Page 6 of 13
DR1.1 | Acne Recognition and Grading — SDL Guide (Part 2)
Grading Acne Severity: IGA and GAGS
Acne Grading: IGA and GAGS
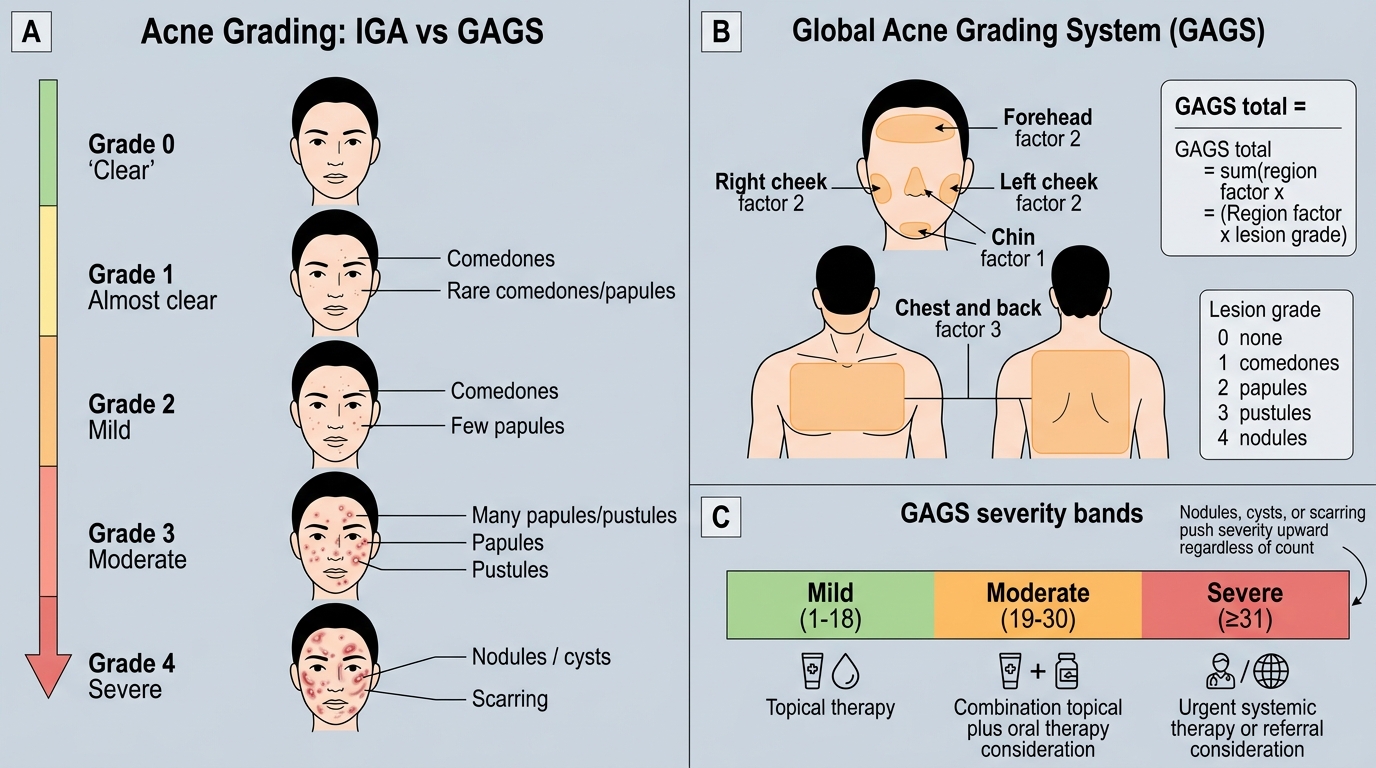
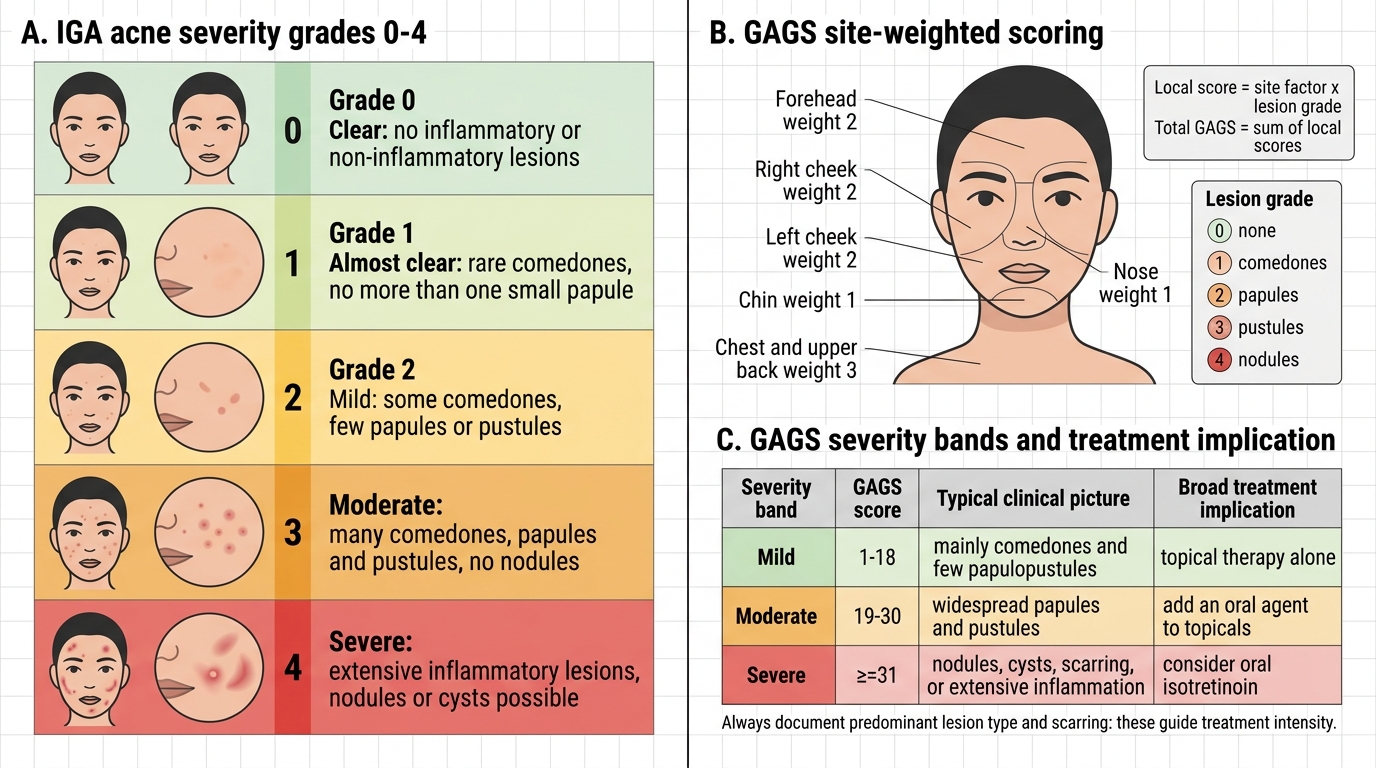
Once you can name the lesions, you must convert that observation into a severity grade, because the grade — not the patient's distress alone — drives the choice of treatment in every guideline. Severity in acne depends on three things working together: the predominant lesion type (comedonal versus inflammatory versus nodular), the number of lesions, and the extent of the body involved, with the presence of nodules, cysts, or scarring automatically pushing a patient toward the severe end regardless of count. Two grading approaches are commonly used in Indian practice and you should know both. The Investigator's Global Assessment (IGA) is a quick five-point clinical scale (grade 0 clear, 1 almost clear, 2 mild, 3 moderate, 4 severe) that is fast at the bedside and widely used in clinical trials of topical agents. The Global Acne Grading System (GAGS) is a more objective, site-weighted score that multiplies a lesion-density grade at six facial/trunk regions (forehead, each cheek, nose, chin, chest-and-back) by a region factor and sums them, giving a total that bands severity.
