Page 2 of 13
DR1.2 | Acne Management Planning — SDL Guide (Part 2)
Topical Agents: Retinoids, Azelaic Acid, BPO, and Antibiotics
Topical Acne Agents: Sites of Action and Prescribing Rules
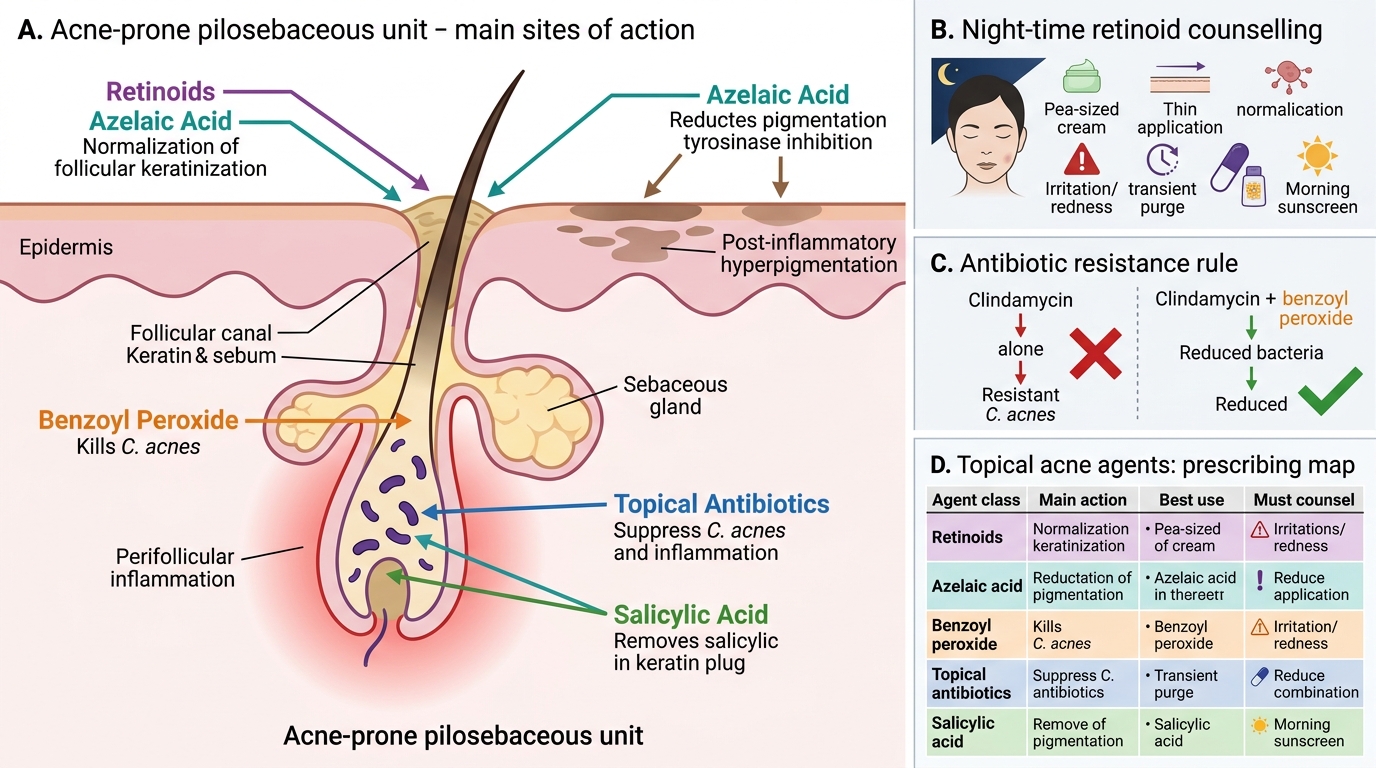
Topical agents are the foundation of acne treatment and are used at every rung of the ladder, so prescribing them correctly — and counselling the patient on how to use them — is the most widely applicable skill in this module. Topical retinoids (adapalene, tretinoin, tazarotene) are first-line for comedonal and mild-to-moderate acne; they are applied thinly at night, commonly cause an initial irritation and a transient 'purge,' and tretinoin in particular is photodegradable and photosensitising, so night-time use plus daytime sunscreen must be counselled. Azelaic acid deserves special mention for Indian skin because it is genuinely multi-functional: it is anti-comedonal (normalising keratinisation), antimicrobial against C. acnes, AND anti-pigmentary (inhibiting tyrosinase), making it especially valuable where post-inflammatory hyperpigmentation accompanies the acne. Salicylic acid is a keratolytic adjunct useful in comedonal acne. Benzoyl peroxide (BPO) is a non-antibiotic bactericidal whose great virtue is that C. acnes cannot develop resistance to it, so it is the essential partner for any antibiotic. Topical antibiotics (clindamycin, erythromycin) must never be used alone — always with BPO or a retinoid — to slow the emergence of resistance.
