Page 1 of 20
DR12.1-2 | Eczema Recognition and Basic Treatment — SDL Guide
Learning Objectives
- Identify common types of eczema (endogenous and exogenous) from clinical features and history.
- Distinguish acute from chronic eczema morphology and recognise the typical distribution of each endogenous type.
- Differentiate irritant from allergic contact dermatitis and state the role of patch testing.
- Outline the stepwise treatment of eczema: emollients, topical corticosteroids by potency, topical calcineurin inhibitors, and when systemic therapy is needed.
- Apply site-specific rules for topical corticosteroid potency to avoid harm on the face and flexures.
INSTRUCTIONS
Eczema (dermatitis) is the single most common reason a patient walks into a skin clinic or a general practice in India with an itchy rash, and it is one of the conditions a primary-care physician is expected to recognise and treat without referral. This module builds your ability to look at an itchy, red, scaly or oozing eruption and name the kind of eczema it is, then choose safe first-line treatment. Getting the type right matters because the management of an allergic contact dermatitis (find and avoid the allergen) differs from atopic eczema (long-term barrier repair) — and because misuse of potent topical steroids on the face is a widespread, harmful problem in India.
References
- Khanna N. Illustrated Synopsis of Dermatology and Sexually Transmitted Diseases, 6th ed. Ch: Eczema/Dermatitis (textbook)
- Sacchidanand S, et al. IADVL Textbook of Dermatology, 4th ed. Section: Eczema and Contact Dermatitis (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 28-year-old tailor comes to your clinic with itchy, red, cracked skin over both hands that has troubled him for three months. It improves on Sundays and flares within a day of returning to work. His mother says he had a similar weepy rash in the folds of his elbows as a child. In the same waiting room sits a 65-year-old man whose lower legs are dry, scaly and fissured like cracked porcelain, worse since winter began. Both have eczema — but of completely different types, with completely different causes and treatments. The skill you build in this module is the one that separates these two patients at a glance: recognising the kind of eczema in front of you, and matching it to the right first-line care.
WHY THIS MATTERS
Eczema accounts for a large share of every dermatology and primary-care outpatient load in India, and most cases never need a specialist if the first doctor recognises the type and treats it correctly. Mislabelling eczema as a fungal infection (and prescribing the wrong cream), or reaching reflexively for a potent steroid on a child's face, are everyday errors that prolong suffering and cause harm such as skin atrophy and steroid-induced rosacea. As a future physician you will be the first point of contact for these patients, and your ability to distinguish endogenous from exogenous eczema, acute from chronic, and to apply the topical steroid potency ladder safely, is a core clinical competence (DR12.1 and DR12.2).
RECALL
Before we begin, recall three things you already know. First, from anatomy: the epidermis is capped by the stratum corneum, a brick-and-mortar barrier of corneocytes and intercellular lipids that keeps water in and irritants out. Second, from physiology and immunology: type IV hypersensitivity is a delayed, T-cell-mediated reaction that needs a prior sensitisation phase before it can be elicited on re-exposure — this is the mechanism of allergic contact dermatitis. Third, atopy is the inherited tendency to produce IgE against common environmental antigens, linking eczema, asthma and allergic rhinitis in the same patient or family. Eczema, at its core, is what happens when this barrier fails and the immune system over-reacts.
