Page 4 of 11
DR6.1 | Pediculosis Diagnosis and Management — SDL Guide
Learning Objectives
- Distinguish the three clinical types of pediculosis — capitis, corporis and pubis — by causative louse, site and morphology.
- Explain the louse life cycle, modes of transmission and the itch mechanism, and recognise the body louse as a vector of epidemic typhus, relapsing fever and trench fever.
- Identify the diagnostic features of each type, including nits on the hair shaft, clothing-seam lice and maculae ceruleae.
- Devise a type-specific management plan for adults and children, selecting the correct pediculicide and stating its adverse effects.
- Apply special-population and community measures, including school advice and partner treatment for pubic lice.
INSTRUCTIONS
Pediculosis is among the commonest ectoparasitic infestations seen in school health checks, crowded living conditions and STD clinics, yet it is frequently mistreated because the three types behave differently. Head lice in a school-age child, body lice in a person living rough (who may also be carrying a life-threatening rickettsial infection), and pubic lice in a sexually active adult each demand a different management plan. This module builds the DR6.1 competency — pathogenesis, diagnostic features and management in adults and children — across the full diagnostic-to-management arc, with the adverse effects and community measures that make a plan workable.
References
- Khanna N. Illustrated Synopsis of Dermatology and Sexually Transmitted Diseases, 6th ed. Ch: Infestations — Pediculosis (textbook)
- Sacchidanand S, et al. IADVL Textbook of Dermatology, 4th ed. Section: Parasitic Infestations — Pediculosis (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 7-year-old girl is sent home from school with an itchy scalp; the teacher has noticed several children in her class scratching. On parting her hair near the nape and behind the ears you see tiny greyish-white oval specks cemented firmly to the hair shafts close to the scalp, and a fast-moving grey insect darts out of sight. Her mother, meanwhile, is embarrassed and asks whether this means the house is 'dirty'. This is pediculosis capitis — head lice — the commonest louse infestation worldwide, spread by head-to-head contact and entirely unrelated to hygiene. The diagnosis is made at the bedside, the treatment is straightforward, and a large part of your job is to manage the family's shame and the school's response correctly.
WHY THIS MATTERS
Pediculosis matters far beyond the itch. Head lice drive enormous anxiety, school absence and unnecessary 'no-nit' exclusions, so a clinician who can diagnose confidently and advise calmly prevents weeks of disruption. Body lice are a different matter entirely: they are the classic vector of three serious infections — epidemic typhus, louse-borne relapsing fever and trench fever — and tend to occur in exactly the vulnerable populations (homeless people, refugees, those in overcrowded conditions) where these diseases re-emerge, so recognising body lice can be the clue that prevents an outbreak. Pubic lice are a sexually transmitted infestation, mandating partner treatment and a wider STI screen, and their appearance on a child's eyelashes raises the possibility of sexual abuse. Getting the type right therefore changes not just the prescription but the whole plan.
RECALL
Recall a few foundations before building the management plan. From zoology/parasitology, lice are six-legged insects (order Phthiraptera) — distinguish them from the eight-legged scabies mite — and they are obligate blood-feeding ectoparasites that die within a day or two off the host. From anatomy, the hair shaft is the structure to which the louse cements its egg (the nit) with a sleeve of chitinous 'glue', which is why nits cannot simply be brushed off like dandruff. From pharmacology, permethrin (a pyrethroid) acts on insect sodium channels, while malathion is an organophosphate that inhibits the louse's acetylcholinesterase — the same two mechanisms you met for scabicides, here repurposed against lice. Finally, recall from microbiology that Rickettsia prowazekii, Borrelia recurrentis and Bartonella quintana are the organisms the body louse transmits.