Topical Acne Agents: Comparison and Prescribing Rules
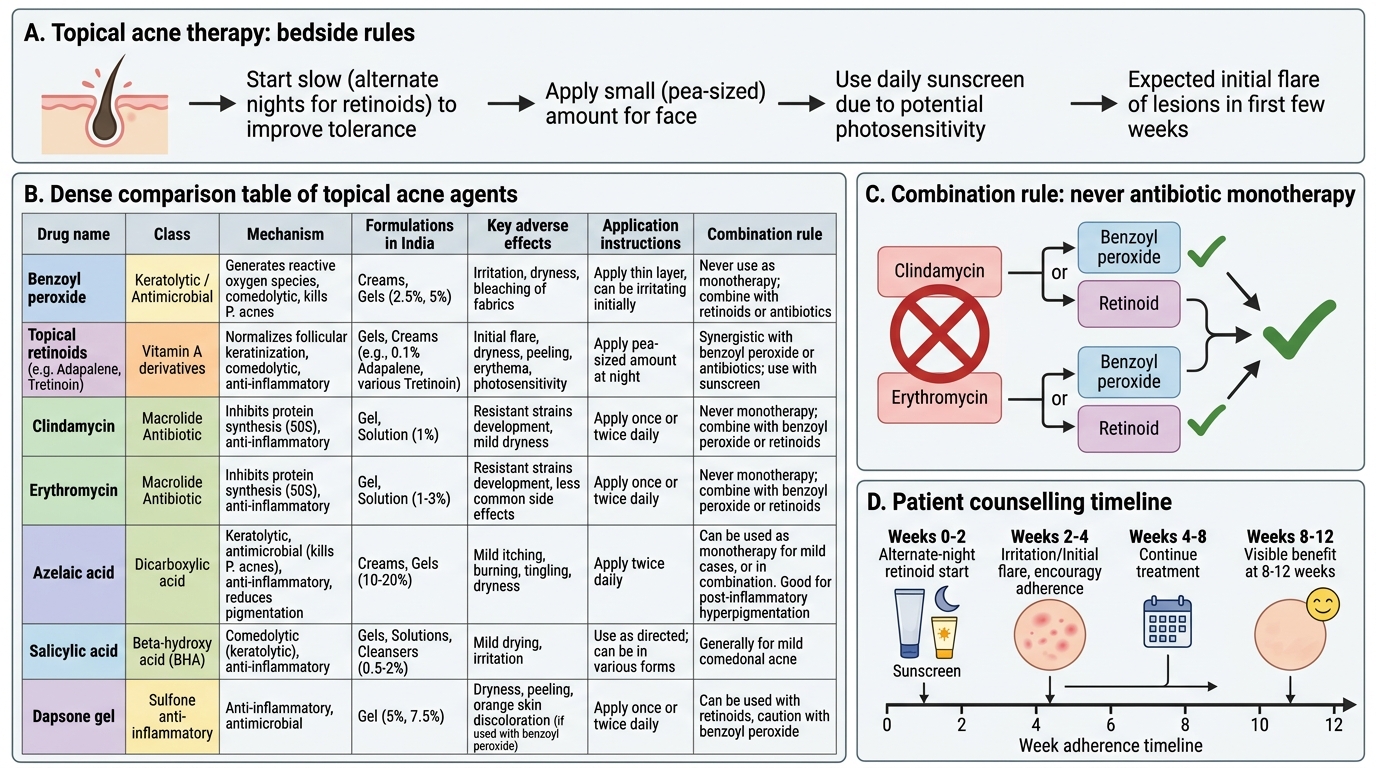
The key topical-prescribing rules to carry to the bedside:
- Always pair a topical antibiotic with benzoyl peroxide (or a retinoid) — never antibiotic monotherapy.
