Page 2 of 20
DR12.1-2 | Eczema Recognition and Basic Treatment — SDL Guide (Part 2)
Recognising Exogenous Eczema: Contact Dermatitis
Recognising Contact Dermatitis: Irritant vs Allergic
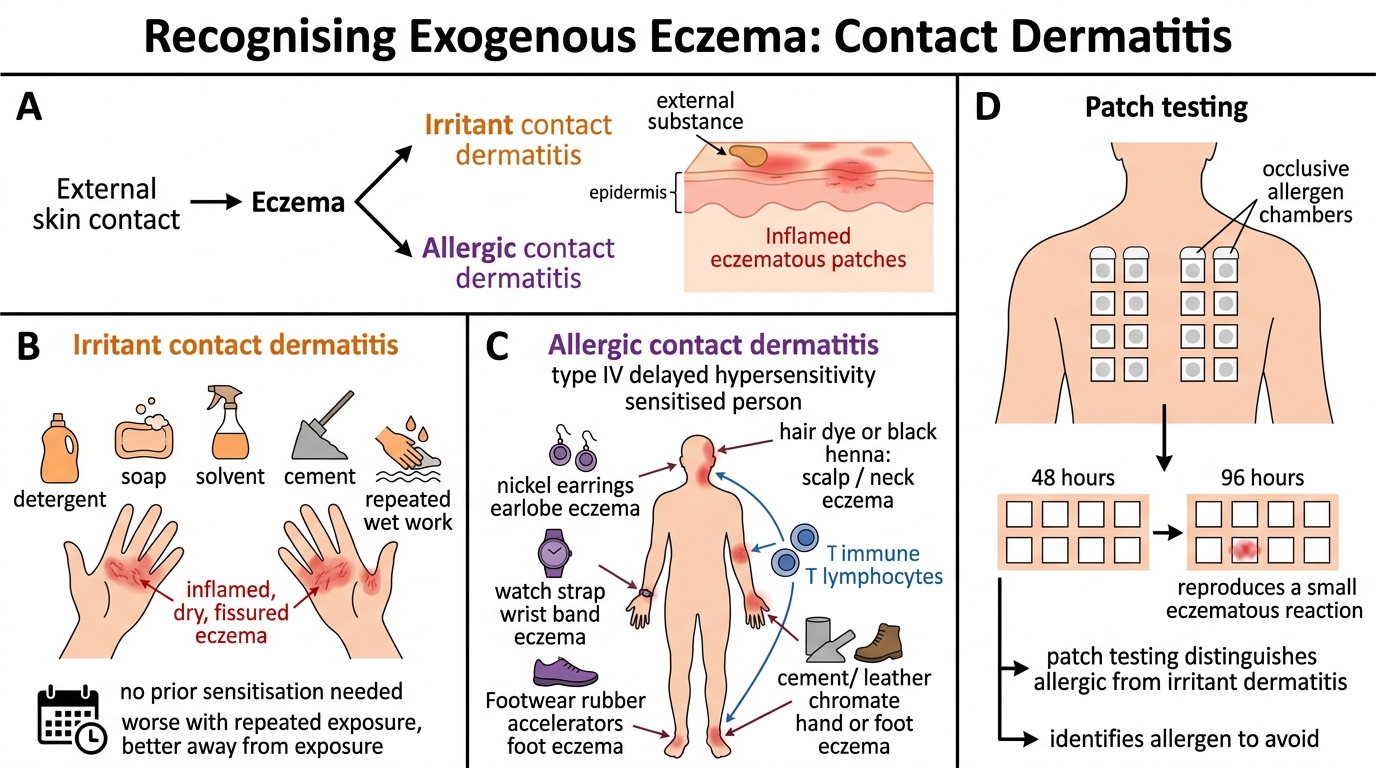
Exogenous eczema is caused by something the skin touches, and separating its two forms — irritant and allergic — is a high-yield clinical skill because their management diverges. Irritant contact dermatitis is the commoner form: a direct toxic effect of substances such as detergents, soaps, solvents, cement or repeated wet work, producing eczema wherever and whenever exposure is sufficient. It needs no prior sensitisation, so it can affect anyone, and the history of a relevant exposure that correlates with flares (better on days off, worse at work) is the key clue. Allergic contact dermatitis is an immunological type IV reaction in a person already sensitised to a specific allergen; common Indian culprits include nickel (jewellery, bindi clips), paraphenylenediamine in hair dyes and black henna, fragrances, rubber accelerators in footwear, and chromate in cement and leather.