Clinical Presentation of Pediculosis: Types and Morphological Features
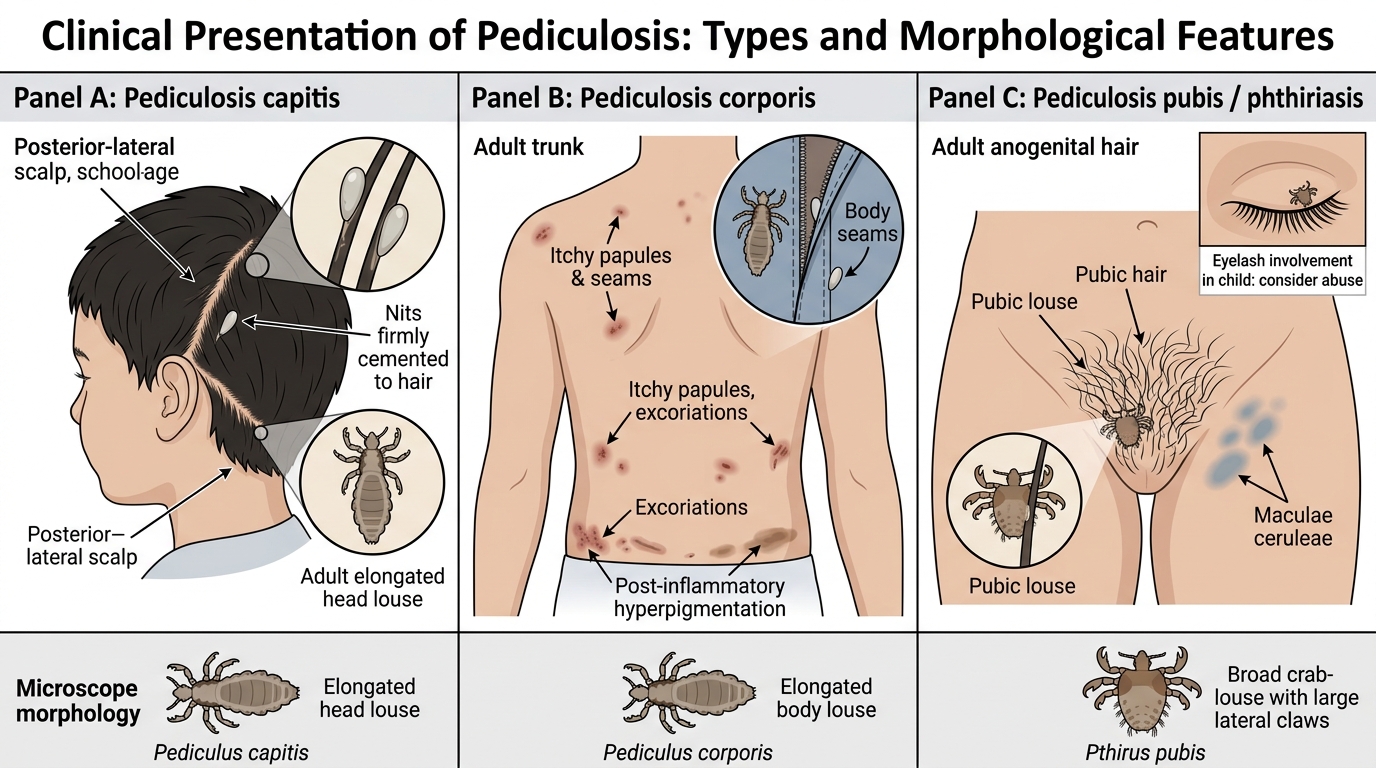
Clinical Types and Morphology of Pediculosis
Pediculosis presents in three clinically distinct forms defined by the causative louse and the body site it infests, and recognising which type you are dealing with is the first and most important diagnostic step. Pediculosis capitis, caused by the head louse, presents with scalp itch and greyish-white nits cemented to hair shafts, especially behind the ears and at the nape, and is overwhelmingly a disease of school-age children. Pediculosis corporis, caused by the body louse, presents with intensely itchy excoriations, papules and post-inflammatory pigmentation on the trunk; crucially the lice and their eggs live and are found in the seams of clothing rather than on the skin, so a clinician who looks only at the skin will miss the diagnosis — it occurs in people living in poverty, overcrowding or without regular changes of clothing. Pediculosis pubis (phthiriasis), caused by the broad, crab-shaped pubic louse, presents with itch in the anogenital hair and sometimes bluish-grey macules (maculae ceruleae); because it is sexually transmitted it occurs in sexually active adults, and eyelash involvement in a child should prompt consideration of sexual abuse. The morphology of the three lice differs too, which helps confirmation under the microscope.
