Page 20 of 27
CM10.8-10 | CM10.8-10 | Adolescent Health, Gender Issues and RMCH Services — SDL Guide
Learning Objectives
- Describe the physiology, clinical management, and principles of adolescent health including the ARSH programme
- Describe and discuss gender issues and women empowerment in the context of RMNCH
- Manage healthcare services for reproductive and child care under supervision at the PHC level
INSTRUCTIONS
India has the world's largest adolescent population — 253 million people aged 10-19 years, representing one-fifth of the country's total population. Their health determines India's demographic trajectory for the next 40 years. Yet 59.1% of adolescent girls in India are anaemic, 23.3% of women marry before age 18, and gender-based violence remains vastly underreported. As a PHC medical officer you will run ARSH clinics, supervise WIFS distribution, manage RKSK peer educator programmes, and be the first institutional responder to cases of domestic violence, sexual abuse, and female foeticide. This module consolidates the physiological, programmatic, and gender-equity dimensions of adolescent and RMCH services.
References
- Park's Textbook of Preventive and Social Medicine, 26th ed., Ch 11 (RMNCH) & Ch 19 (Adolescent Health) (textbook)
Version 2.0 | NMC CBUC 2024
CLINICAL SCENARIO
A 16-year-old girl is brought to the PHC by her mother, who reports the girl has had amenorrhoea for 4 months. The mother is embarrassed and asks if the doctor can see the girl alone. When seen privately, the girl discloses she is married (child marriage, age 14), is 4 months pregnant, has a haemoglobin of 7.8 g/dL, and shows bruises on her arms consistent with repeated blunt trauma. She has never been to an ARSH clinic, has never received an IFA tablet, and was not aware of any government programme that could help her. As the PHC Medical Officer, what clinical, legal, and public health responses are simultaneously required?
WHY THIS MATTERS
Adolescent health sits at the intersection of every major public health domain — nutrition, reproductive health, mental health, gender equity, and programme delivery. In your PHC catchment, adolescents represent approximately 20% of your total population, but they are among the least likely to seek care voluntarily and the most likely to fall through the cracks between vertical programmes. The competencies in this module — from recognising Tanner stages to responding to domestic violence — are among the most ethically complex and practically demanding in the entire CBME curriculum.
RECALL
From your growth and development module, recall that puberty is driven by activation of the hypothalamic-pituitary-gonadal (HPG) axis: hypothalamic GnRH pulses trigger LH and FSH secretion, which drive gonadal steroidogenesis. From nutrition, recall that iron deficiency anaemia is the most prevalent micronutrient deficiency in India, and that the adolescent growth spurt — marked by the highest rate of lean mass accrual and red blood cell volume expansion in postnatal life — dramatically increases iron demand. From your epidemiology module, recall that child marriage (marriage before age 18 for girls) is associated with two-fold higher obstetric risk (immature pelvis, nutritional depletion), higher domestic violence risk, lower educational attainment, and higher lifetime fertility — it is both a health outcome and a social determinant of further health disparity.
Adolescent Health Burden in India
India's adolescent health burden is quantified by several overlapping indicators that reveal the intersection of biological vulnerability, social disadvantage, and gender discrimination. Anaemia is the single most prevalent adolescent health problem: NFHS-5 (2019-21) finds that 59.1% of girls aged 15-19 years are anaemic, making adolescent girls the most severely anaemic demographic group in India — higher than pregnant women (52.2%) or children under 5 (67.1% moderate-to-severe). The mechanism is a convergence of high physiological demand (growth spurt, menstrual blood loss), chronically inadequate dietary iron, and low absorption from predominantly plant-based Indian diets. Child marriage persists as a major adolescent health determinant: NFHS-5 reports that 23.3% of women aged 20-24 were married before age 18, a marker of educational deprivation, loss of bodily autonomy, and early entry into the high-risk-pregnancy demographic. Adolescent fertility — births to mothers aged 15-19 — carries the highest obstetric risk of any age group because the adolescent pelvis is not fully mature, and because adolescent girls are disproportionately anaemic, malnourished, and unregistered for ANC. Nutritional deficiencies beyond iron include protein-energy malnutrition (height-for-age stunting affects 35.5% of adolescent boys in NFHS-5), calcium deficiency (at a developmental phase when peak bone mass is still accruing), and iodine deficiency (neurological effects persist through late adolescence). Mental health: depression, anxiety, and substance use disorders peak in onset during adolescence — India's National Mental Health Survey estimated that 7.3% of adolescents have a diagnosable mental disorder, and suicide is the leading cause of death in the 15-29 age group. This mental health burden is substantially underrecognised in the community medicine programme, which has historically focused on physical health.
