit — converting the system from passive recording to active follow-up. The HMIS aggregates facility-wise data monthly on: institutional delivery rate (target 90%+ by NRHM), full ANC coverage, first-trimester ANC registration, SNCU admission and survival rates, and HBNC visit completion rates. The LaQshya programme (Labour Room Quality Improvement Initiative, 2017) uses a 100-point quality dashboard for labour rooms: it measures direct indicators such as use of partograph, administration of oxytocin with correct timing, buddy birth companion allowance, and delayed cord clamping (30-60 seconds after birth). The Maternal Death Surveillance and Response (MDSR) system mandates community-level investigation of every maternal death within 24 hours — the investigation identifies the three-delay category and the root cause, which are then fed into programme correction. National Family Health Survey (NFHS) rounds (every 4-5 years) provide population-level coverage data — institutional delivery 88.6% (NFHS-5), full ANC 58.1%, early initiation of breastfeeding 41.8% — that are used to evaluate long-term trends and district-level equity gaps.
CLINICAL PEARL
The single most cost-effective neonatal intervention is the 10-minute neonatal resuscitation protocol: a newborn who does not breathe spontaneously within 60 seconds of birth needs positive pressure ventilation via bag-and-mask at 30-60 breaths/minute. The skills required — positioning the airway, achieving a seal, recognising effective ventilation by chest rise and improving heart rate — can be taught to an ANM in a one-day training. Yet failure to resuscitate birth-asphyxiated newborns accounts for 25% of all neonatal deaths in India. Every delivery point, including sub-centres, should have a functioning neonatal bag and mask and an ANM trained to use it.