Page 7 of 13
DR1.1 | Acne Recognition and Grading — SDL Guide (Part 3)
How Grading Drives Management: The Clinical Link
How Acne Grade Guides Management
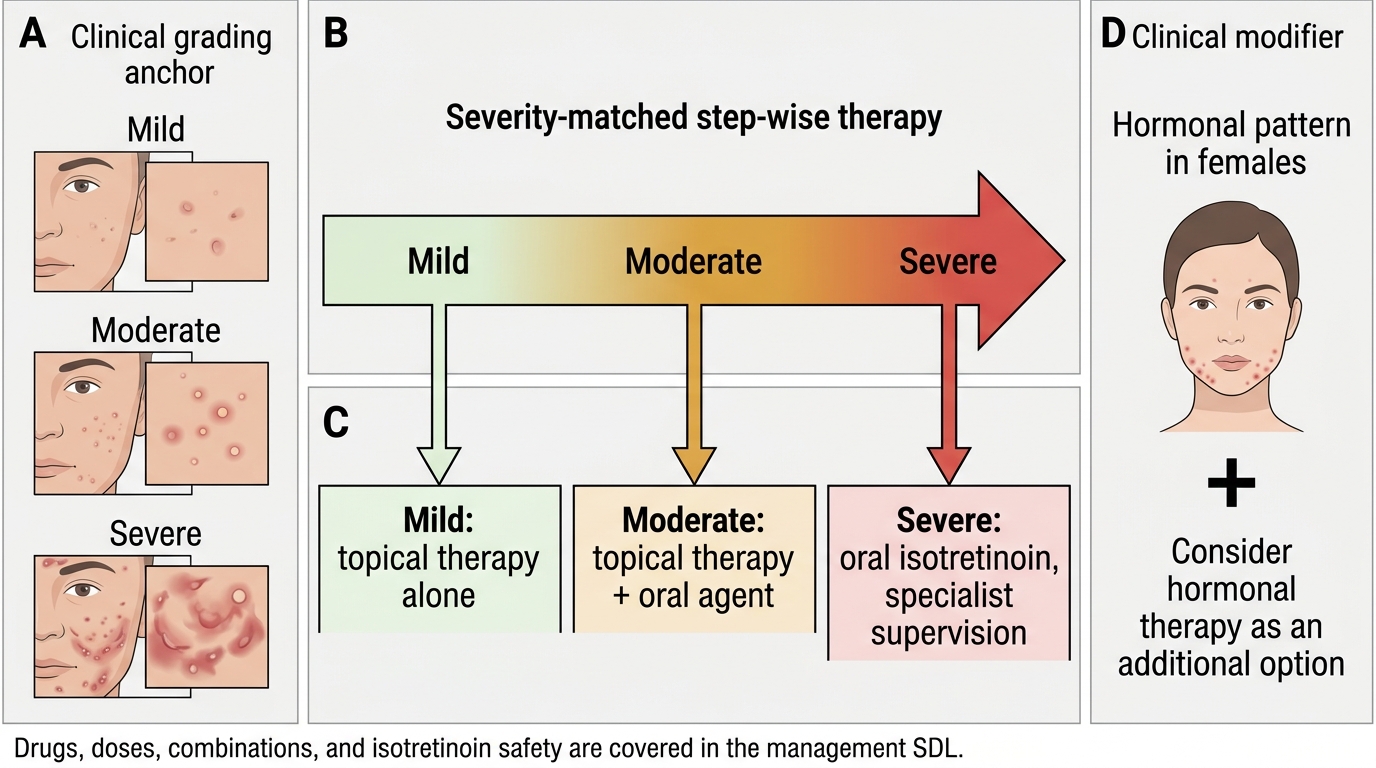
The entire purpose of recognising and grading acne is that the grade hands you the outline of a management plan before you have prescribed a single drug, which is why this recognition SDL and the management SDL that follows are two halves of one skill. The principle running through every guideline is severity-matched, step-wise therapy: the more severe the grade and the greater the scarring risk, the more aggressive and the more systemic the treatment becomes. Mild, predominantly comedonal acne is treated with topical agents alone; moderate inflammatory acne adds an oral agent to those topicals; and severe nodulocystic or treatment-refractory acne, where the risk of permanent scarring is highest, is the territory of oral isotretinoin under specialist supervision. This brief mapping is intentionally kept at the level of principle here — the actual drugs, doses, combinations, and the critical safety issues such as isotretinoin's teratogenicity are developed fully in the management SDL.
The grade-to-management skeleton, to carry into the next SDL, is:
- Mild (mainly comedonal): topical therapy alone.
- Moderate (inflammatory papulopustular): topical therapy PLUS an oral agent.
- Severe (nodulocystic / scarring / refractory): consider oral isotretinoin (specialist).
- Any female with a hormonal pattern: consider hormonal therapy as an additional option.
