Page 1 of 13
DR1.2 | Acne Management Planning — SDL Guide
Learning Objectives
- Devise a severity-matched, step-wise management plan for acne (mild, moderate, severe, and hormonal-pattern presentations)
- Describe the topical agents — retinoids, azelaic acid, benzoyl peroxide, and antibiotics — their mechanisms, key adverse effects, and combination rules
- State the indications, dosing principles, monitoring, and absolute teratogenic contraindication of oral isotretinoin, including mandatory pregnancy prevention
- Recognise and systematically address treatment failure, and identify when hormonal therapy or investigation for hyperandrogenism is appropriate
INSTRUCTIONS
Recognising and grading acne is only useful if it leads to a safe, effective treatment plan — and acne is so common that every doctor must be able to write one. This module converts the severity grade into a step-wise management plan: topical agents for mild disease, an added oral antibiotic for moderate disease, oral isotretinoin for severe or refractory disease, and hormonal therapy for women with a hormonal pattern. It places particular emphasis on the safety-critical decisions that distinguish good acne care from harm — above all the teratogenicity of isotretinoin and its mandatory pregnancy prevention, and the antibiotic-stewardship rules that prevent resistance — so that your plans are not only effective but safe.
References
- Neena Khanna. Illustrated Synopsis of Dermatology & Sexually Transmitted Diseases, 6th ed. Ch: Acne — Treatment (textbook)
- IADVL Textbook of Dermatology. Ch: Management of Acne (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
Two patients arrive in your OPD on the same morning. The first is a 15-year-old boy with scattered blackheads and whiteheads over his nose and forehead and just a few small red papules — his skin barely troubles him, but his mother wants 'something done.' The second is a 16-year-old girl with deep, tender nodules and pus-filled cysts over both cheeks and the jaw, several already healing into pitted scars; she has tried three creams from a pharmacy with no benefit and is in tears. Both have acne vulgaris, yet prescribing the same treatment to both would be a serious error — the boy needs a single topical agent, while the girl needs systemic therapy and possibly the most powerful (and most hazardous) acne drug we have. This module teaches you to convert a severity grade into a safe, individualised management plan, and to handle the safety-critical decisions — above all the teratogenicity of isotretinoin — that separate good acne care from harm.
WHY THIS MATTERS
Devising an acne management plan is a core competency for every MBBS graduate because acne is so common that you will treat it whatever speciality you enter, and because the consequences of getting it wrong are real and lasting. Under-treat severe acne and the patient is left with permanent scars and the psychological burden that drives adolescents to depression and social withdrawal; over-treat or mis-prescribe and you expose a young person to needless drug toxicity — most gravely, a serious birth defect if isotretinoin is given to a woman who becomes pregnant. A rational, severity-matched plan also tackles the public-health problem of antibiotic resistance, which is worsened by the careless long-term antibiotic monotherapy still common in practice. Knowing not just which drugs exist but how to sequence, combine, and monitor them — and how to counsel the patient so the plan actually works — is what this module builds.
RECALL
Before devising treatment, recall from the recognition-and-grading SDL of this cluster the two things that govern every decision here. First, recall the four pillars of acne pathogenesis — androgen-driven excess sebum, follicular hyperkeratinisation, Cutibacterium acnes proliferation, and inflammation — because each drug class works by attacking one or more of these pillars. Second, recall severity grading: mild (mainly comedonal), moderate (inflammatory papulopustular), and severe (nodulocystic, scarring, or refractory), assessed with the IGA or GAGS scale, with nodules, cysts, or scarring marking severe disease regardless of count. The grade you assigned in that SDL is the single input that determines where on the treatment ladder you start, so keep it firmly in mind as we build the plan.
