Page 5 of 11
DR6.1 | Pediculosis Diagnosis and Management — SDL Guide (Part 2)
Differential Diagnosis and Investigations
Differential Diagnosis and Investigations in Pediculosis
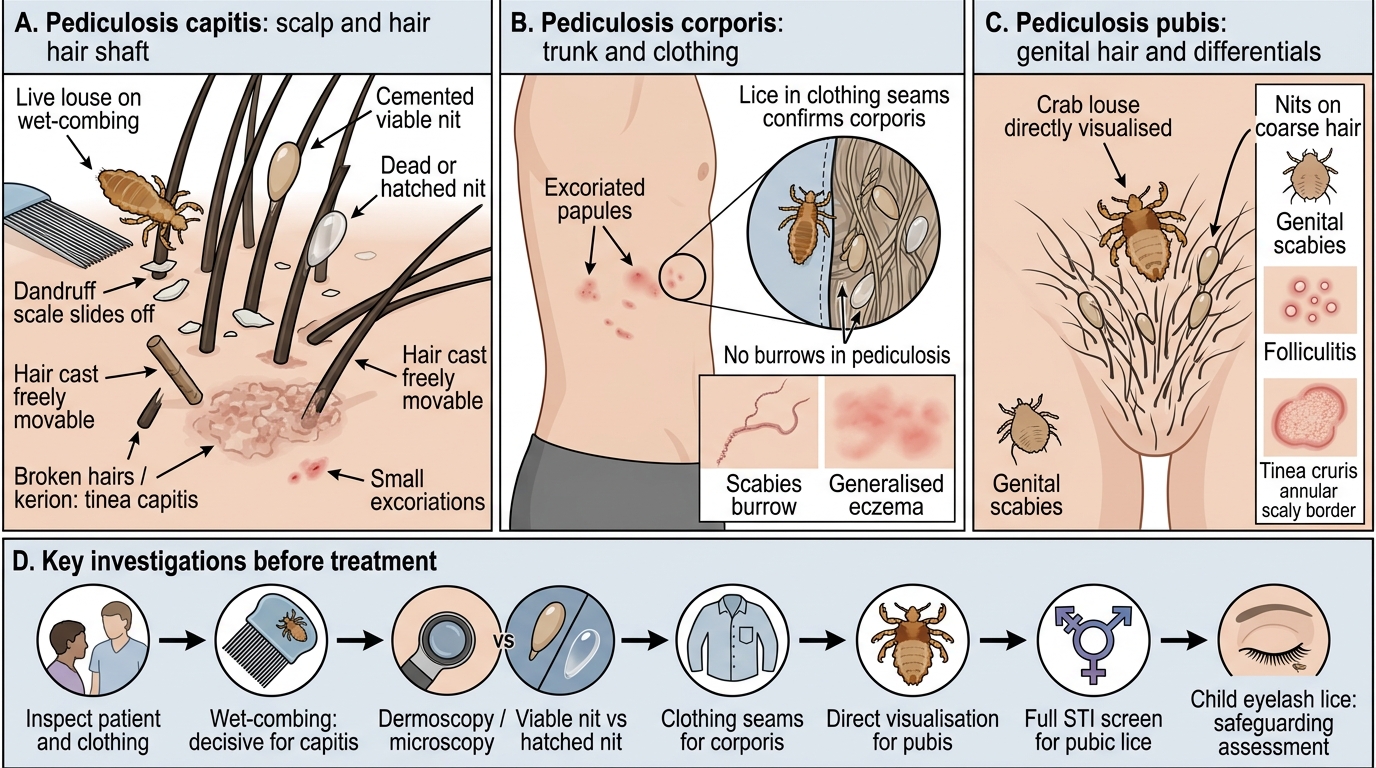
Before treating, exclude the conditions that mimic each type of pediculosis, because the management differs. For capitis, the chief differentials are seborrhoeic dermatitis and dandruff (scales slide off the hair, unlike cemented nits), hair casts (freely movable keratin cylinders), tinea capitis (scaling, broken hairs, sometimes a boggy kerion), and simple excoriation; the decisive test is finding a live louse on wet-combing, since dead nits alone may persist after past infestation and do not warrant treatment. For corporis, scabies and generalised eczema must be considered, distinguished by the absence of burrows and by finding lice in clothing. For pubis, the differentials include scabies of the genital area, folliculitis and tinea cruris, separated by direct visualisation of the crab louse. The key investigations are therefore bedside and microscopic: wet-combing and dermoscopy/microscopy to demonstrate the louse and to distinguish viable from hatched nits. For pubic lice, the most important 'investigation' is a full sexual-health work-up — because the diagnosis is itself a marker of an STI — and, in a child with eyelash infestation, a safeguarding assessment.