How Eczema Presents: Morphology and Phases
Morphological Phases of Eczema
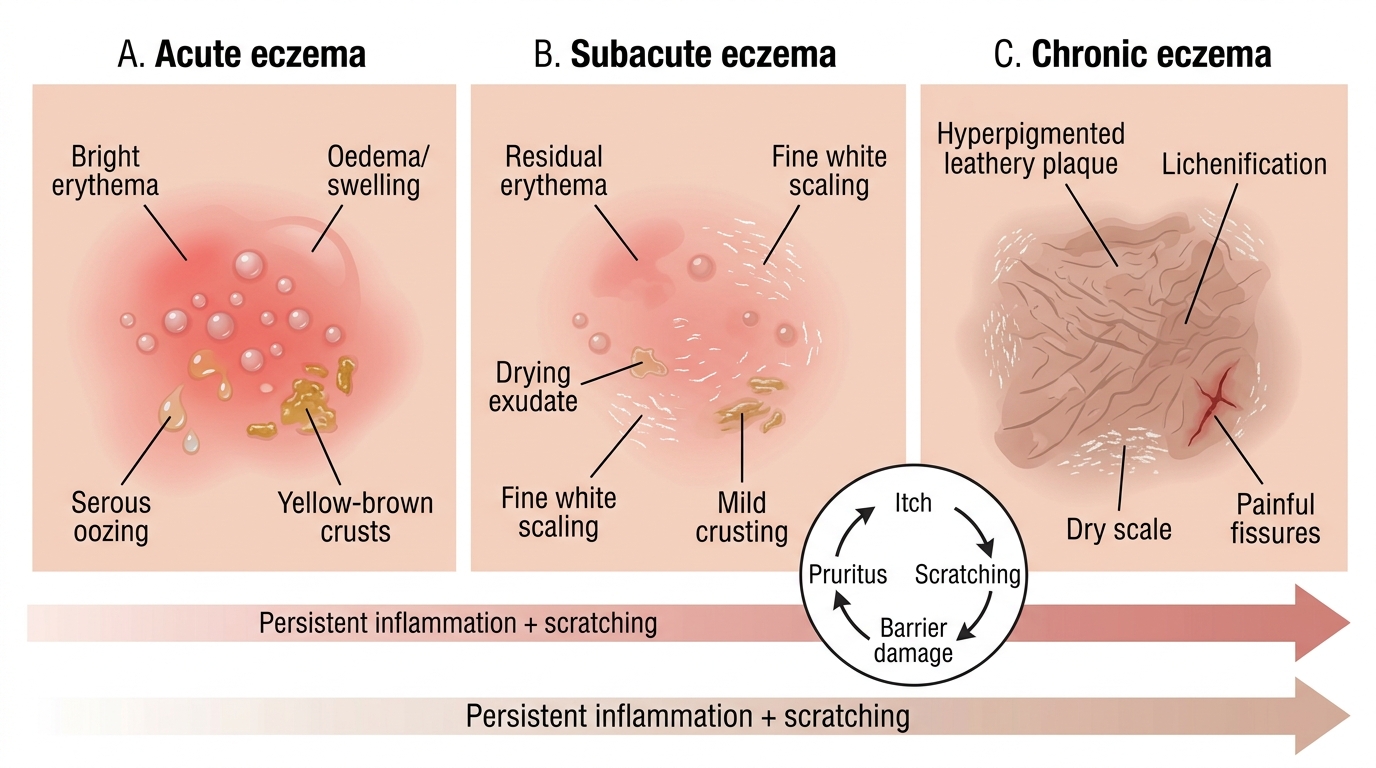
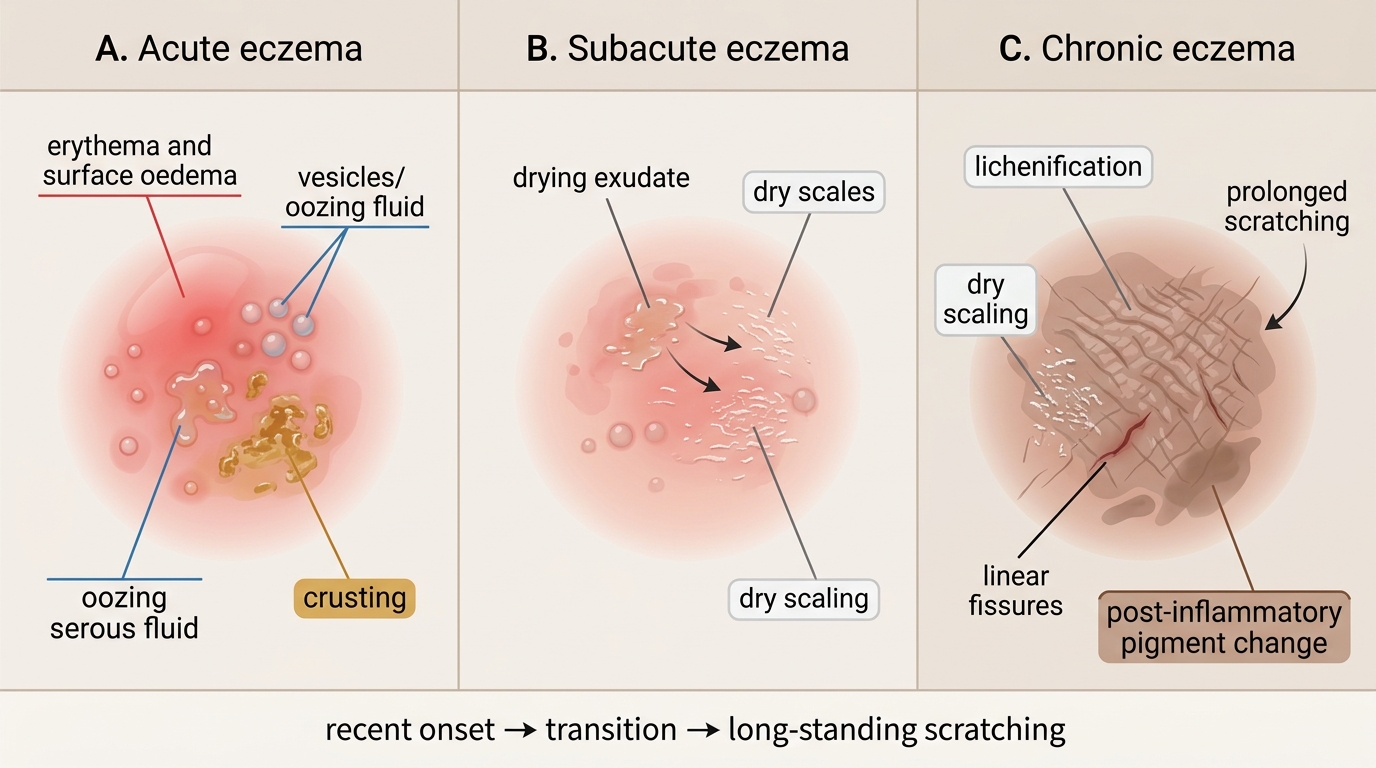
Eczema is not one appearance but a sequence, and recognising which phase you are looking at is the first diagnostic step. In the acute phase the skin is intensely red, swollen and studded with tiny vesicles that weep clear fluid and crust over — the picture of a fresh allergic reaction or a flare. If the inflammation persists for weeks, it passes through a subacute phase and finally becomes chronic, where repeated scratching thickens the skin into leathery plaques with exaggerated skin markings, a change called lichenification, often with scaling and painful fissures. The unifying clinical clue across all phases is itch (pruritus): eczema is, above all, an itchy condition, and the scratching itself drives the chronic changes in a self-perpetuating itch-scratch cycle.
Learning to read the phase tells you both the likely cause and the treatment intensity. Acute, oozing eczema points towards a recent contact or an acute flare and needs drying, soothing measures; chronic lichenified eczema points to a long-standing endogenous process and needs sustained emollient and potency-matched steroid therapy.
Morphological Stages of Eczema
- Acute: erythema, oedema, vesicles, oozing, crusting — typically intensely itchy and recent in onset.