- Counsel on retinoid irritation and photosensitivity — start on alternate nights, use a sunscreen, expect an initial flare.
- Choose azelaic acid when post-inflammatory hyperpigmentation is a prominent concern, or in pregnancy where retinoids are contraindicated.
- Set expectations: topical benefit takes 8–12 weeks; adherence is the commonest reason for apparent failure.
SELF-CHECK
A topical antibiotic such as clindamycin should NOT be prescribed as monotherapy for acne. What is the minimum co-prescription rule, and why?
A. Co-prescribe an oral antibiotic, to achieve higher tissue levels
B. Co-prescribe topical benzoyl peroxide (or a retinoid), because benzoyl peroxide is a non-antibiotic bactericidal that reduces the emergence of C. acnes resistance
C. Co-prescribe a topical steroid, to reduce irritation
D. No co-prescription is needed if the course is kept under two weeks
Reveal Answer
Answer: B. Co-prescribe topical benzoyl peroxide (or a retinoid), because benzoyl peroxide is a non-antibiotic bactericidal that reduces the emergence of C. acnes resistance
Topical (and oral) antibiotics used alone for acne promote antibiotic resistance in Cutibacterium acnes, which is a growing problem. The minimum rule is to combine a topical antibiotic with topical benzoyl peroxide (or with a retinoid). Benzoyl peroxide is a non-antibiotic bactericidal agent: because it kills bacteria by oxidation rather than a specific antibiotic target, C. acnes cannot develop resistance to it, and co-using it markedly reduces the selection of antibiotic-resistant organisms. This is why fixed-dose clindamycin–benzoyl peroxide combinations are popular, and why antibiotic monotherapy is considered poor practice.
Differential Diagnosis of Treatment Failure and Acne Mimics
Differential Diagnosis of Acne Treatment Failure
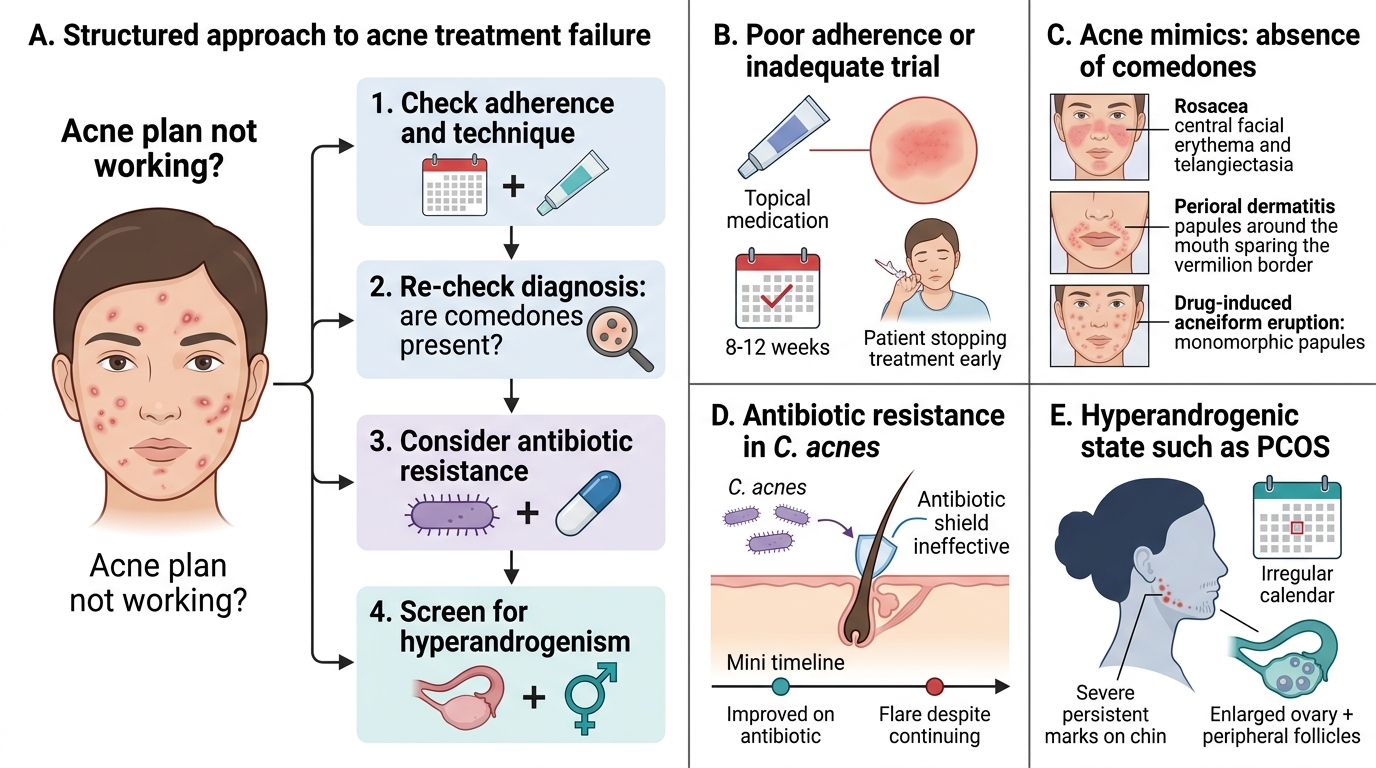
