Page 21 of 27
CM10.8-10 | CM10.8-10 | Adolescent Health, Gender Issues and RMCH Services — SDL Guide (Part 2)
Adolescent Health Programmes: ARSH, RKSK, WIFS
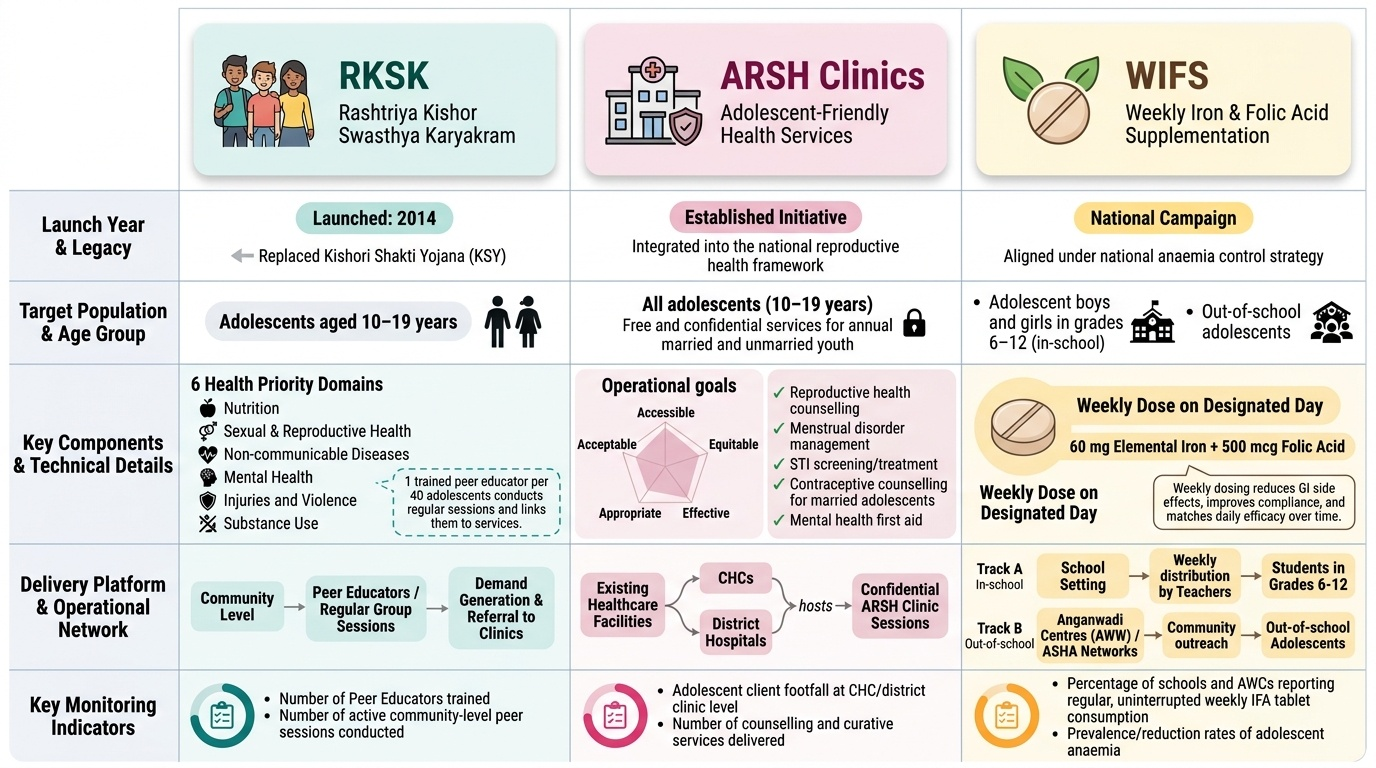
India's primary programmatic response to adolescent health is structured around three interconnected initiatives that address different dimensions of the burden. The Rashtriya Kishor Swasthya Karyakram (RKSK) — launched in 2014, replacing the earlier Kishori Shakti Yojana (KSY) — is the overarching national adolescent health programme targeting all adolescents aged 10-19 years (not only girls). It is organised around six health priority domains: (1) nutrition, (2) sexual and reproductive health, (3) non-communicable diseases, (4) mental health, (5) injuries and violence, and (6) substance use. The programme uses a community-based peer educator model: trained peer educators (adolescent volunteers selected from the community, 1 per 40 adolescents) conduct regular peer-group sessions, link community adolescents to ARSH clinic services, and conduct community-level demand generation. ARSH (Adolescent Reproductive and Sexual Health) clinics: designated sessions within existing CHC or district hospital facilities, providing adolescents with a package of services in a confidential, non-judgemental, adolescent-friendly setting — the five criteria for an adolescent-friendly health service are: accessible, acceptable, equitable, appropriate, and effective. ARSH clinic services include reproductive health counselling, treatment for menstrual disorders, STI screening and management, contraceptive counselling for married adolescents, and mental health first aid. WIFS (Weekly Iron and Folic Acid Supplementation): the GOI's programme to address the 59.1% adolescent anaemia prevalence. All adolescent girls and boys in grades 6-12 (and out-of-school adolescents through AWW/ASHA