Page 5 of 20
DR12.3 | Erythroderma Stabilization Before Referral — SDL Guide
Learning Objectives
- Define erythroderma as a generalised inflammatory skin condition involving more than 90% of body surface area.
- List the major causes of erythroderma: psoriasis, eczema, drug reactions and cutaneous T-cell lymphoma.
- Recognise the life-threatening systemic complications: hypothermia, high-output cardiac failure, fluid/electrolyte and protein loss, and secondary infection.
- Provide appropriate primary-care stabilisation — warmth, fluids, electrolytes, emollients, infection control, drug cessation — before referral.
- Identify the red flags that mandate urgent referral and the bundle of care to complete before transfer.
INSTRUCTIONS
Erythroderma is one of the few true dermatological emergencies, and the reason it matters to every doctor — not just dermatologists — is that the patient is systemically ill, not merely 'red all over'. When more than 90% of the skin becomes inflamed, the skin can no longer do its job of regulating temperature, retaining fluid and protein, and keeping infection out, and the patient can die of these failures while waiting for a skin diagnosis. This module teaches you to recognise erythroderma, understand why it kills, and deliver the primary-care stabilisation (DR12.3) that keeps the patient alive long enough to reach specialist care.
References
- Khanna N. Illustrated Synopsis of Dermatology and Sexually Transmitted Diseases, 6th ed. Ch: Erythroderma (Exfoliative Dermatitis) (textbook)
- Sacchidanand S, et al. IADVL Textbook of Dermatology, 4th ed. Section: Erythroderma (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 58-year-old man with long-standing psoriasis is brought to a rural health centre. Over the past week his scaly plaques have merged until almost his entire skin is fiery red, hot, and shedding sheets of scale. He is shivering uncontrollably despite the warm afternoon, his ankles are swollen, and his pulse is racing at 120. The family thinks 'it is only a skin problem' and asks for an ointment. In fact this man has erythroderma, a whole-body skin failure that can kill him within days through hypothermia, high-output cardiac failure and fluid loss — long before any skin diagnosis is confirmed. What you do in the next hour, before he is referred, may decide whether he survives.
WHY THIS MATTERS
Erythroderma is uncommon, but when it presents it is a medical emergency that a primary-care doctor or rural physician will often meet first, before any dermatologist is available. The danger is that it looks like 'just a severe skin disease' while the patient is in fact losing heat, fluid, electrolytes and protein through a vast inflamed surface and may be slipping into cardiac failure. The competency DR12.3 specifically requires you not only to diagnose erythroderma and recognise its complications, but to stabilise the patient before referral — because a patient transferred warm, rehydrated and protected from infection survives the journey, whereas one sent off cold and shocked may not. This is a skill where correct primary care directly saves lives.
RECALL
Recall what the skin normally does, because erythroderma is the failure of exactly these functions. The skin is a thermoregulatory organ: by controlling blood flow and sweating it keeps core temperature stable. It is a barrier that retains water, electrolytes and protein and keeps microbes out. And it is a large vascular bed: widespread cutaneous vasodilation diverts blood to the skin surface. Recall too from physiology that high-output cardiac failure occurs when the heart must pump an abnormally large volume — as happens when a huge area of skin is vasodilated — and that loss of the protein albumin lowers oncotic pressure and causes oedema. Erythroderma turns each of these normal functions into a threat.