When an acne plan does not work, the right response is not simply to escalate the dose but to ask systematically why it failed, because the commonest reasons for apparent treatment failure are correctable and do not call for stronger drugs at all. By far the most frequent cause is poor adherence — topical regimens are demanding, irritation drives patients to stop early, and benefit takes two to three months to appear, so many 'failures' are really patients who never completed an adequate trial. The second consideration is whether the diagnosis is even correct: a 'non-responding acne' may actually be rosacea, perioral dermatitis, or a drug-induced acneiform eruption, none of which respond to standard acne treatment, and the absence of comedones should make you reconsider. The third is antibiotic resistance in C. acnes, suspected when a patient who improved on an antibiotic then flares despite continuing it. The fourth is an underlying hyperandrogenic state such as PCOS in a woman whose acne is severe, persistent, or accompanied by hirsutism and menstrual irregularity, which needs investigation and hormonal treatment rather than ever-stronger topicals.
A structured approach to the non-responder:
- Re-check adherence and technique first — is the patient actually using the regimen, for long enough, correctly?
- Re-check the diagnosis — are there comedones? If not, consider rosacea, perioral dermatitis, or an acneiform eruption.
- Consider antibiotic resistance — flare while on an antibiotic, or repeated antibiotic courses.
- Investigate for hyperandrogenism — severe/persistent acne in a woman with hirsutism or irregular cycles (testosterone, DHEAS, LH:FSH ratio, pelvic ultrasound).
Only once these are addressed does true treatment-resistant severe acne — the appropriate indication for isotretinoin — remain as the explanation.