Clinical Presentations Driving Treatment Choice
Clinical Presentation Guides Acne Treatment Choice
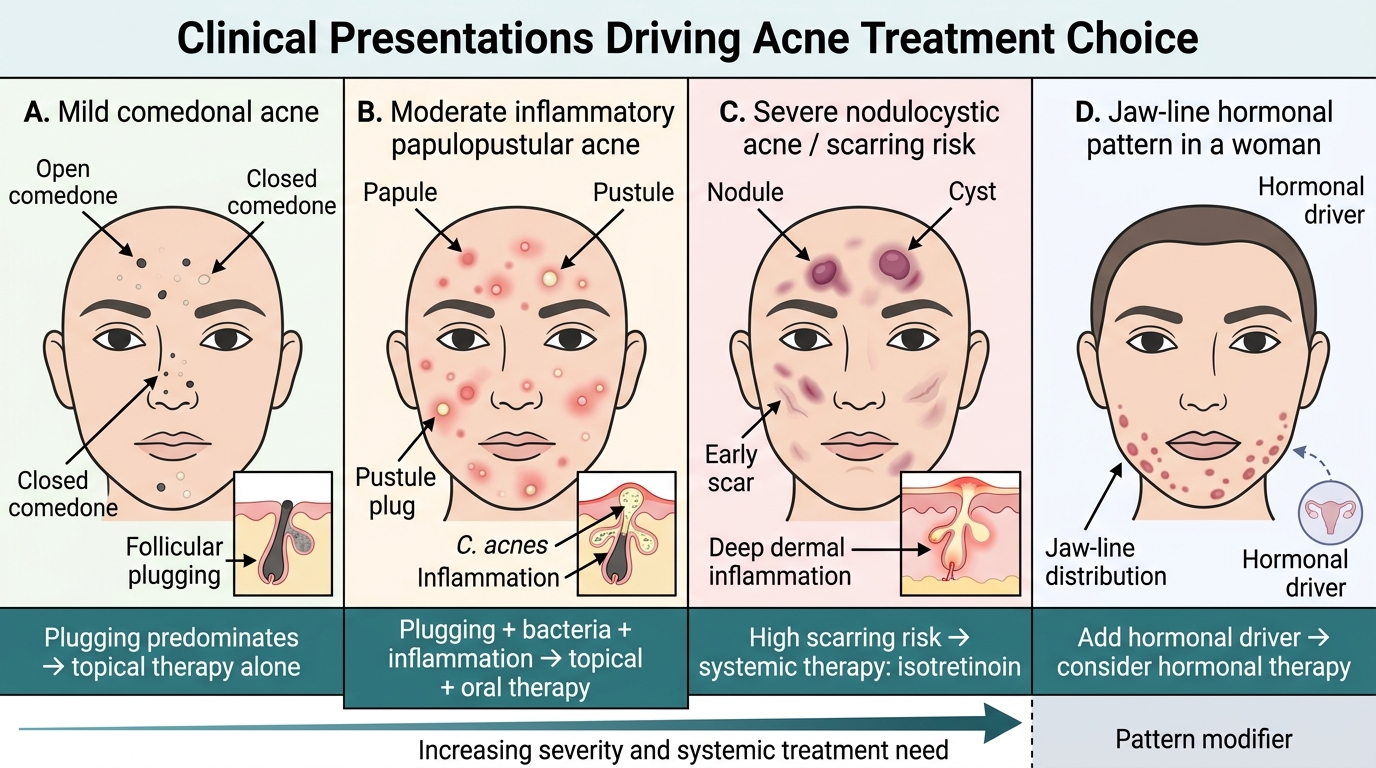
Every acne management plan begins not with a drug but with a clear reading of the clinical picture in front of you, because the predominant lesion type and the severity grade are what point you to the right rung of the treatment ladder. A face dominated by blackheads and whiteheads with little redness is comedonal acne, and it tells you the problem is mainly follicular plugging — a presentation that responds to a topical agent that normalises keratinisation. A face with numerous red papules and pus-filled pustules spread across several regions is moderate inflammatory acne, signalling that C. acnes and inflammation have joined plugging as active drivers and that topical therapy alone will usually be insufficient. A face bearing deep tender nodules, cysts, or early scars is severe nodulocystic acne, where the scarring risk is high and only systemic therapy will reliably help. Reading the presentation this way means the treatment decision is half-made before you reach for the prescription pad.