networks) receive one IFA tablet (60 mg elemental iron + 500 mcg folic acid) per week on a designated day. Weekly (not daily) supplementation is used because weekly dosing reduces gastrointestinal side effects, improves compliance, and evidence shows comparable efficacy for improving haemoglobin over time. WIFS is delivered through the school health programme in school settings and through ASHAs/AWWs for out-of-school adolescents.
Provided image
SELF-CHECK
A 13-year-old girl is enrolled in WIFS at school. She complains of nausea and stomach cramps every Monday (the designated WIFS day) after taking the tablet. What is the most appropriate advice?
A. Discontinue the IFA tablet — she is clearly allergic to iron
B. Change to daily dosing, which will resolve the side effects
C. Take the IFA tablet after a meal on Mondays; if symptoms persist, take it with fruit juice containing vitamin C to improve absorption and tolerance
D. Switch her to injectable iron dextran at the ARSH clinic
Reveal Answer
Answer: C. Take the IFA tablet after a meal on Mondays; if symptoms persist, take it with fruit juice containing vitamin C to improve absorption and tolerance
Gastrointestinal side effects (nausea, cramping, constipation) are the most common reason for WIFS non-adherence, and the primary management is to take the tablet after food — this reduces gastric irritation without significantly impairing absorption. Vitamin C-containing juice alongside enhances non-haem iron absorption. Option A is incorrect — GI symptoms are a dose-related pharmacological side effect of oral iron, not an allergic reaction. Option B is wrong — daily dosing typically causes MORE gastrointestinal side effects than weekly dosing, not fewer (one reason WIFS specifically uses weekly dosing). Injectable iron is reserved for severe, symptomatic iron deficiency anaemia that fails oral therapy, not for GI side effects.