Acne Grading: IGA vs GAGS
A simple, practical way to remember the GAGS bands and what they mean clinically:
| Severity band | GAGS score | Typical clinical picture | Broad treatment implication |
|---|---|---|---|
| Mild | 1–18 | Mainly comedones, few papulopustules | Topical therapy alone |
| Moderate | 19–30 | Widespread papules and pustules | Add an oral agent to topicals |
| Severe | ≥31 | Nodules, cysts, scarring, or extensive inflammation | Consider oral isotretinoin |
Whatever scale you use, always document the predominant lesion type and whether scarring is present, because those two observations carry as much weight as any number in deciding how aggressively to treat.
SELF-CHECK
A 19-year-old woman has widespread inflammatory papules and pustules over both cheeks, forehead, and chin, with no nodules or cysts and no scarring, and her calculated GAGS score is 24. How should her acne be graded, and what is the broad treatment implication?
A. Mild — topical therapy alone is sufficient
B. Moderate — typically add an oral agent (e.g. an oral antibiotic) to topical therapy
C. Severe — oral isotretinoin should be started immediately
D. Severe — because any facial involvement automatically qualifies as severe
Reveal Answer
Answer: B. Moderate — typically add an oral agent (e.g. an oral antibiotic) to topical therapy
A GAGS score of 24 falls in the moderate band (19–30). The clinical picture fits this: widespread inflammatory papules and pustules but no nodules, cysts, or scarring, which would be needed to push her into the severe band (GAGS ≥31). Moderate acne is generally not controlled by topical agents alone, so the broad implication is to add an oral agent (commonly a short course of an oral antibiotic, always combined with topical benzoyl peroxide) to topical therapy. Isotretinoin is reserved for severe/nodulocystic or treatment-refractory acne, so starting it immediately here would be premature.
Differential Diagnosis and When to Suspect a Mimic
Acne Vulgaris and Its Mimics: Key Diagnostic Discriminators
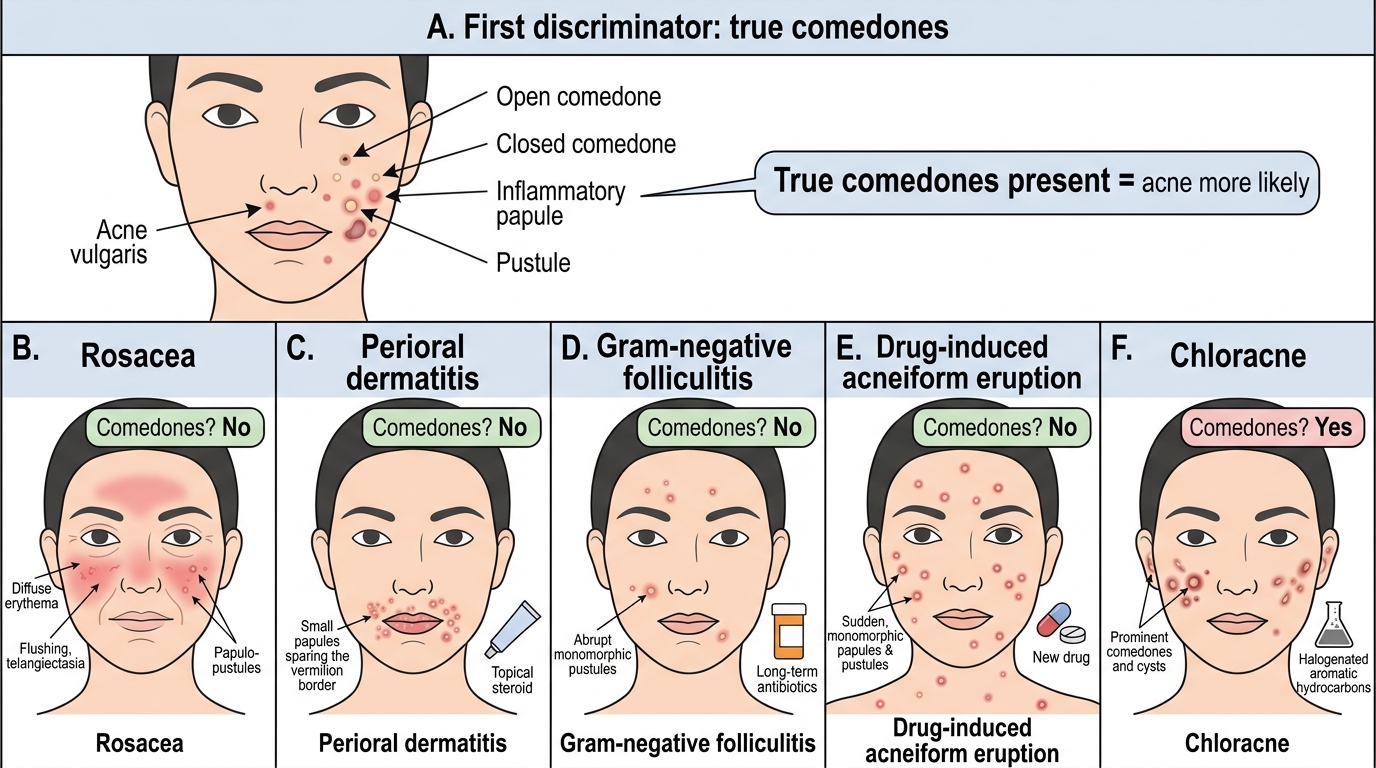