Seen this way, every minute you spend naming lesions and assigning a grade is repaid immediately as a defensible, guideline-aligned starting point for treatment.
Self-Assessment: Recognising and Grading Acne
Recognising and Grading Acne
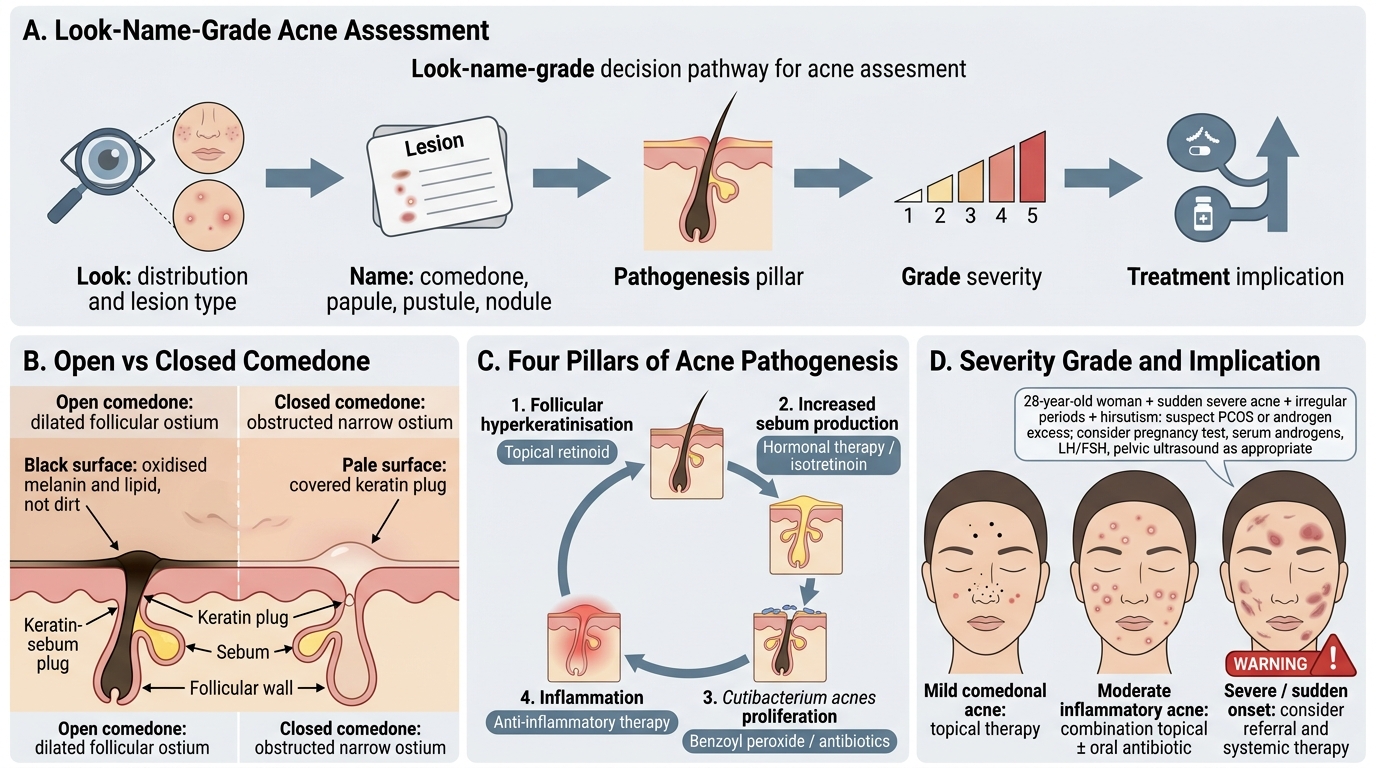
Use the following structured prompts to consolidate what you have learnt about recognising lesion types, applying the pathogenesis framework, and assigning a severity grade. Work through each one actively — describe the lesions in words, name the pathogenetic pillar involved, and commit to a grade with its treatment implication, then check yourself against the principles in this module. The aim is to make the look-name-grade sequence automatic, so that when a real patient sits in front of you, the diagnosis and severity grade form in your mind within the first few seconds of looking at the skin. These self-checks deliberately mirror the kinds of short-answer and case questions you will meet in examinations and in the everyday outpatient department, so treating them as rehearsal will pay off directly in both settings.
- Describe, in your own words, how you would distinguish an open comedone from a closed comedone, and explain why one is black and the other pale.
- List the four pillars of acne pathogenesis in order, and for each name one treatment that targets it.
- For a patient with mainly blackheads and whiteheads over the nose and forehead and only two or three small papules, assign a severity grade and state the broad treatment implication.
- A woman of 28 presents with sudden severe acne, irregular periods, and increased facial hair. What underlying condition would you suspect, and which investigations would you consider?
- Give two clinical features that should make you doubt the diagnosis of acne and consider rosacea instead.