Gender Issues, Women Empowerment and RMCH Services
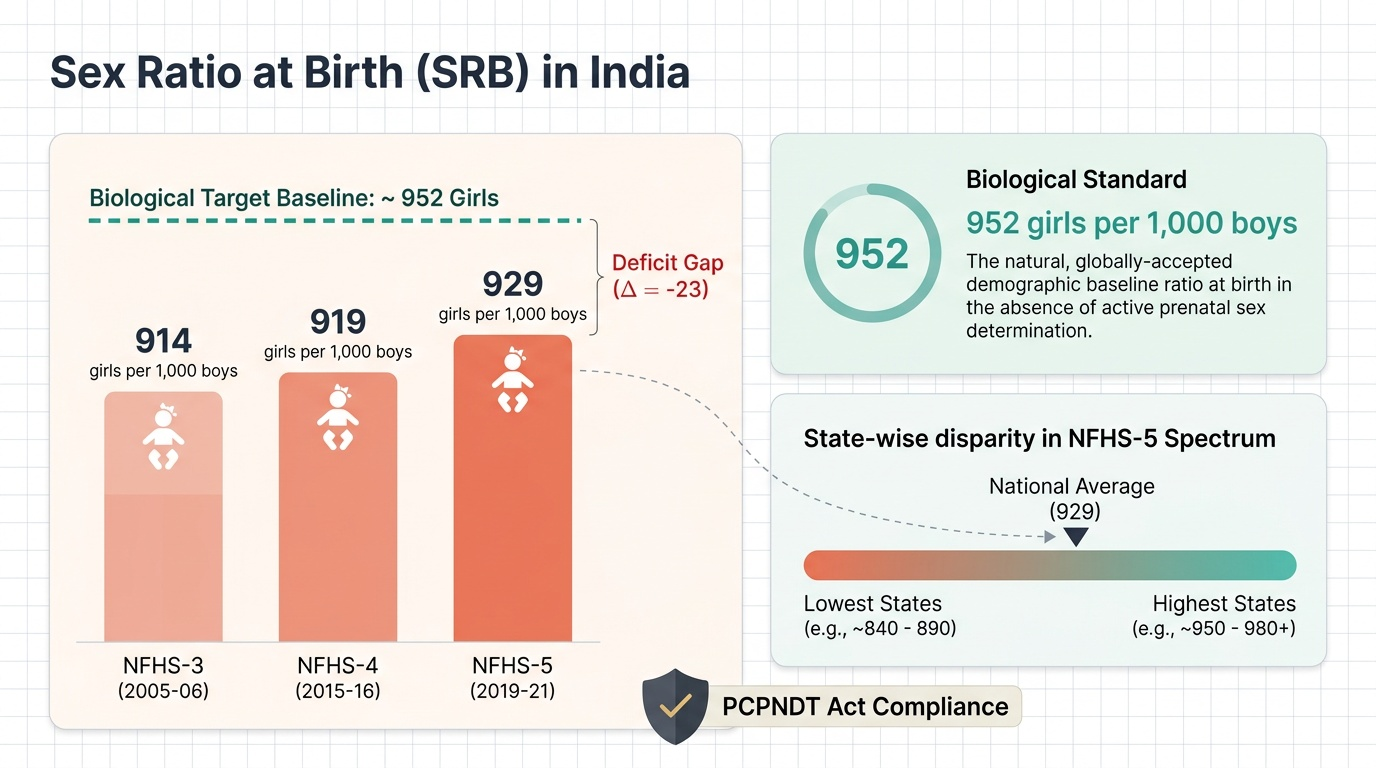
Gender is a social construct — it refers to the socially defined roles, behaviours, and attributes that a society assigns to women and men — as distinct from sex, which is the biological classification (chromosomal, gonadal, anatomical). Gender inequity in health arises when this social construct systematically disadvantages one group, usually women, in access to resources, healthcare, and decision-making. Gender-based violence (GBV) encompasses all violence directed at individuals because of their gender — including domestic violence, sexual violence (including marital rape), early and forced marriage, honour killings, and female foeticide. The Domestic Violence Act 2005 (Protection of Women from Domestic Violence Act) defines domestic violence broadly to include physical, sexual, verbal, emotional, and economic abuse within a shared household; it provides for protection orders, residence orders, and monetary relief. Son preference is quantifiable through the sex ratio at birth: NFHS-5 India = 929 girls per 1,000 boys, against the biological baseline of approximately 952 girls per 1,000 boys; the deficit represents sex-selective abortions facilitated by prenatal sex determination. The PCPNDT Act (1994, amended 2003) prohibits prenatal sex determination for non-medical purposes and sex-selective abortion; every registered ultrasound centre must maintain a Form F (patient particulars) register that the PHC medical officer and District Appropriate Authority are required to inspect. At the community level, the PHC medical officer has a mandatory legal duty: any suspicion of PCPNDT violation must be reported to the District Appropriate Authority; failure to report is itself an offence. Women empowerment is measured through composite indices: the Gender Development Index (GDI) (ratio of female to male HDI), the Gender Inequality Index (GII) (composite of reproductive health, empowerment, and labour market participation), and sector-specific indicators (female literacy rate, female work participation rate, women in local governance — Panchayats have 33-50% reservation for women in many states). In RMCH services, gender-responsive care means: ARSH clinics with female staff or private-room options, POSH (Prevention of Sexual Harassment) compliance in facilities, community-level female health worker networks (ASHA, ANM, AWW), and counselling protocols that address intimate partner violence as a health risk. The POCSO Act 2012 (Protection of Children from Sexual Offences) mandates that all health workers who become aware of sexual abuse of a person under 18 years must report it to the police or the Child Welfare Committee — this is a mandatory reporting obligation, not discretionary.