The presentation-to-decision link can be summarised as:
- Comedonal-predominant, mild: problem is plugging → topical therapy alone.
- Inflammatory papulopustular, moderate: plugging + bacteria + inflammation → topical plus oral therapy.
- Nodulocystic / scarring, severe: deep inflammation, high scarring risk → systemic therapy (isotretinoin).
- Jaw-line / hormonal pattern in a woman: consider an added hormonal driver → hormonal therapy as an option.
Throughout, the patient's own distress and the presence of scarring may justify treating more aggressively than the lesion count alone would suggest — a patient scarring before your eyes cannot wait for a slow ladder.
How Treatments Work: Mechanisms Targeting Pathogenesis
How Acne Treatments Target Pathogenesis
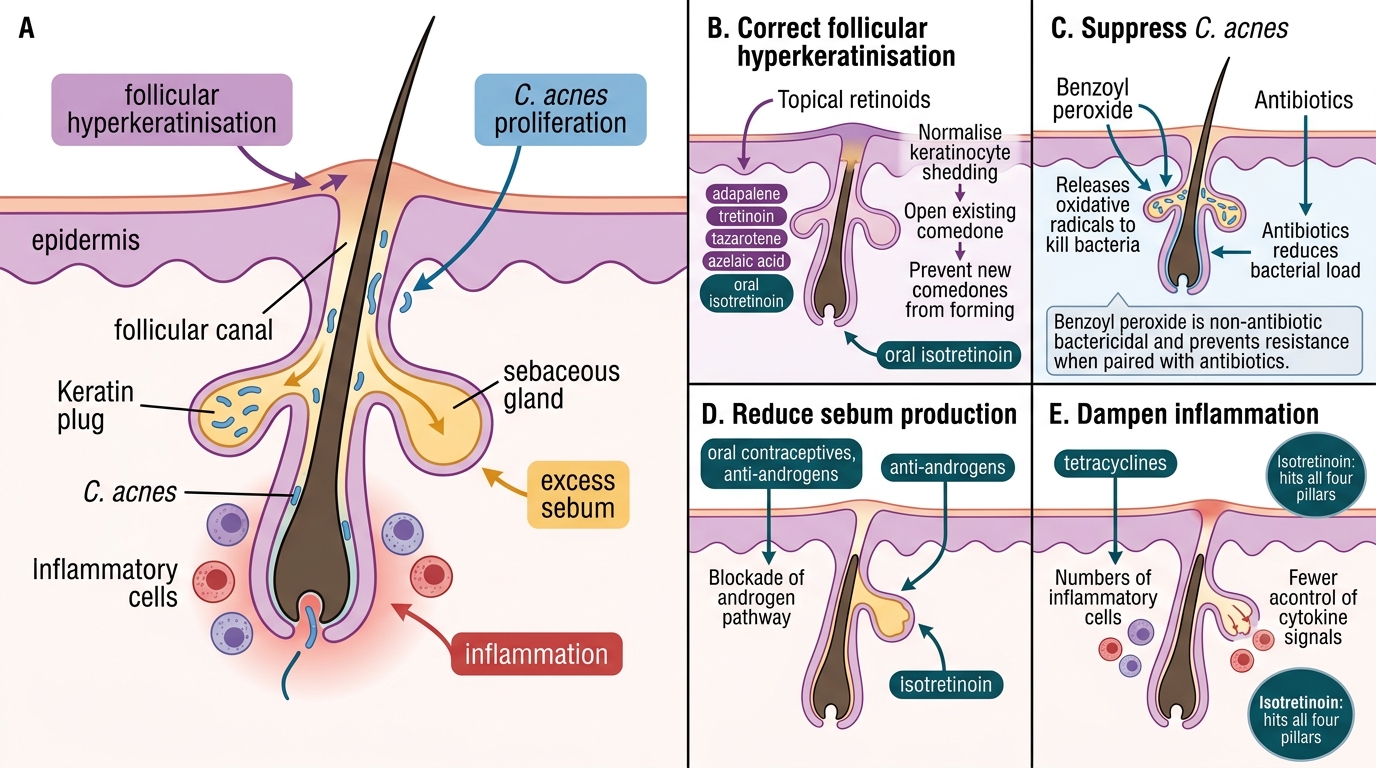
Acne pharmacotherapy becomes logical rather than a list to memorise once you map each drug class onto the pathogenetic pillar it attacks, because every rational plan combines agents that together cover all four pillars. Topical and systemic retinoids are the only agents that directly correct follicular hyperkeratinisation — they normalise the shedding of follicular keratinocytes, dissolve existing comedones, and prevent new ones, which is why a retinoid is the backbone of almost every plan. Benzoyl peroxide and antibiotics (topical and oral) suppress C. acnes; benzoyl peroxide does so as a non-antibiotic bactericidal that the organism cannot become resistant to, which is precisely why it is always paired with an antibiotic. Hormonal agents and oral isotretinoin reduce sebum production by acting on the androgen pathway and the sebaceous gland respectively. Inflammation is dampened both directly (by tetracyclines' anti-inflammatory action) and indirectly as the other pillars are controlled. Isotretinoin is unique in hitting all four pillars at once, which explains its unmatched efficacy.