Oral Isotretinoin: Indications, Dosing, and Safety
Oral Isotretinoin: Indications, Dosing, and Safety
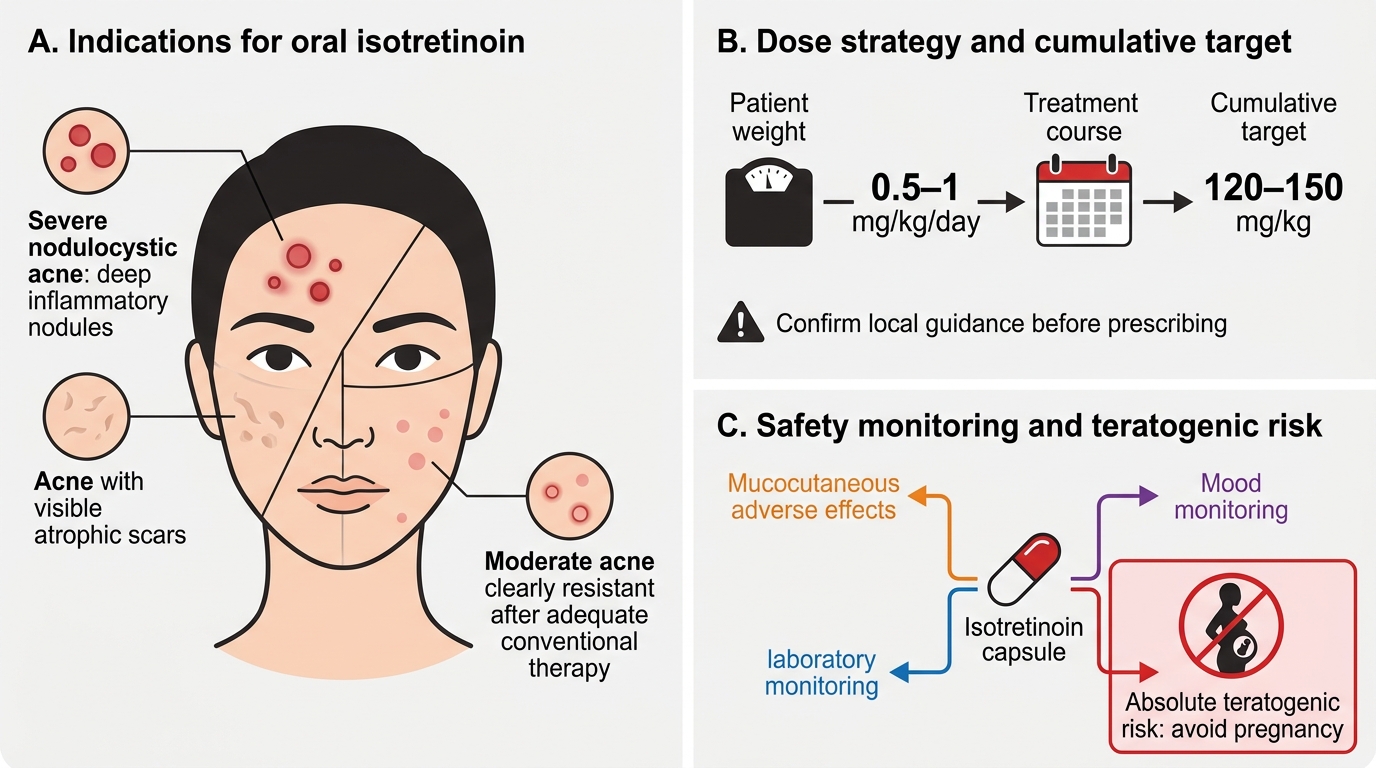
Oral isotretinoin (13-cis-retinoic acid) is the single most effective acne drug — it is the only agent that targets all four pathogenetic pillars and can produce prolonged remission — but it is also the most hazardous, so its indications, dosing, monitoring, and above all its safety rules must be understood precisely. Its accepted indications are severe nodulocystic acne, acne that has scarred or is scarring, and moderate acne that has failed adequate conventional therapy including oral antibiotics. Typical dosing is 0.5–1 mg/kg/day, and treatment is generally continued to a cumulative dose target of approximately 120–150 mg/kg, which is associated with the lowest relapse rates (you should confirm the exact cumulative figure and current dosing against your prescribed reference and local dermatology guidance before prescribing). Because the drug is a retinoid, it has predictable mucocutaneous effects — cheilitis, dry skin and eyes, epistaxis — and requires laboratory monitoring of liver function tests and fasting lipids, plus attention to mood, as a small risk of mood disturbance is reported. None of these, however, is as critical as its teratogenicity, which dominates every decision to prescribe it in a woman of childbearing potential.