- Capitis differentials: dandruff/seborrhoeic dermatitis (scales slide), hair casts (movable), tinea capitis (broken hairs, kerion)
- Corporis differentials: scabies (burrows), eczema — confirm by lice in clothing
- Pubis differentials: genital scabies, folliculitis, tinea cruris — confirm by seeing crab louse
- Investigations: wet-combing, dermoscopy/microscopy (viable vs hatched nit); for pubis → full STI screen + partner; child eyelash infestation → safeguarding
Management of Pediculosis: Pediculicides, ADRs, Special Populations, and School/Community Measures
Management of Pediculosis
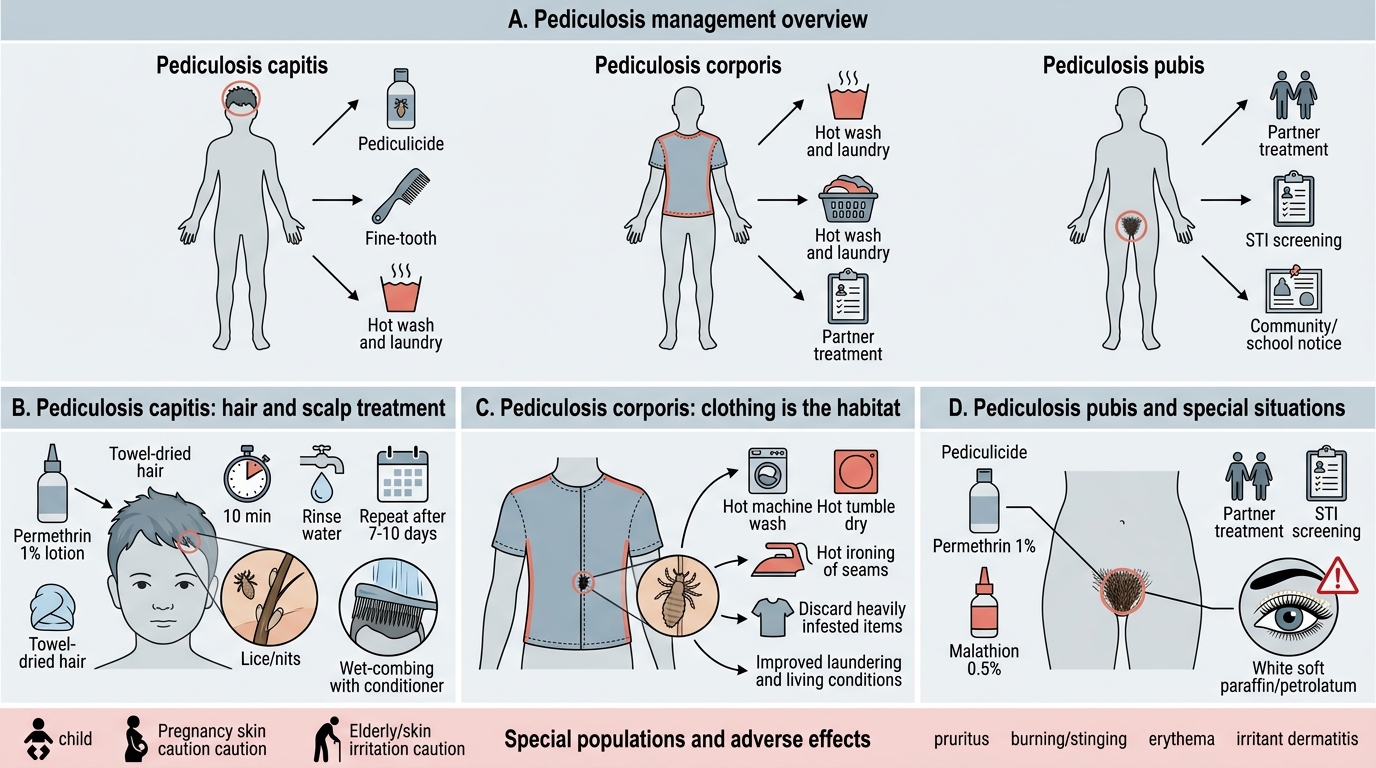
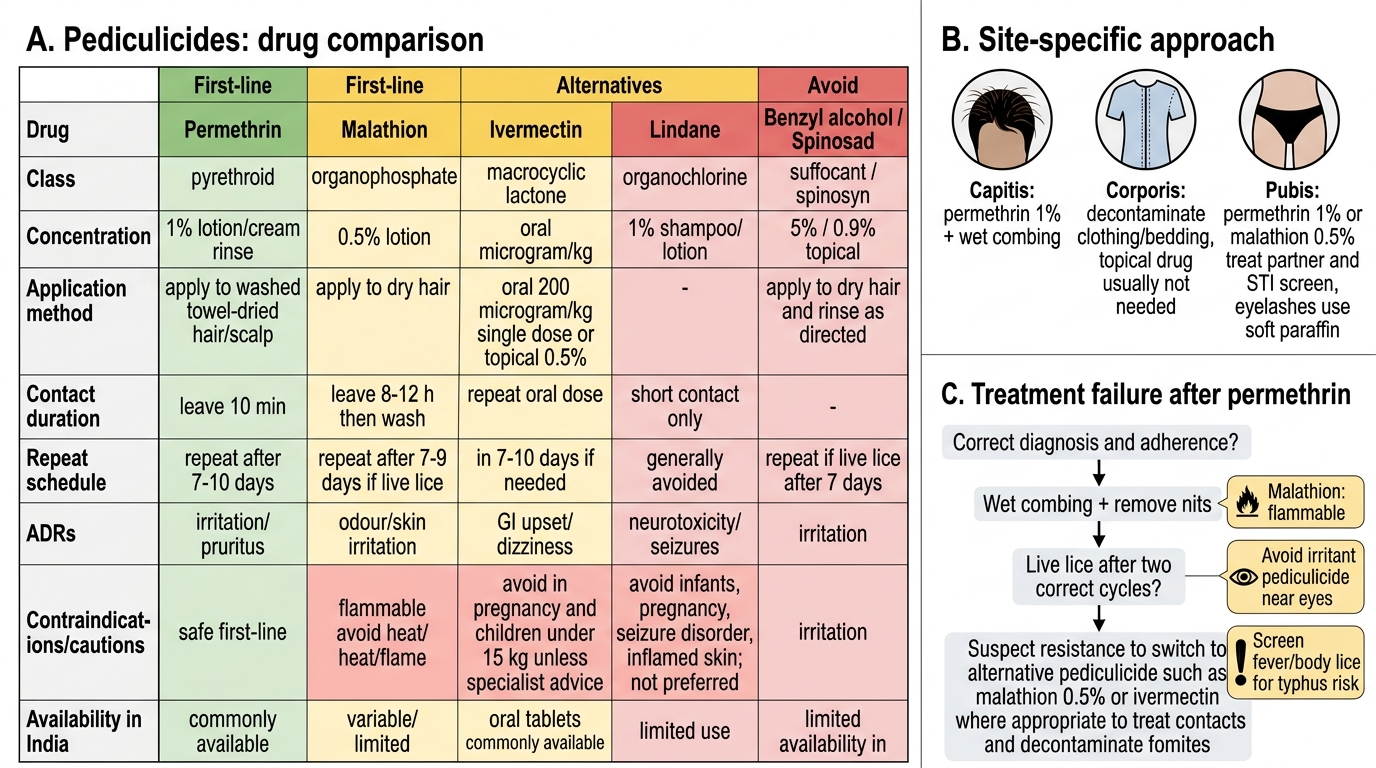
Management is type-specific, and a complete plan combines the correct pediculicide, mechanical measures, treatment of contacts or partners, and appropriate community advice. For pediculosis capitis, first-line treatment is permethrin 1% lotion or cream rinse, applied to towel-dried hair, left for about 10 minutes and rinsed off, then repeated after 7 to 10 days to kill lice hatching from surviving eggs; malathion 0.5% lotion is the principal second-line agent, used where there is permethrin resistance, and wet-combing with conditioner is a useful adjunct and the preferred approach in very young children. Oral or topical ivermectin is reserved for resistant or extensive cases. For pediculosis corporis, the louse lives in clothing, so the cornerstone of treatment is decontaminating clothing and bedding by hot machine-washing, hot tumble-drying or hot ironing of seams (or discarding heavily infested items); topical pediculicides to the body are usually unnecessary, and improving the patient's living and laundering conditions is essential. For pediculosis pubis, apply permethrin 1% or malathion 0.5% to the affected areas, treat