Mapping class to pillar:
- Follicular hyperkeratinisation → topical retinoids (adapalene, tretinoin, tazarotene), azelaic acid, oral isotretinoin.
- C. acnes → benzoyl peroxide, topical/oral antibiotics, azelaic acid.
- Excess sebum → oral isotretinoin, hormonal agents (oral contraceptives, anti-androgens).
- Inflammation → oral tetracyclines (anti-inflammatory), and resolution as other pillars are controlled.
Because no single class covers every pillar except isotretinoin, combination therapy that pairs a retinoid with an anti-C. acnes agent is the standard backbone for most patients.
SELF-CHECK
Why is a topical retinoid considered the backbone of most acne treatment plans, in terms of the four pillars of pathogenesis?
A. Because it is the only agent that kills Cutibacterium acnes directly
B. Because it directly corrects follicular hyperkeratinisation — dissolving existing comedones and preventing new ones at their source
C. Because it is the only agent that reduces sebum production
D. Because it has no irritant side effects and is therefore safe for everyone
Reveal Answer
Answer: B. Because it directly corrects follicular hyperkeratinisation — dissolving existing comedones and preventing new ones at their source
Topical retinoids are the backbone of acne therapy because they directly target follicular hyperkeratinisation — the very first step of acne pathogenesis. By normalising the abnormal cohesion and retention of follicular keratinocytes, they dissolve existing comedones and, crucially, prevent the formation of new microcomedones, halting acne at its source. Benzoyl peroxide and antibiotics tackle C. acnes, and isotretinoin/hormonal agents reduce sebum, but only retinoids correct the plugging that initiates every lesion. Retinoids are also irritant and photolabile (tretinoin especially), so they require correct counselling rather than being free of side effects.