Comparison of Pediculosis Types
- Capitis (head louse): scalp itch, nits on hair shafts (nape, behind ears); school-age children
- Corporis (body louse): trunk excoriations; lice/nits in CLOTHING SEAMS, not on skin; poverty/overcrowding
- Pubis (crab louse): anogenital itch, maculae ceruleae; sexually transmitted adults; eyelashes in children → suspect abuse
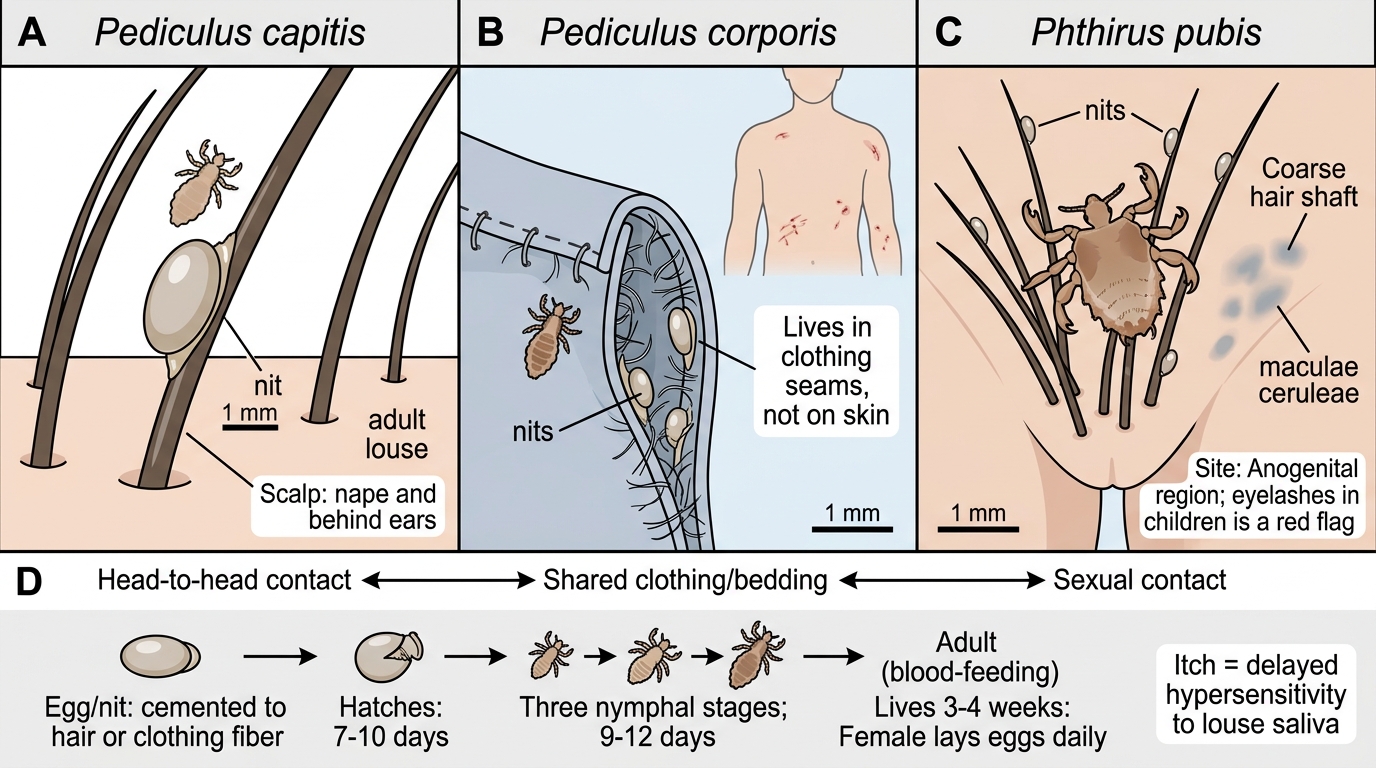
Pathogenesis of Pediculosis: Life Cycle, Transmission, and Itch Mechanism
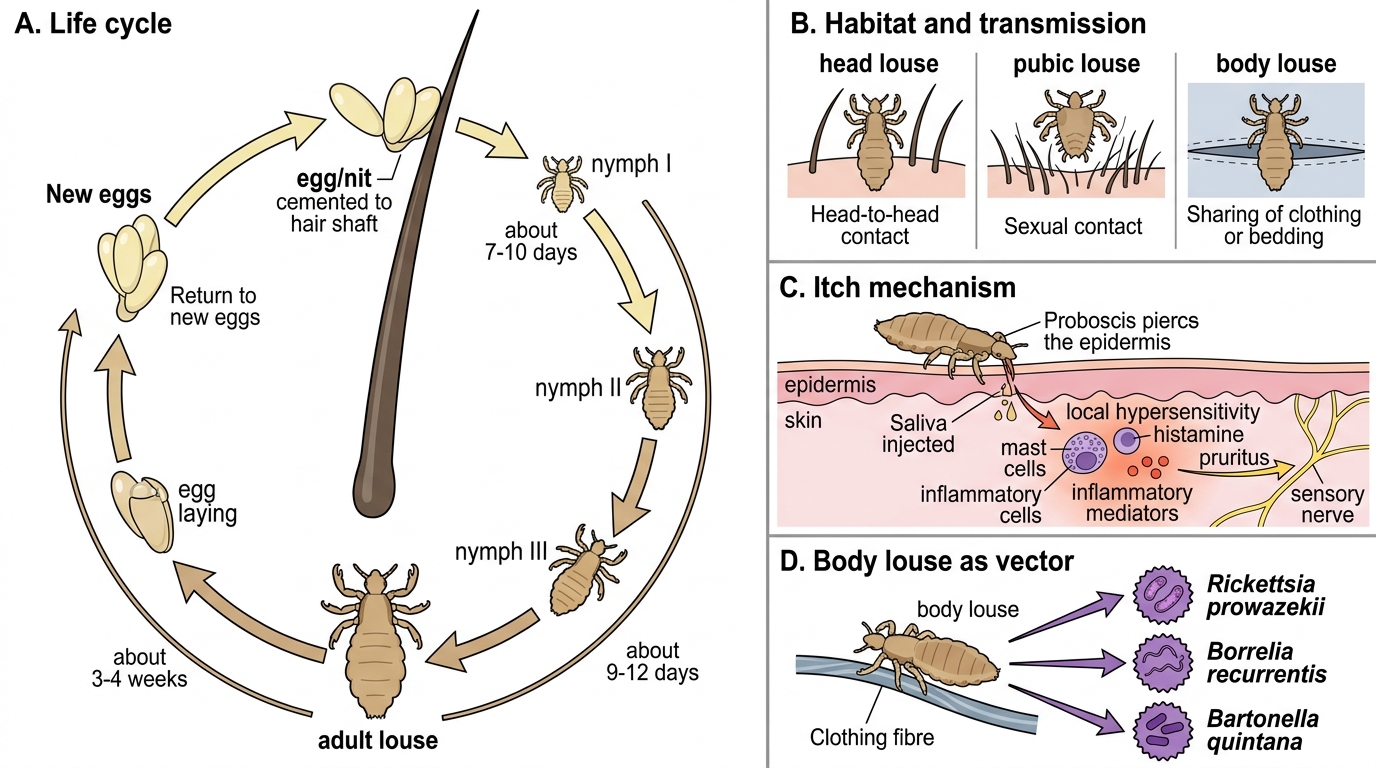
Pediculosis: Life Cycle, Transmission, Itch, and Vector Risk
All three lice share a broadly similar life cycle but differ critically in where they live and what they transmit. The female cements her eggs (nits) to hair shafts (capitis, pubis) or to clothing fibres (corporis); the egg hatches in about 7 to 10 days into a nymph, which matures through three nymphal stages into a blood-feeding adult over a further 9 to 12 days, and the adult then lives for around three to four weeks, the female laying several eggs a day. Transmission of head and pubic lice is by direct contact — head-to-head play among children for capitis, sexual contact for pubis — whereas the body louse, living in clothing, also spreads readily by sharing of contaminated clothing and bedding. The itch in all forms is a hypersensitivity reaction to louse saliva injected during feeding, so as with scabies it may take time to develop in a first infestation. The unique and clinically vital feature of the body louse is that it is a disease vector: it transmits Rickettsia prowazekii (epidemic typhus), Borrelia recurrentis (louse-borne relapsing fever) and Bartonella quintana (trench fever) — head and pubic lice do not transmit these.