Determinants of Adolescent Health Outcomes and Gender Inequity
Poor adolescent health outcomes are not random — they cluster along well-defined social fault lines, with gender inequality as the primary axis. Understanding these determinants is essential for designing interventions that address root causes rather than symptoms. Son preference is the foundation of gender inequity in India: at the level of individual families, son preference drives sex-selective abortions (detectable as a skewed sex ratio at birth — NFHS-5: 929 girls per 1,000 boys, against a biological baseline of approximately 950-952) and female infanticide; at the level of household resource allocation it manifests as differential access to food, healthcare, and education. Adolescent girls are more likely to be pulled out of school to assist with domestic labour, married early, and restricted from seeking healthcare independently. Psychosocial development: Erik Erikson's model places adolescence (approximately 12-18 years) in the stage of identity vs role confusion — the developmental task is to integrate a coherent sense of self from among competing social roles (student, child, friend, emerging adult). For adolescent girls in joint-family contexts with early marriage, this developmental task is bypassed by externally imposed role assignment, foreclosing the psychosocial development that supports health-seeking autonomy. Poverty and education: every additional year of secondary school education for a girl reduces her lifetime fertility by approximately 0.3-0.5 births, reduces her risk of child marriage, and increases her economic agency — making girls' education the single highest-return investment in RMNCH outcomes. Peer influence: during adolescence, peer norms exert greater influence on behaviour than parental instructions — this is the mechanism that makes peer educator programmes (used in RKSK) more effective than didactic health education for adolescents.
SELF-CHECK
NFHS-5 reports the sex ratio at birth in India as 929 girls per 1,000 boys. What does this figure indicate, and which legal provision directly addresses the practice driving this deficit?
A. Normal biological variation; no legal intervention is required
B. Gender-based violence in hospitals; addressed by the Domestic Violence Act 2005
C. Sex-selective abortion and female foeticide driven by son preference; prohibited by the PCPNDT Act 1994
D. Underreporting of female births in rural areas; addressed by the Civil Registration System
Reveal Answer
Answer: C. Sex-selective abortion and female foeticide driven by son preference; prohibited by the PCPNDT Act 1994
The biological sex ratio at birth is approximately 950-952 girls per 1,000 boys; India's NFHS-5 figure of 929 is significantly below this and reflects son preference-driven sex-selective abortions and female foeticide. The Pre-Conception and Pre-Natal Diagnostic Techniques (PCPNDT) Act, enacted in 1994 and amended in 2003, prohibits the use of diagnostic techniques for sex determination for non-medical purposes and makes sex-selective abortion illegal. Penalties include imprisonment of up to 3 years and a fine. The PHC medical officer has a legal duty to report suspected PCPNDT violations to the District Appropriate Authority.
Physiology, Clinical Management and Principles of Adolescent Health
Adolescent health management begins with a thorough grounding in the physiology of puberty, because many of the clinical presentations encountered in adolescent practice — menstrual irregularity, primary amenorrhoea, growth faltering, acne — are only interpretable against the normal developmental baseline. Puberty is staged by the Tanner scale (also called Sexual Maturity Rating, SMR), which describes five stages from prepubertal (Stage 1) to adult phenotype (Stage 5). In girls, the pubertal sequence is: thelarche (breast bud appearance, Tanner Stage 2, typically at 9-11 years) → pubic hair growth (Tanner Stage 2-3) → peak height velocity (growth spurt, ~12 cm/year, occurring at Tanner Stage 3 in girls) → menarche (first menstruation, typically at Tanner Stage 3-4, average age 12.5-13 years in India). In boys: testicular enlargement (Stage 2, typically at 10-13 years) → pubic hair → spermarche (first ejaculation, approximately age 13) → peak height velocity (growth spurt at Tanner Stage 4, approximately 14 cm/year, later than girls). Nutritional requirements: the adolescent growth spurt creates peak demands for iron (girls need 12 mg/day through diet during active growth + menstrual replacement; boys 11 mg/day), calcium (1,300 mg/day for both sexes during 9-18 years — critical for peak bone mass accrual), and protein (52 g/day for boys, 46 g/day for girls at active growth). Clinical presentations: (1) Primary dysmenorrhoea (menstrual cramps without pelvic pathology) is the most common gynaecological complaint in adolescent girls — managed with NSAIDs (ibuprofen 400 mg 8-hourly, taken 1-2 days before expected onset) and heat therapy; (2) Primary amenorrhoea (no menarche by age 16 with secondary sexual characteristics, or by age 14 without) is an ARSH clinic red flag requiring referral for hormonal evaluation; (3) Acne (comedonal and inflammatory, driven by androgenic stimulation of sebaceous glands at puberty) — managed at ARSH clinics with topical retinoids and, when severe, oral tetracycline or doxycycline. Psychosocial issues commonly encountered in adolescent clinics: depression (PHQ-A screening), substance use (tobacco, alcohol, inhalants), and online or peer bullying — all require a non-judgemental, confidential, adolescent-friendly approach.