The pattern and site of the eczema often betray the allergen — a band of eczema under a watch strap, eczema of the earlobes from earrings, or eyelid eczema from nail varnish transferred by touch. When the history does not reveal the cause, patch testing is the definitive investigation: standardised allergens are applied to the back under occlusion and read at 48 and 96 hours, a positive reaction reproducing a small patch of eczema. Patch testing distinguishes allergic from irritant dermatitis and identifies exactly what the patient must avoid.
- Irritant: direct chemical damage; no sensitisation; affects anyone with enough exposure; history ties flares to exposure.
- Allergic: type IV hypersensitivity; needs prior sensitisation; distribution points to allergen; patch testing confirms and identifies the allergen.
- Avoidance of the identified irritant/allergen is the single most effective treatment for exogenous eczema.
SELF-CHECK
A woman develops a sharply demarcated patch of itchy eczema only on the skin directly beneath her new metal watch strap. Which statement is correct?
A. This is irritant contact dermatitis and will resolve without identifying any allergen
B. This is allergic contact dermatitis (often to nickel); patch testing can confirm the allergen and avoidance is curative
C. This is atopic eczema because it is itchy
D. Patch testing is read immediately at 15 minutes like a prick test
Reveal Answer
Answer: B. This is allergic contact dermatitis (often to nickel); patch testing can confirm the allergen and avoidance is curative
Eczema confined to the site of contact with a metal object strongly suggests ALLERGIC contact dermatitis, classically to nickel. Patch testing (read at 48 and 96 hours, not immediately) confirms the type IV allergen, and avoiding the metal is curative.