- Subacute: drying exudate, scaling, less vesiculation — the transition stage.
- Chronic: lichenification, scaling, fissuring, post-inflammatory pigment change — the result of prolonged scratching.
Why the Skin Breaks Down: Pathogenesis of Eczema
Pathogenesis of Eczema: Barrier Failure, Irritation, and Hypersensitivity
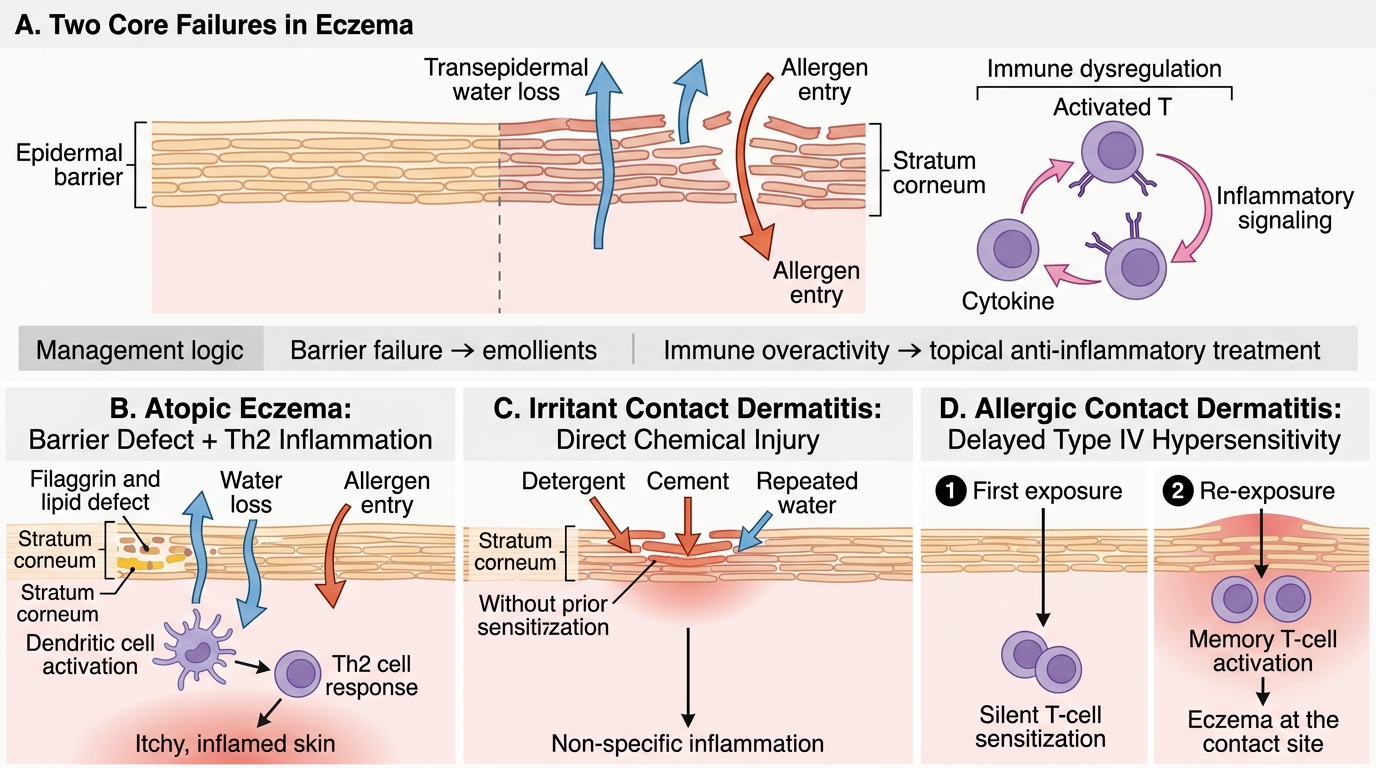
Eczema arises from the interaction of two failures: a defective skin barrier and a dysregulated immune response, but the balance between them differs by type. In atopic eczema, an inherited barrier weakness — classically loss-of-function mutations in the filaggrin gene — lets water escape and allergens enter, triggering a T-helper-2 (Th2) dominated inflammation that produces the chronic itchy disease. In irritant contact dermatitis, there is no prior immune sensitisation at all; a chemical (detergent, cement, repeated water exposure) directly damages the stratum corneum and provokes inflammation in anyone exposed enough. In allergic contact dermatitis, the mechanism is a true delayed type IV hypersensitivity: the first contact sensitises the patient's T cells silently, and only on a later re-exposure does eczema erupt at the contact site.
