Page 3 of 20
DR12.1-2 | Eczema Recognition and Basic Treatment — SDL Guide (Part 3)
Putting It Together: Applying Treatment to Each Eczema Type
Eczema Treatment Matched to Type and Site
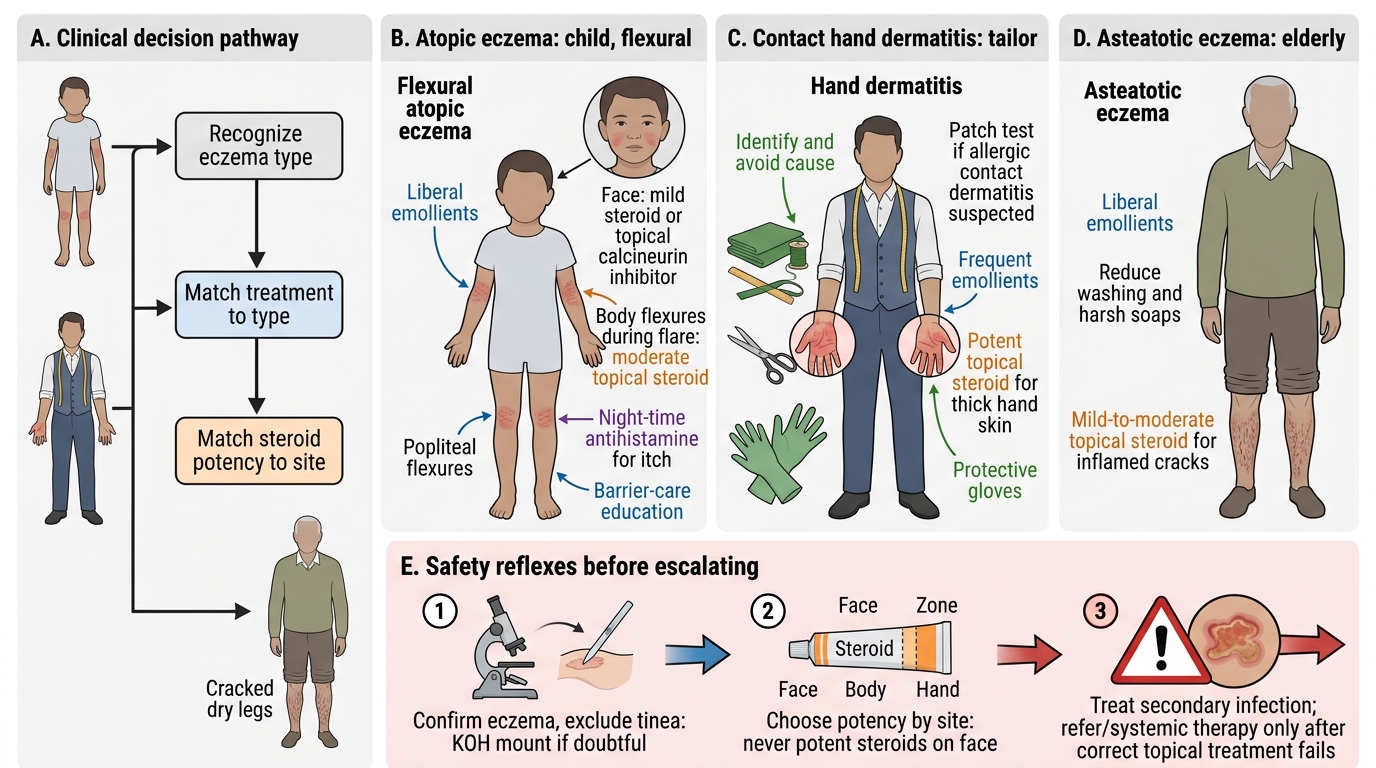
The final skill is to fold recognition and treatment into a single clinical decision: name the eczema type, then choose treatment that matches both the type and the body site. For the child with flexural atopic eczema, that means liberal emollients, a mild steroid or calcineurin inhibitor on the face, a moderate steroid for body flexures during flares, night-time antihistamine, and education on long-term barrier care. For the tailor with allergic or irritant hand dermatitis, the decisive intervention is identifying and avoiding the cause — patch testing if allergic contact dermatitis is suspected — supported by emollients, a potent steroid for the thickened hand skin, and protective gloves. For the elderly man with asteatotic eczema, simple liberal emollients, reduced washing and a mild-to-moderate steroid for inflamed cracks usually suffice.
Three safety reflexes should now be automatic. First, confirm it is eczema and not tinea (KOH mount if in doubt) before reaching for a steroid. Second, match steroid potency to site — never potent steroids on the face. Third, look for and treat secondary infection, and escalate to systemic therapy or specialist referral only when correctly applied topical treatment has genuinely failed. With these, the great majority of eczema is managed safely at first contact.
- Atopic (child, flexural): emollients + mild steroid/TCI on face + moderate steroid on body flexures + antihistamine + barrier education.
- Contact (hands): identify and avoid cause (patch test if allergic) + emollients + potent steroid + gloves.
- Asteatotic (elderly legs): liberal emollients + reduced washing + mild–moderate steroid for cracks.
- Always: exclude tinea, respect site-based potency limits, treat infection, escalate only on genuine failure.
CLINICAL PEARL
The most damaging mistake in Indian eczema practice is the casual use of potent topical steroids — and worse, over-the-counter steroid-antifungal-antibiotic combination creams — on the face. They flatten inflammation briefly but cause skin atrophy, telangiectasia, perioral dermatitis and steroid-dependent facial rashes, and they convert a simple tinea into a spreading tinea incognito. Teach every patient: on the face, only mild steroids or a calcineurin inhibitor, and never a combination cream bought without prescription.