all sexual partners, screen for other STIs, and manage eyelash involvement with white soft paraffin (petrolatum) applied to smother the lice rather than an irritant pediculicide near the eye. In children, prefer permethrin and wet-combing, observe age and weight cautions for systemic agents, and follow current guidance that the child may return to school after the first treatment — routine 'no-nit' exclusion is no longer recommended. The adverse effects to counsel on are: permethrin — scalp/skin irritation, itching and occasional contact dermatitis; malathion — local irritation, an unpleasant odour, and importantly it is flammable (keep away from flames/hairdryers) with a theoretical organophosphate toxicity risk if misused, so it is used cautiously in young children; ivermectin — caution in children under 15 kg and in pregnancy.
Pediculicides: Drug Comparison and Clinical Use
| Type | First-line | Key adjuncts / measures | ADRs / cautions |
|---|---|---|---|
| Capitis | Permethrin 1% (repeat in 7-10 d) | Wet-combing; malathion 0.5% if resistant | Permethrin irritation; malathion flammable, odour |
| Corporis | Decontaminate clothing/bedding (hot wash/iron seams) | Improve laundering/living conditions | Topical usually not needed; treat any typhus/fever |
| Pubis | Permethrin 1% or malathion 0.5% | Treat partner, STI screen; eyelashes → soft paraffin | Avoid irritant pediculicide near eye |
SELF-CHECK
A 7-year-old child with pediculosis capitis was treated correctly with permethrin 1%, but live lice persist after two cycles. What is the most appropriate next step?
A. Repeat the same permethrin a third time at the same concentration
B. Switch to a second-line agent such as malathion 0.5% lotion (suspecting permethrin resistance), continue wet-combing, and recheck for re-infestation from untreated contacts