Understanding which mechanism dominates explains the whole management logic that follows. Barrier failure is why emollients are the foundation of every eczema regimen; immune over-activity is why topical anti-inflammatories (corticosteroids and calcineurin inhibitors) are layered on top; and the sensitisation mechanism of allergic contact dermatitis is why finding and avoiding the culprit allergen can be curative where creams alone are not.
- Barrier failure (filaggrin/lipid defect) → water loss + allergen entry → underlies atopic and asteatotic eczema.
- Direct chemical injury (no immunity needed) → irritant contact dermatitis.
- Type IV delayed hypersensitivity (needs prior sensitisation) → allergic contact dermatitis.
SELF-CHECK
A man develops hand eczema only after starting a new job handling cement, and the rash affects everyone in his work section who handles it without gloves. Which mechanism best explains this?
A. Type IV (delayed) hypersensitivity requiring prior sensitisation
B. Direct irritant injury to the skin barrier, no prior sensitisation needed
C. IgE-mediated immediate hypersensitivity
D. Filaggrin gene mutation causing atopic eczema
Reveal Answer
Answer: B. Direct irritant injury to the skin barrier, no prior sensitisation needed
The rash affecting most exposed workers, in proportion to exposure and without needing prior sensitisation, is characteristic of IRRITANT contact dermatitis — direct toxic damage to the barrier. Allergic contact dermatitis (type IV) would affect only previously sensitised individuals, not everyone exposed.