Life Cycle of Pediculus humanus capitis
- Egg (nit) → nymph (~7-10 days) → adult (~9-12 days more); adult lives ~3-4 weeks
- Capitis: head-to-head contact; Pubis: sexual contact; Corporis: clothing/bedding sharing
- Itch = hypersensitivity to louse saliva
- Body louse ONLY = vector for epidemic typhus (R. prowazekii), relapsing fever (B. recurrentis), trench fever (B. quintana)
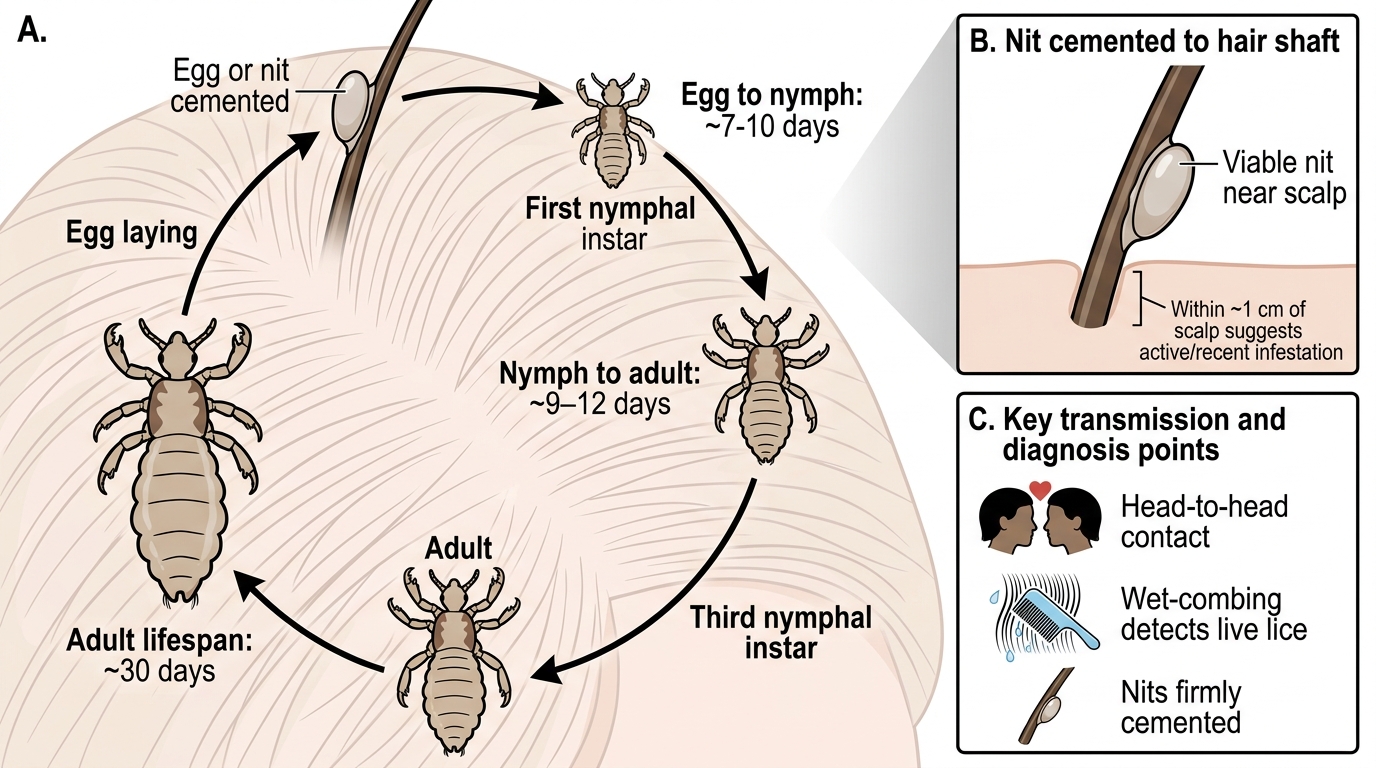
Clinical Features and Diagnosis
Clinical Features and Diagnosis of Pediculosis
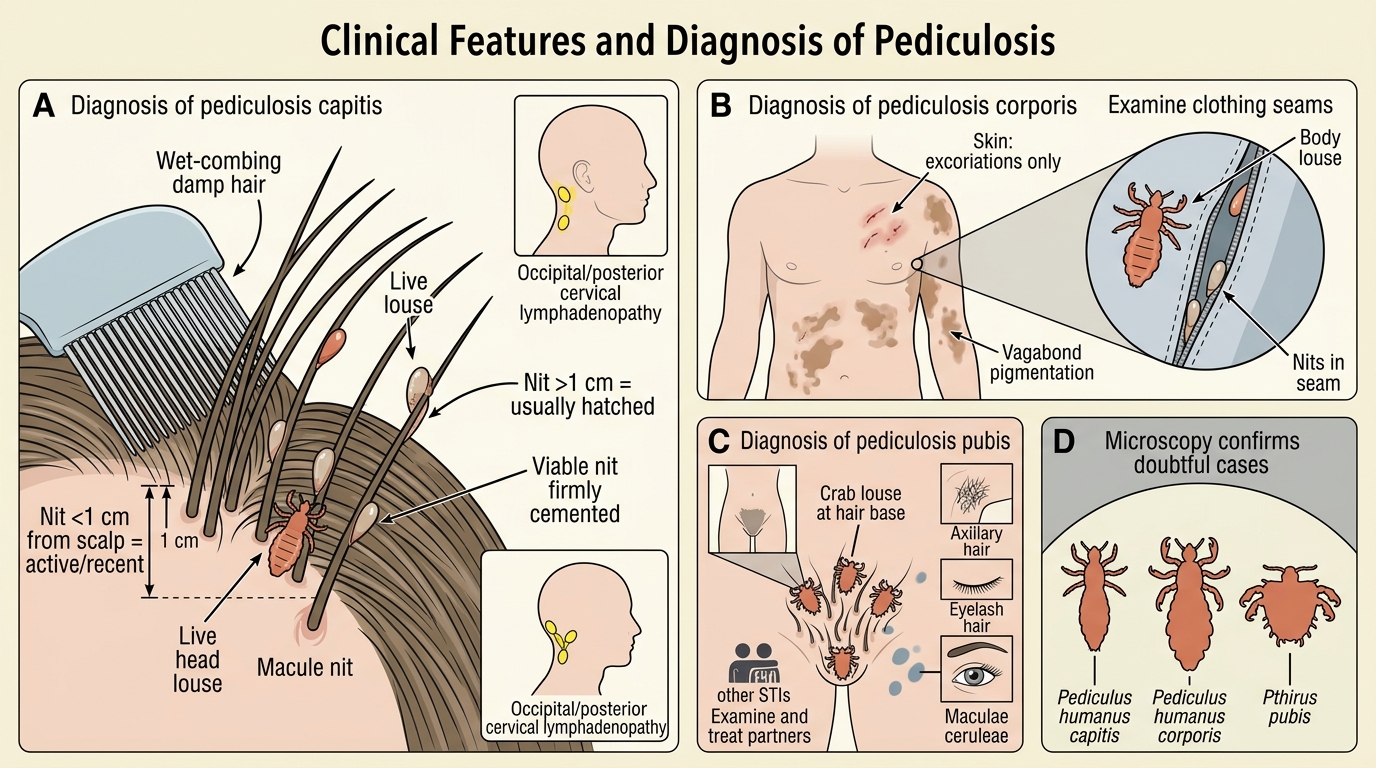
Diagnosis of pediculosis is made by directly demonstrating lice or viable nits, and the approach differs by type. In capitis, the diagnosis is confirmed by finding live lice — best done by wet-combing damp, conditioned hair with a fine-toothed louse comb — and by seeing nits firmly cemented to hair shafts; the position of the nit matters, because nits within about 1 cm of the scalp indicate active or recent infestation whereas nits more than 1 cm out have usually already hatched, and occipital or posterior cervical lymphadenopathy is a useful supportive sign. In corporis, the skin shows only the secondary changes (excoriations, the 'vagabond's' hyperpigmentation), so diagnosis depends on examining the seams of the patient's clothing, where the lice and nits are found. In pubis, look for crab lice clinging at the base of pubic, perianal, axillary or even eyelash hairs, together with maculae ceruleae; because it is an STI, diagnosis should trigger screening for other sexually transmitted infections and examination and treatment of partners. Microscopy distinguishes the three lice morphologically and confirms a doubtful case.