Differentiating Eczema Types and Key Investigations
Eczema Mimics and Targeted Investigations
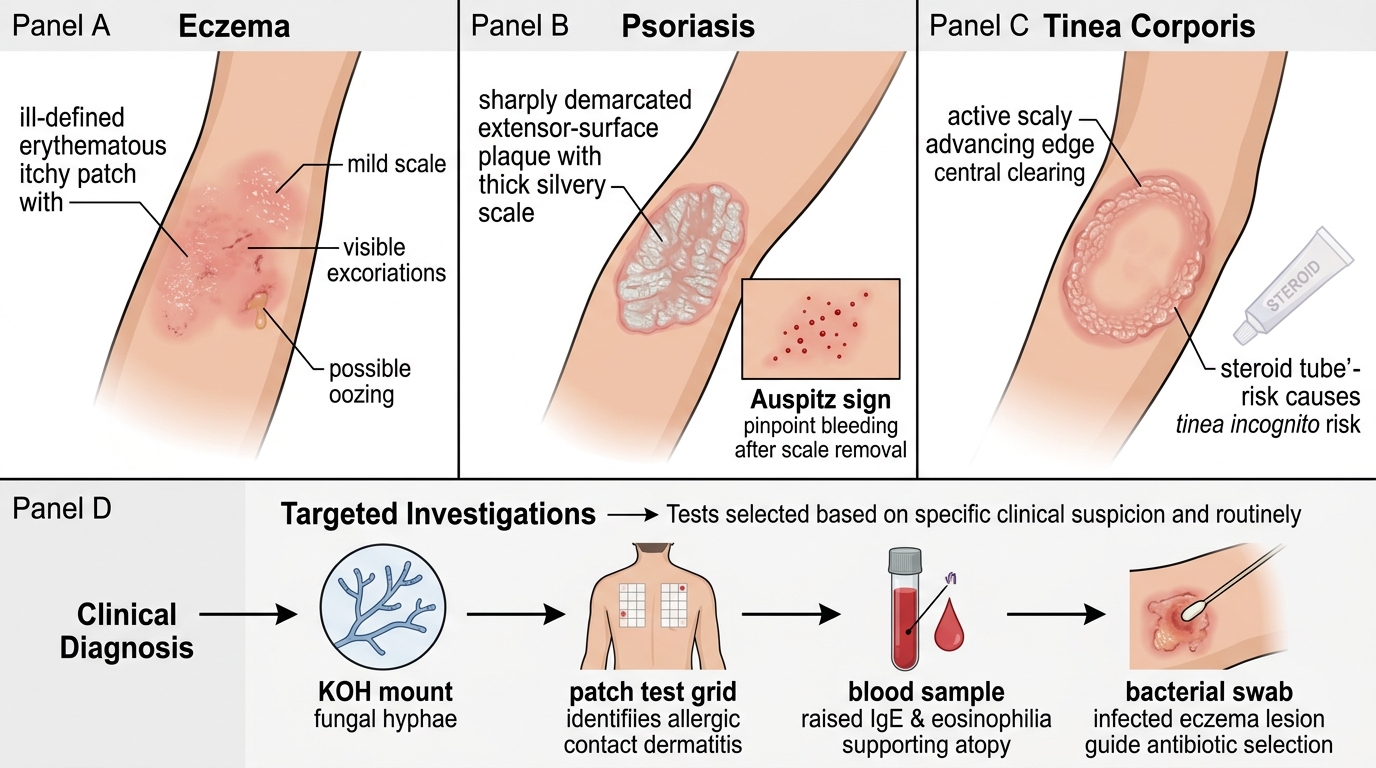
Eczema must be separated from the conditions that mimic it, because treating the wrong diagnosis wastes time and can worsen the disease. The commonest trap in India is mistaking tinea (dermatophyte infection) for eczema: tinea has an active, scaly, advancing edge with central clearing, and applying a topical steroid (as one would for eczema) produces the modified, deceptive picture of tinea incognito. A skin scraping examined in potassium hydroxide (KOH) mount settles this by showing fungal hyphae. The other key mimic is psoriasis, which forms well-defined plaques with thick silvery scale on extensor surfaces (knees, elbows, scalp) and shows the Auspitz sign (pinpoint bleeding when the scale is lifted) — features absent in eczema.
Most eczema is a clinical diagnosis needing no test, but targeted investigations help in specific situations. Patch testing is reserved for suspected allergic contact dermatitis to identify the allergen. A raised serum IgE and peripheral eosinophilia support atopy in atopic eczema but are not required for diagnosis. A bacterial swab guides antibiotic choice when secondary infection is suspected. The clinical reasoning, not a laboratory result, remains the backbone of eczema diagnosis.
| Feature | Eczema | Psoriasis | Tinea corporis |
|---|---|---|---|
| Margin | Ill-defined | Well-defined plaque | Active raised edge, central clearing |
| Scale | Fine, variable | Thick silvery | Peripheral scale |