Recognising Endogenous Eczema Types
Distribution Patterns of Endogenous Eczemas
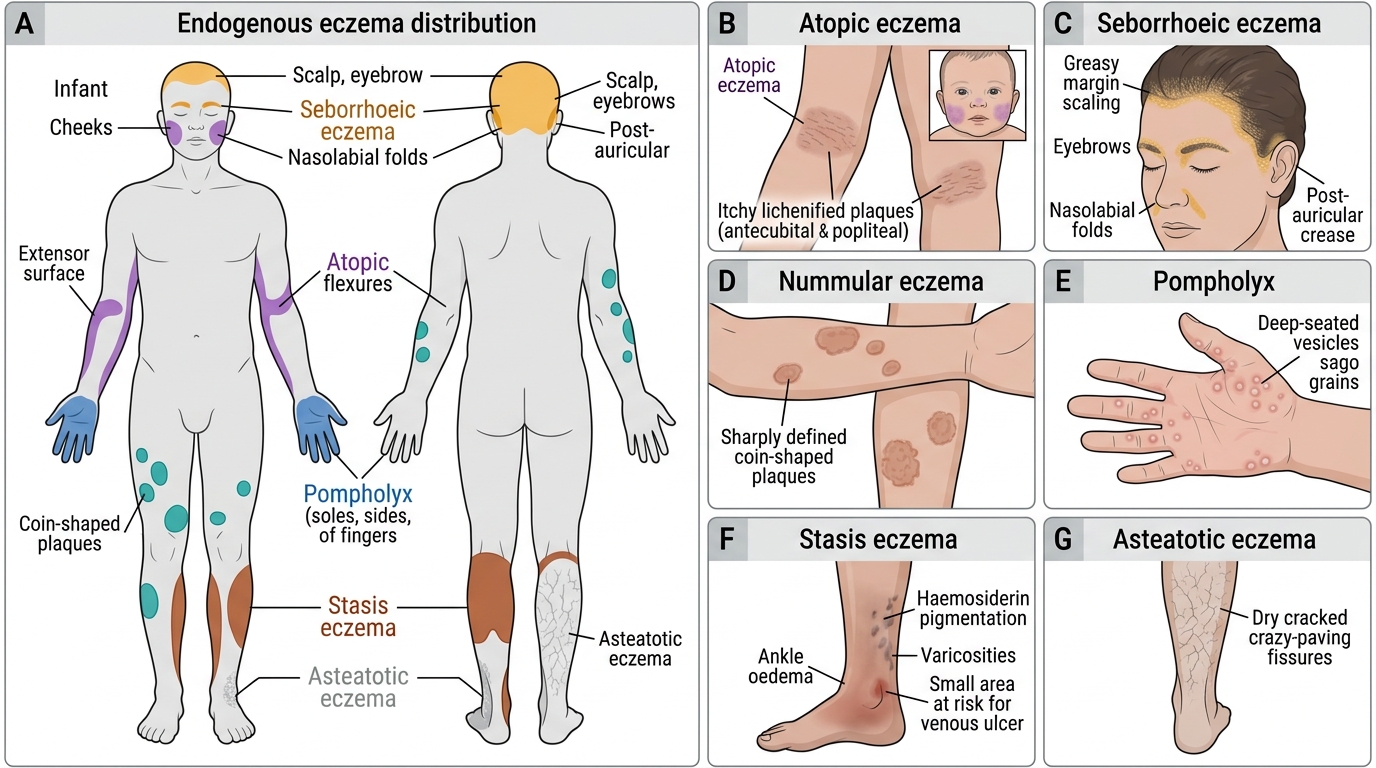
Endogenous eczemas arise from within the patient's own constitution rather than an external contactant, and each has a signature distribution and context that lets you name it from the bedside. Atopic eczema is the prototype: in infants it favours the cheeks and extensor surfaces, but in older children and adults it classically settles in the flexures — the antecubital and popliteal fossae — as itchy, lichenified plaques in a patient with a personal or family history of atopy. Seborrhoeic eczema picks out the sebum-rich zones — scalp, eyebrows, nasolabial folds and post-auricular areas — as greasy, yellowish scaling, and is associated with the commensal yeast Malassezia. Nummular (discoid) eczema forms sharply defined coin-shaped plaques, usually on the limbs.