Although acne vulgaris is usually obvious, several conditions mimic it, and recognising acne partly means knowing what it is NOT — the single most useful discriminator is the presence of true comedones, which are the hallmark of acne and absent in most of its mimics. The most important differential is rosacea, which affects the central face of middle-aged adults with persistent erythema, flushing, telangiectasia, and inflammatory papulopustules but characteristically NO comedones; mistaking rosacea for acne leads to the wrong treatment. Perioral dermatitis presents as small grouped papules and pustules around the mouth (sparing the vermilion border), often triggered by topical steroids. Gram-negative folliculitis should be suspected when an acne patient on long-term oral antibiotics suddenly flares with monomorphic pustules. Drug-induced acneiform eruptions are monomorphic (all lesions at the same stage), lack comedones, and appear abruptly after starting a culprit drug. Chloracne from halogenated aromatic hydrocarbon exposure produces comedones and cysts in a characteristic distribution.
A quick comparison helps fix the discriminators:
| Condition | Key distinguishing feature | Comedones present? |
|---|---|---|
| Acne vulgaris | Polymorphic lesions, comedones the hallmark | Yes |
| Rosacea | Central-face erythema, flushing, telangiectasia | No |
| Perioral dermatitis | Papulopustules around mouth sparing lip border | No |
| Drug-induced acneiform | Monomorphic, abrupt onset after a drug | No |
| Chloracne | Comedones/cysts after chemical exposure | Yes |
| Gram-negative folliculitis | Flare of pustules on long-term antibiotics | No |
Whenever the lesions are monomorphic, comedones are absent, or the age and distribution do not fit, pause and reconsider the diagnosis before committing the patient to a long acne treatment course.
Investigations in Acne: Routinely Needed?
Investigations in Acne: When Are They Needed?
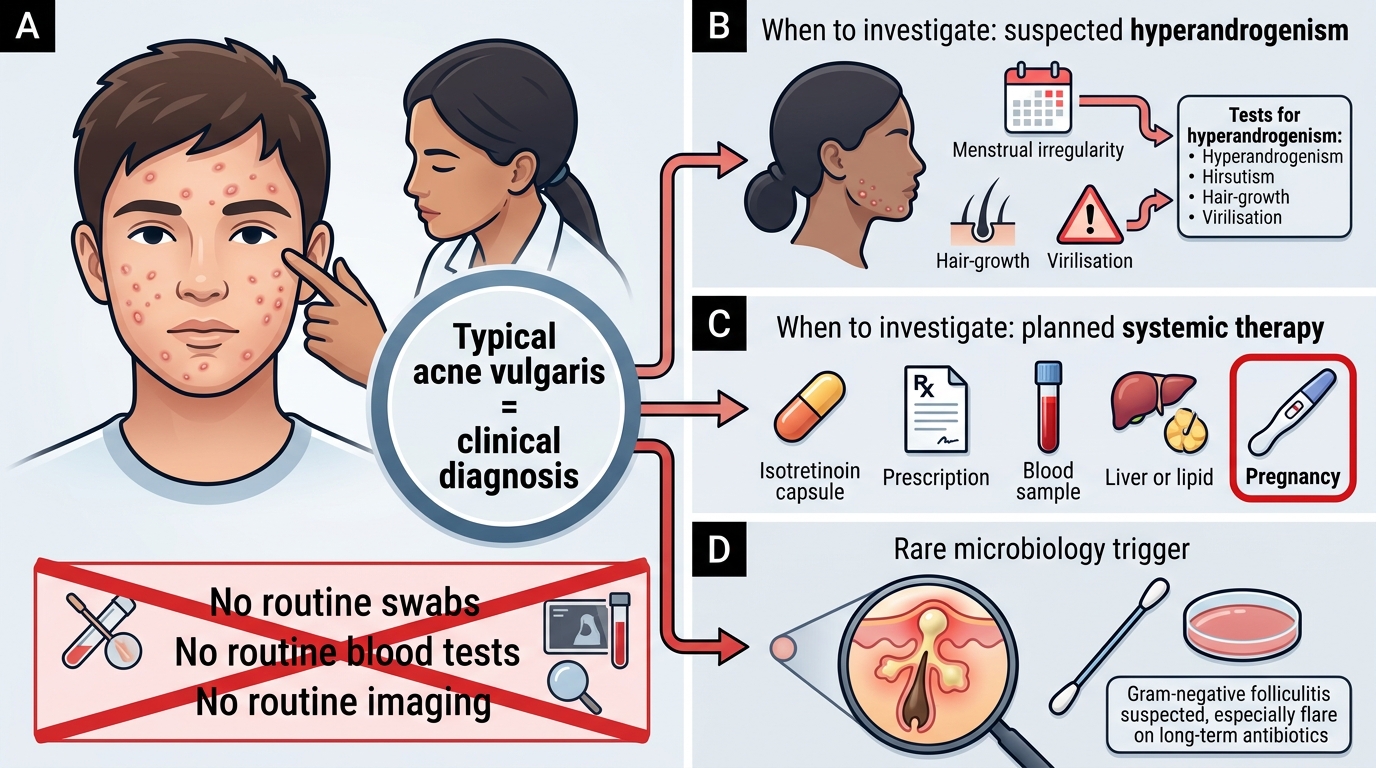