| Auspitz sign | Absent | Present | Absent |
| KOH mount | Negative | Negative | Hyphae positive |
| Key clue | Itch, flexural/contact pattern | Extensor plaques, nail pits | Annular, spreading edge |
Treating Eczema: The Stepwise Approach
Provided image
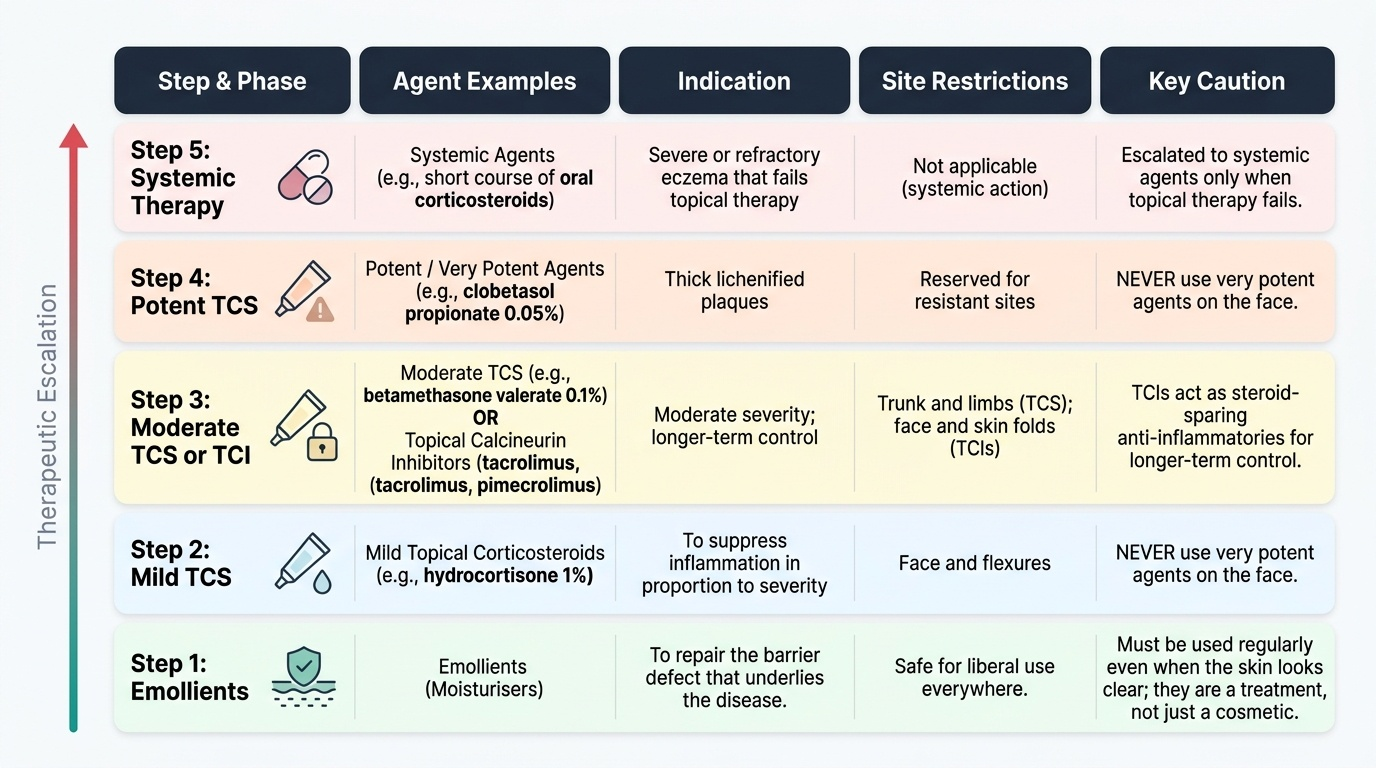
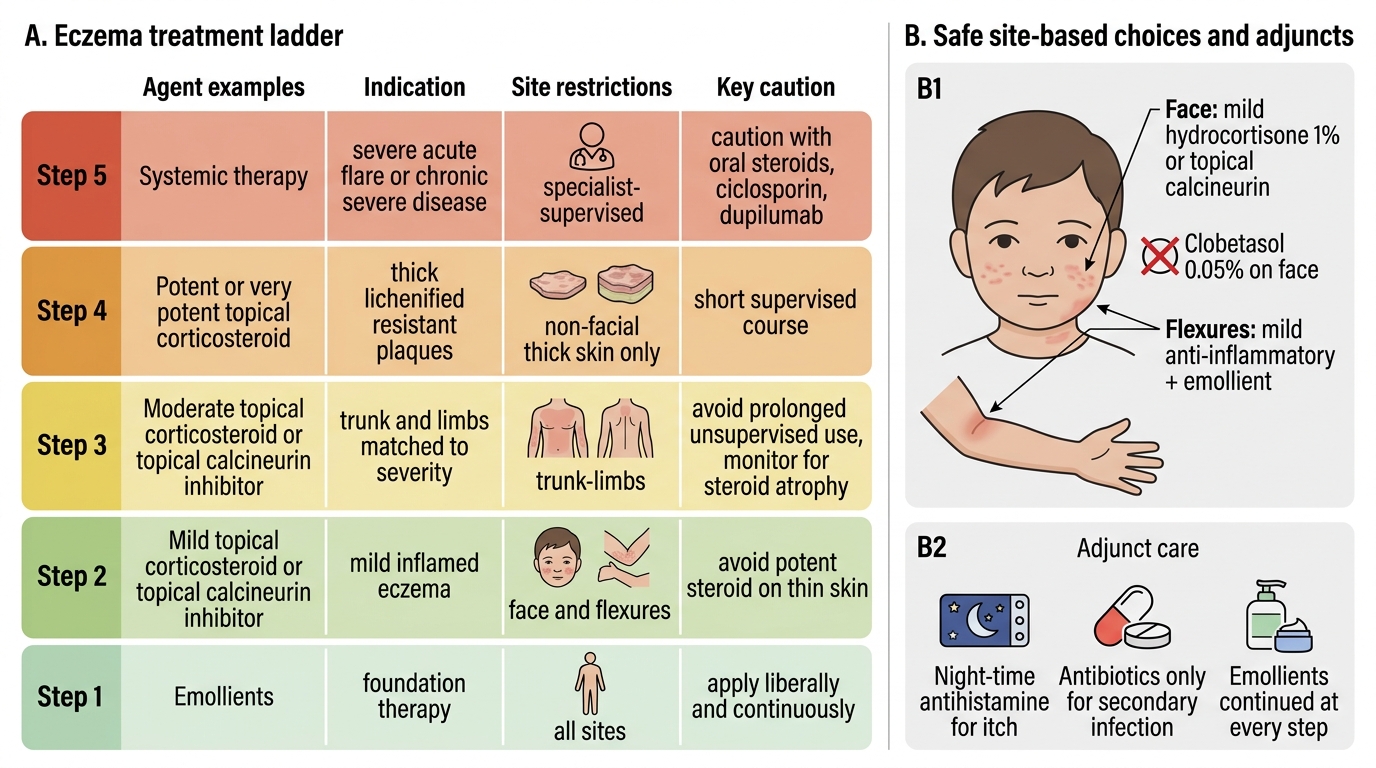
Eczema treatment is a ladder built on a single foundation: restore the barrier first, then suppress the inflammation in proportion to severity. Emollients (moisturisers) are the base of every regimen and must be used liberally and regularly, even when the skin looks clear, because they repair the barrier defect that underlies the disease — they are a treatment, not just a cosmetic. On top of emollients sit the anti-inflammatory agents. Topical corticosteroids are the workhorse, but they must be matched to site and severity using the potency ladder: mild (hydrocortisone 1%) for the face and flexures, moderate and potent agents (betamethasone valerate 0.1%) for the trunk and limbs, and very potent agents (clobetasol propionate 0.05%) reserved for thick lichenified plaques on resistant sites, never the face. Topical calcineurin inhibitors (tacrolimus, pimecrolimus) are steroid-sparing anti-inflammatories that are safe on the face and skin folds for longer-term control.
Several adjuncts complete the picture. Sedating antihistamines at night help the itch-driven sleep disturbance; secondary bacterial infection (weeping, golden crusting, often Staphylococcus aureus) needs topical or oral antibiotics; and severe or refractory eczema that fails topical therapy is escalated to systemic agents — a short course of oral corticosteroids for an acute flare, or specialist-initiated agents