- Capitis: wet-combing for live lice; nits <1 cm from scalp = active; occipital lymphadenopathy
- Corporis: examine CLOTHING SEAMS (skin shows only excoriations / vagabond's pigmentation)
- Pubis: crab lice at hair bases (pubic, axillary, eyelash); maculae ceruleae; screen for other STIs + treat partner
- Microscopy: confirms species and distinguishes from hair casts/dandruff (nits are cemented, do not slide)
SELF-CHECK
A man brought from a homeless shelter has intensely itchy excoriations and hyperpigmentation over his trunk, but careful examination of the skin reveals no lice or nits. What is the diagnosis and where should you look to confirm it?
A. Pediculosis capitis; examine the scalp hair
B. Pediculosis corporis; examine the seams of his clothing, where the lice and nits live — and be alert that the body louse can transmit epidemic typhus and relapsing fever
C. Scabies; take a skin scraping from a burrow
D. Atopic dermatitis; no parasite to find
Reveal Answer
Answer: B. Pediculosis corporis; examine the seams of his clothing, where the lice and nits live — and be alert that the body louse can transmit epidemic typhus and relapsing fever
Body lice (pediculosis corporis) live and lay eggs in clothing seams, not on the skin, so the skin shows only secondary excoriations and 'vagabond's' pigmentation. Confirmation comes from examining the clothing. Importantly, the body louse is the vector for epidemic typhus, louse-borne relapsing fever and trench fever, which must be considered in this population.