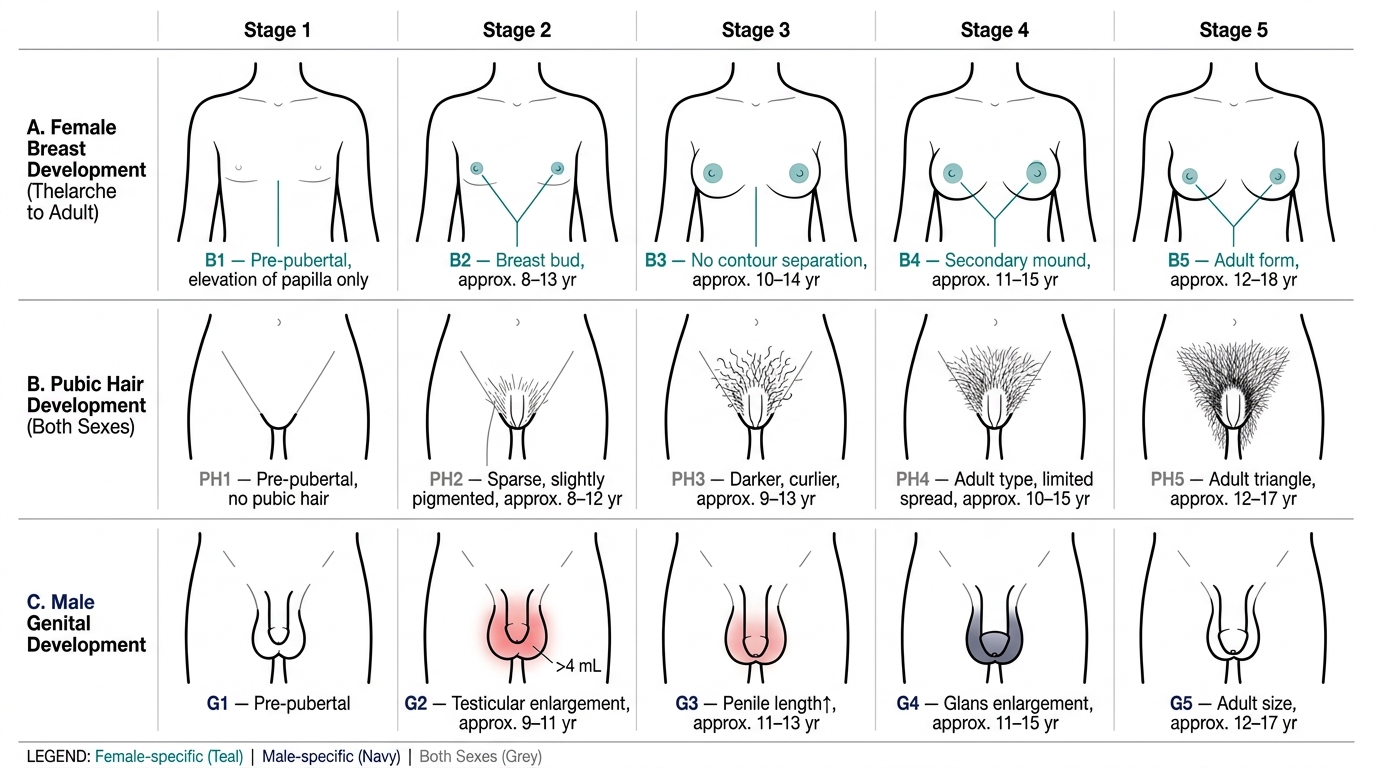
Tanner Stages of Puberty: Breast, Pubic Hair, and Genital Development