Step-Therapy Ladder: Matching Treatment to Severity
Acne Step-Therapy Ladder
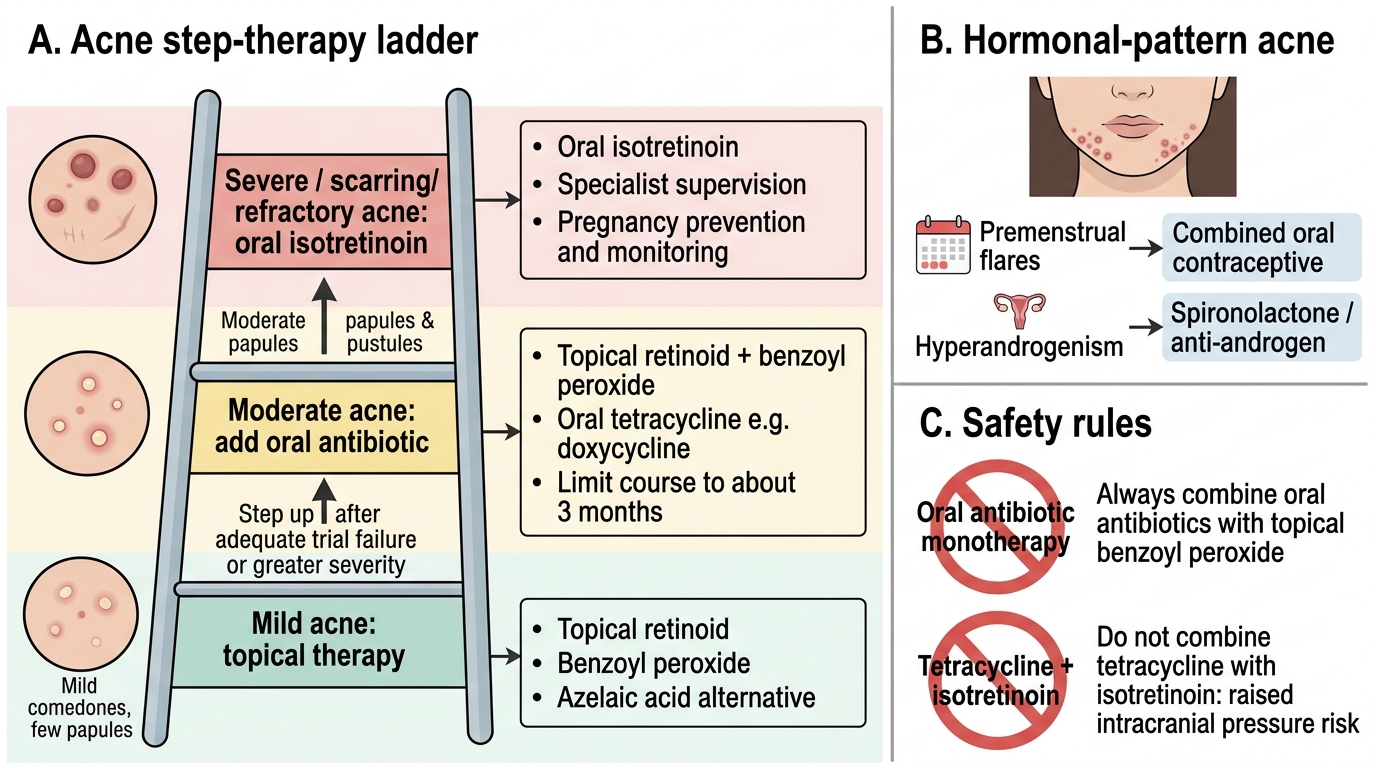
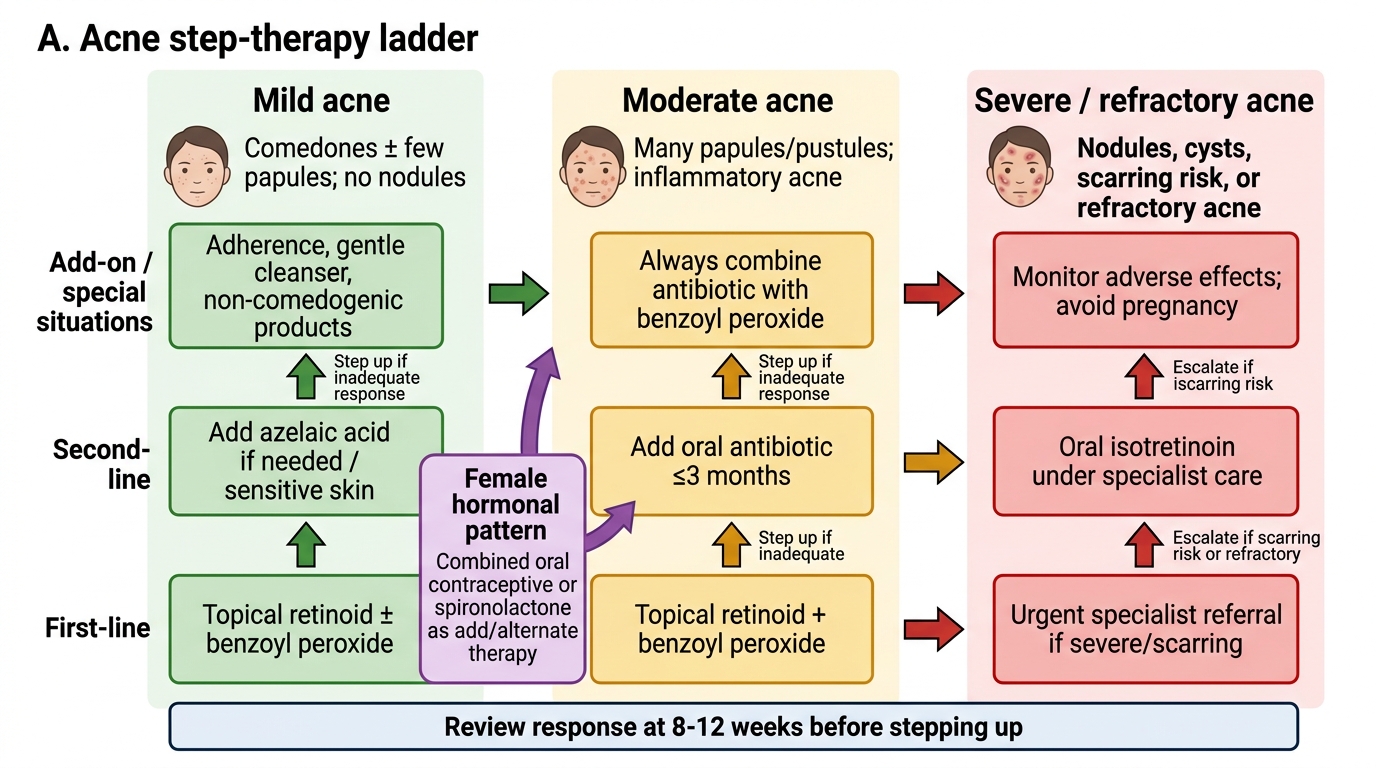
The central organising principle of acne management is severity-matched step therapy: you start at the rung of the ladder that corresponds to the patient's grade, and you step up only if an adequate trial fails or the disease is more severe than first thought. For mild acne, topical therapy alone is sufficient — typically a topical retinoid, often combined with benzoyl peroxide, with azelaic acid as a useful alternative. For moderate acne, you add an oral antibiotic (a tetracycline such as doxycycline) to topical therapy, always co-prescribing topical benzoyl peroxide to limit resistance, and you limit the antibiotic course to about three months. For severe nodulocystic, scarring, or treatment-refractory acne, the plan moves to oral isotretinoin under specialist supervision. For a woman with a hormonal pattern — jaw-line acne, premenstrual flares, or signs of hyperandrogenism — combined oral contraceptives or an anti-androgen such as spironolactone are valuable additions or alternatives. A vital safety rule threads through the whole ladder: oral antibiotics are never used as monotherapy, and they are never combined with oral isotretinoin (the tetracycline–isotretinoin combination risks raised intracranial pressure).
Acne Step-Therapy Ladder
The ladder, summarised:
- Mild: topical retinoid ± benzoyl peroxide (± azelaic acid).
- Moderate: above PLUS an oral antibiotic (≤3 months, always with benzoyl peroxide).
- Severe / refractory: oral isotretinoin (specialist).
- Female hormonal pattern: add/alternate with combined oral contraceptive or spironolactone.
Review response at 8–12 weeks before deciding to step up, because topical and antibiotic effects take that long to declare themselves.