such as ciclosporin or the biologic dupilumab for chronic severe atopic eczema. A crucial safety message for Indian practice is to never use potent steroids on the face and to counsel patients against over-the-counter steroid-containing fairness or anti-fungal combination creams.
Eczema Treatment Ladder and Site-Safe Therapy
- Step 1 — Emollients: foundation; apply liberally and continuously.
- Step 2 — Mild topical steroid / topical calcineurin inhibitor: face and flexures.
- Step 3 — Moderate/potent topical steroid: trunk and limbs, matched to severity.
- Step 4 — Very potent topical steroid: thick lichenified plaques on resistant non-facial sites.
- Step 5 — Systemic therapy: short oral steroid for acute flare; specialist ciclosporin / dupilumab for severe chronic disease.
- Adjuncts: night-time antihistamine for itch; antibiotics for secondary infection.
SELF-CHECK
A mother brings her 6-year-old with mild itchy eczema in the antecubital folds and on the cheeks. Which topical anti-inflammatory choice is safest and most appropriate for the FACE?
A. Clobetasol propionate 0.05% (very potent) twice daily
B. Mild hydrocortisone 1% or a topical calcineurin inhibitor
C. A potent steroid-antifungal combination cream
D. No anti-inflammatory; emollient alone is always sufficient even when inflamed
Reveal Answer
Answer: B. Mild hydrocortisone 1% or a topical calcineurin inhibitor
On the face and flexures only MILD topical steroids (e.g. hydrocortisone 1%) or steroid-sparing topical calcineurin inhibitors should be used. Potent/very potent steroids on a child's face cause atrophy and steroid rosacea, and combination 'fairness/antifungal' steroid creams are harmful and contraindicated here.