A crucial teaching point is that acne vulgaris is a clinical diagnosis — for the vast majority of patients, no investigation is required at all, and the recognition and grading you have just learnt are entirely sufficient to begin treatment. Ordering routine swabs, blood tests, or imaging in typical adolescent acne is unnecessary, costly, and delays care. Investigations become relevant only in specific situations, and knowing exactly when to investigate is as much a part of competent recognition as the diagnosis itself. The commonest trigger is suspicion of an underlying hyperandrogenic state, particularly in a woman whose acne is sudden, severe, persistent into adulthood, or accompanied by menstrual irregularity, hirsutism, or signs of virilisation. A second trigger is planned systemic therapy, especially isotretinoin, which mandates baseline tests and, critically, a pregnancy test, covered in the management SDL.
The focused investigations to consider, and only when indicated, are:
- Hormonal workup (for suspected hyperandrogenism / PCOS): total and free testosterone, DHEAS, the LH:FSH ratio, prolactin, and pelvic ultrasound — ideally timed in the early follicular phase.
- Microbiological culture (rarely): when gram-negative folliculitis is suspected in a patient flaring on long-term antibiotics, or to exclude a mimic.
- Baseline pre-systemic-therapy bloods: where isotretinoin or hormonal therapy is being planned (detailed in the management SDL).
The take-home message is restraint: investigate the woman with clues of hyperandrogenism and the patient about to start a systemic drug, but do not medicalise straightforward acne with unnecessary tests.
CLINICAL PEARL
The single most useful bedside discriminator in acne is the comedone. If you can find true open or closed comedones, you are almost certainly dealing with acne vulgaris (or chloracne); if there are none, strongly consider a mimic — rosacea, perioral dermatitis, or a drug-induced acneiform eruption. A second pearl: never grade acne by lesion count alone. The presence of even a few nodules, cysts, or early scars moves a patient into the severe category and changes the treatment plan, because these are the lesions that scar permanently. Always examine the chest and back, not just the face — truncal acne is easily missed under clothing and is often more severe than the facial disease that brought the patient in.