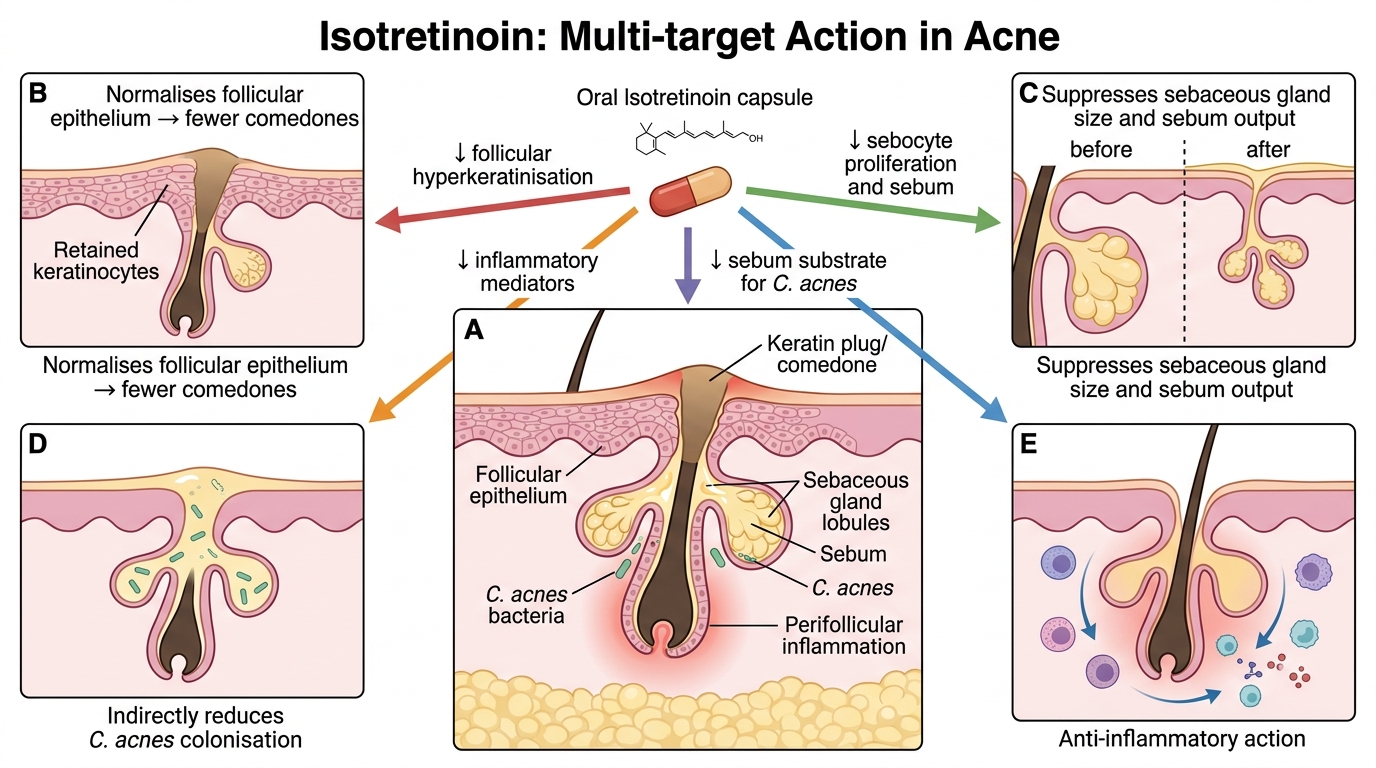
Isotretinoin: Multi-target Action in Acne
The safety framework for isotretinoin:
- Teratogenicity is an ABSOLUTE contraindication in pregnancy — isotretinoin causes severe birth defects, so pregnancy must be excluded before starting and rigorously prevented throughout.
- Mandatory pregnancy prevention in women of childbearing potential: a negative pregnancy test before starting, effective contraception (ideally two methods) during treatment and for the period after stopping specified by your guideline, and repeat pregnancy testing during therapy (the iPLEDGE-type programme in the US; follow current CDSCO/local protocols in India — confirm with faculty).
- Monitor LFTs and fasting lipids at baseline and during treatment; counsel on mucocutaneous effects and mood.
- Do NOT co-prescribe a tetracycline with isotretinoin — the combination risks benign intracranial hypertension.
Isotretinoin is best initiated and supervised by a dermatologist; the MBBS graduate's role is to recognise the indication, refer appropriately, and understand the safety rules well enough to counsel and to recognise complications.