C. Start a potent topical corticosteroid
D. Exclude the child from school until every nit has gone
Reveal Answer
Answer: B. Switch to a second-line agent such as malathion 0.5% lotion (suspecting permethrin resistance), continue wet-combing, and recheck for re-infestation from untreated contacts
Persistent live lice after correctly applied permethrin suggests permethrin resistance (well documented) or re-infestation. The rational next step is a second-line pediculicide such as malathion 0.5%, plus mechanical wet-combing and a check of close contacts. Steroids do not treat lice, and prolonged 'no-nit' school exclusion is no longer recommended; the child can attend after the first effective treatment.
Self-Assessment: Pediculosis Case Scenarios
Pediculosis Case Scenarios: Diagnosis and Management
Work through these scenarios to confirm that you can identify the type of pediculosis and devise a complete, type-appropriate management plan, including the pediculicide, its adverse effects, and the community or partner measures each type demands. For each case, before reading any answer, decide which louse is responsible, which body site and which population fits, what the first-line treatment is, and what extra step beyond the prescription the case requires — school advice, clothing decontamination, partner treatment or a safeguarding question. These extra steps are exactly what distinguishes a safe plan from a bare prescription and are precisely what an examiner is testing when they give you a scenario rather than a single fact. Remember that the body-louse case carries the additional duty of considering louse-borne febrile illness, and that the pubic-louse case is never complete without addressing the partner and screening for other sexually transmitted infections.