Provided image
CLINICAL PEARL
When an adolescent presents to the PHC with bruises, unconvincing explanations, and signs of nutritional neglect — as in the hook scenario — the clinical response must integrate three parallel tracks simultaneously: (1) medical (manage anaemia, assess pregnancy and obstetric risk); (2) legal (mandatory POCSO reporting if the patient is under 18, mandatory reporting of domestic violence if she discloses it); and (3) social (engage the district child protection officer, identify a safe house or shelter if the home is unsafe). The trap is to follow only one track — treating the anaemia and sending her home, or reporting to police without medical management, or providing social support without treating the clinical condition. All three tracks are simultaneous, not sequential.
Monitoring and Evaluation of Adolescent and Gender Programmes
Monitoring adolescent health and gender programme performance requires a distinct set of indicators that capture the intersecting biological and social dimensions of this population. For adolescent nutrition, NFHS-5 provides district-level anaemia prevalence by age-sex group; WIFS programme monitoring uses the monthly WIFS register (tablets distributed vs enrolled students) to calculate tablet distribution rate and periodic haemoglobin improvement assessment at mid-term and end-term using WHO cut-offs (<12 g/dL = anaemia in non-pregnant women ≥15 years). For RKSK and ARSH, programme quality is assessed by: number of trained peer educators per adolescent population, ARSH clinic utilisation rate (number of adolescents attending per month as a proportion of eligible population), and the proportion of adolescents screened for anaemia, BMI, and reproductive health issues. For gender programme monitoring, the key indicators are: sex ratio at birth (NFHS and SRS), child marriage prevalence (NFHS by district), female literacy rate (Census), women's participation in gram panchayats (election commission data), and PCPNDT registration compliance (percentage of ultrasound centres in the district with current Form F compliance). Adolescent fertility rate — the annual birth rate per 1,000 girls aged 15-19 — is the demographic outcome indicator for adolescent reproductive health: India's NFHS-5 adolescent fertility rate is 43 per 1,000, down from 54 per 1,000 in NFHS-4. The Beti Bachao Beti Padhao (BBBP) programme, launched 2015 targeting districts with sex ratio at birth below 918 girls per 1,000 boys, uses sex ratio at birth improvement as the primary programme outcome indicator, monitored quarterly through the district health management system.
SELF-CHECK
A health worker at a PHC discovers during a home visit that a 17-year-old girl has been sexually abused by a family member. The girl begs the health worker not to report to anyone. What is the correct legal and ethical response?
A. Respect the girl's autonomy and maintain confidentiality — she is old enough to make her own decisions
B. Report to the family elder and ask them to handle the matter internally
C. File a mandatory report under POCSO 2012 to the police or Child Welfare Committee, regardless of the victim's wishes
D. Refer her to a counsellor and defer reporting until she consents
Reveal Answer
Answer: C. File a mandatory report under POCSO 2012 to the police or Child Welfare Committee, regardless of the victim's wishes
Under POCSO 2012 (Protection of Children from Sexual Offences Act), any person — including health workers — who has knowledge of or reason to suspect that a child (person under 18 years) has been the victim of a sexual offence has a mandatory obligation to report it to the local police station or Child Welfare Committee within 24 hours. This is a statutory duty, not a discretionary decision — failure to report is itself a criminal offence under Section 21 of POCSO. The victim's consent or refusal is not a legal precondition for reporting; the law explicitly overrides victim confidentiality in cases involving minors. The correct response also includes medical management, documentation of injuries, and engagement of child protection services.