Three more endogenous types complete the common list. Pompholyx produces deep-seated, intensely itchy vesicles on the palms, soles and sides of the fingers, like sago grains. Stasis (gravitational) eczema appears on the lower legs and ankles of patients with chronic venous insufficiency, accompanied by oedema, haemosiderin pigmentation and sometimes ulceration. Asteatotic eczema (eczema craquelé) is the dry, cracked 'crazy-paving' eczema of the lower legs in elderly patients, worse in winter and with over-washing. Recognising the distribution is usually enough to make the diagnosis.
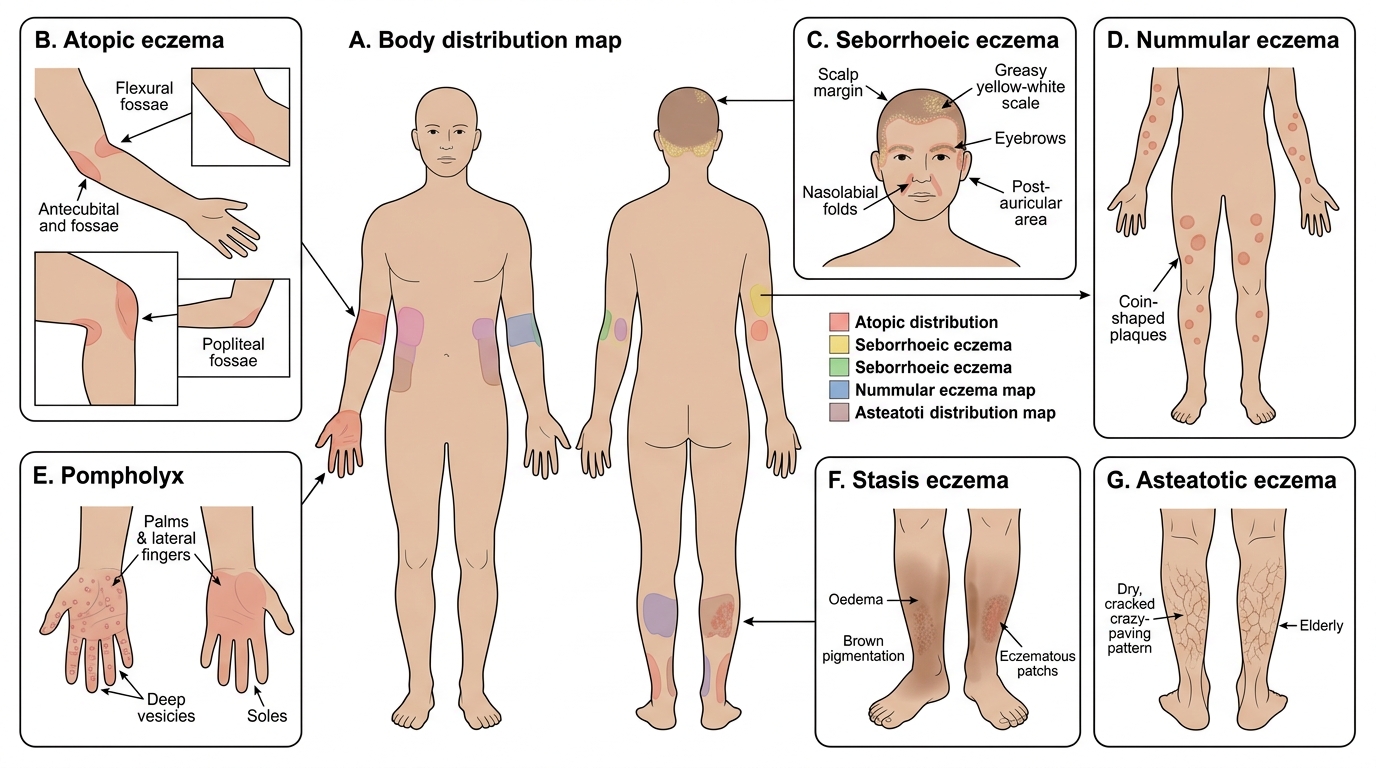
Distribution Patterns of Endogenous Eczemas
- Atopic: flexural in children/adults; atopic history; intensely itchy.
- Seborrhoeic: scalp, nasolabial folds, post-auricular; greasy scale; Malassezia-linked.
- Nummular/discoid: coin-shaped plaques, often on limbs.
- Pompholyx: vesicles on palms, soles, lateral fingers.
- Stasis: lower legs with venous insufficiency, oedema, pigmentation.
- Asteatotic: dry cracked lower legs in the elderly, worse in winter.