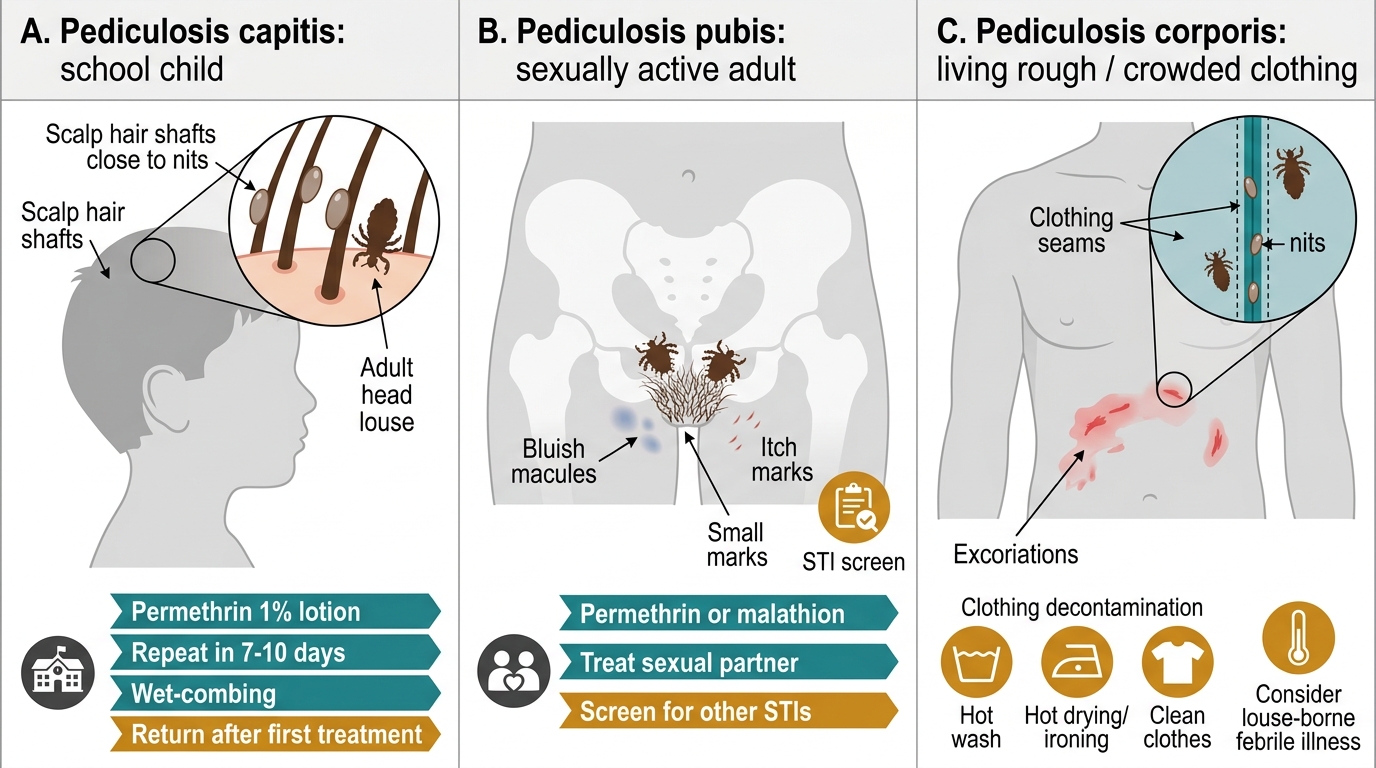
- Scenario 1 — School child with scalp itch and nits near the scalp: diagnose capitis, prescribe permethrin 1% with repeat in 7-10 days, advise wet-combing, reassure it is not about hygiene, allow return to school after first treatment.
- Scenario 2 — Sexually active adult with groin itch and bluish macules: diagnose pubis, treat with permethrin/malathion, treat the partner, screen for other STIs.
- Scenario 3 — Person living rough with excoriated trunk and no skin lice: diagnose corporis, decontaminate clothing/bedding, improve laundering, and actively consider epidemic typhus / relapsing fever if febrile.
CLINICAL PEARL
Two pediculosis facts change management dramatically. First, in pediculosis corporis the lice live in the clothing, not on the skin — so 'no parasite on the body' does not exclude it; examine the seams, and never forget that the body louse can carry epidemic typhus, relapsing fever and trench fever in vulnerable populations. Second, finding pubic lice on a child's eyelashes, or pubic lice in any patient, is a sexually-transmitted-infection event: treat the partner, screen for other STIs, and in a child consider safeguarding. Treat the situation, not just the scalp.