Erythroderma: A Total-Skin Emergency
Erythroderma: A Total-Skin Emergency
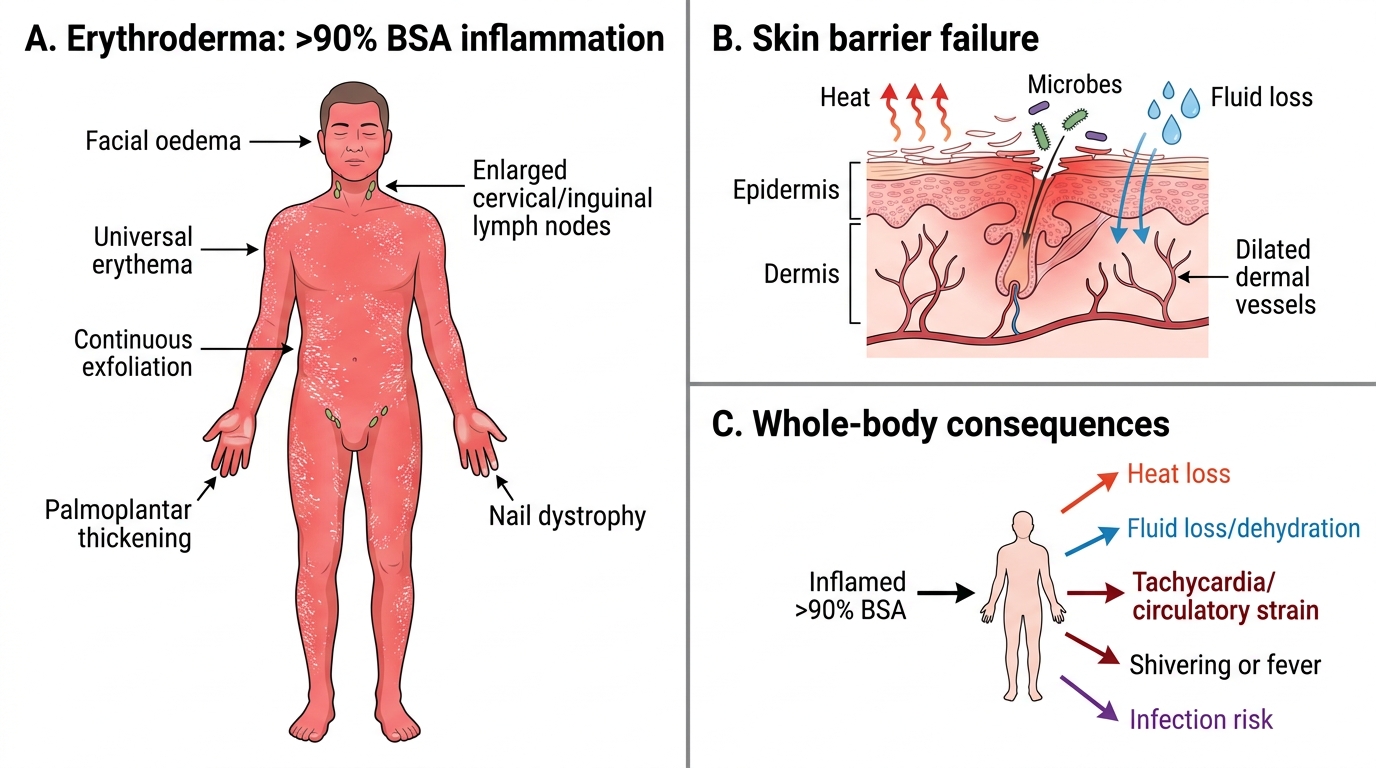
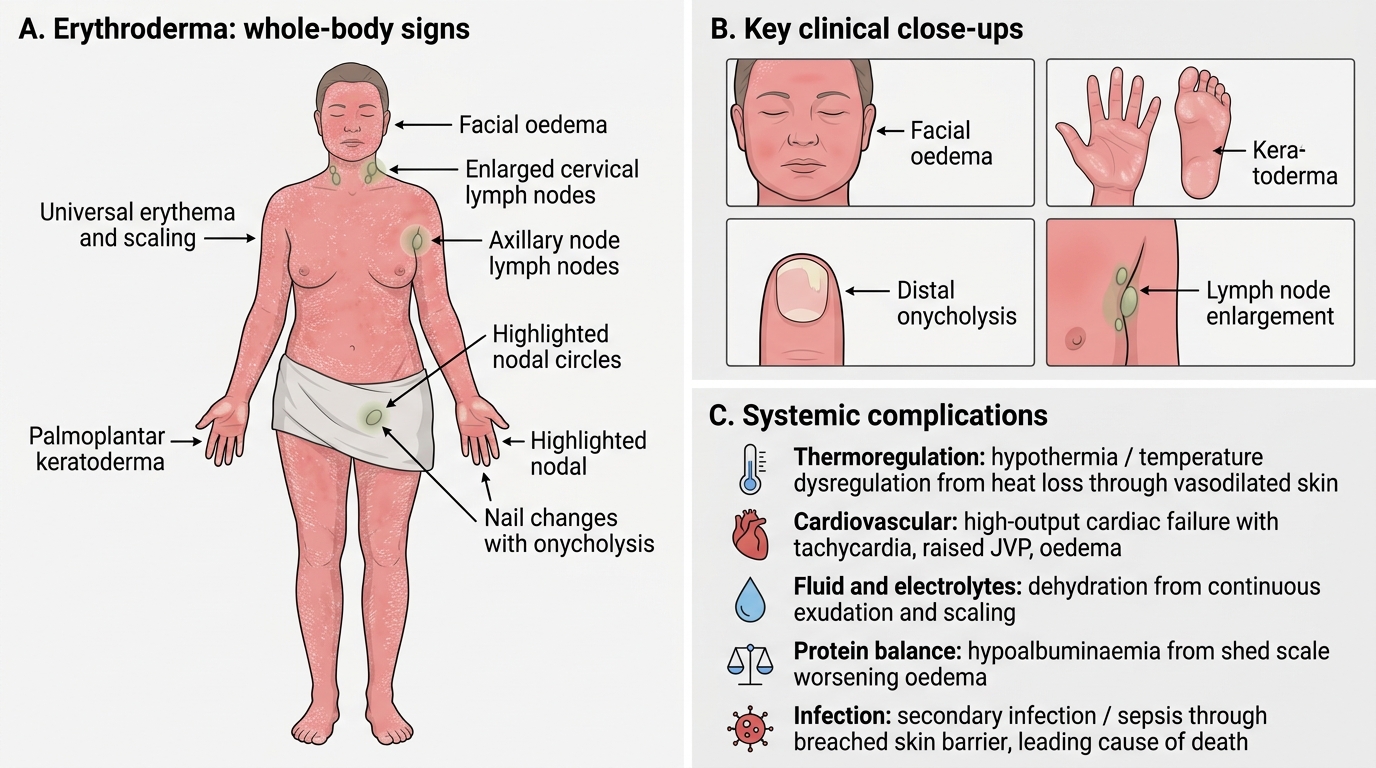
Erythroderma, also called exfoliative dermatitis, is defined as a generalised inflammatory disorder of the skin involving more than 90% of the body surface area. The clinical picture is unmistakable once seen: the whole skin is red, hot to the touch, and continuously shedding scale, often with the patient feeling alternately feverish and intensely cold as thermoregulation fails. The face may be swollen, the palms and soles thickened, the nails dystrophic, and the lymph nodes enlarged. Unlike a localised rash, erythroderma is a state in which the skin as an organ has failed, and the patient is systemically unwell — tachycardic, shivering, dehydrated — rather than simply having an extensive eruption.
The single most important conceptual shift this module asks of you is to stop seeing erythroderma as a skin problem and start seeing it as a whole-body emergency. The redness is the visible sign; the threat is the cascade of systemic consequences — heat loss, fluid loss, circulatory strain and infection — that follows from having 90% of the body surface inflamed. Recognising this at first contact is what triggers the right stabilisation.
- Definition: generalised inflammatory skin disease involving >90% BSA (exfoliative dermatitis).
- Skin signs: universal erythema, warmth, continuous scaling/exfoliation, facial oedema, palmoplantar thickening, nail changes, lymphadenopathy.
- Systemic signs: shivering or fever, tachycardia, dehydration — the patient is systemically ill, not just 'red'.
Causes of Erythroderma: Why the Whole Skin Fails
Aetiological Pathways to Erythroderma
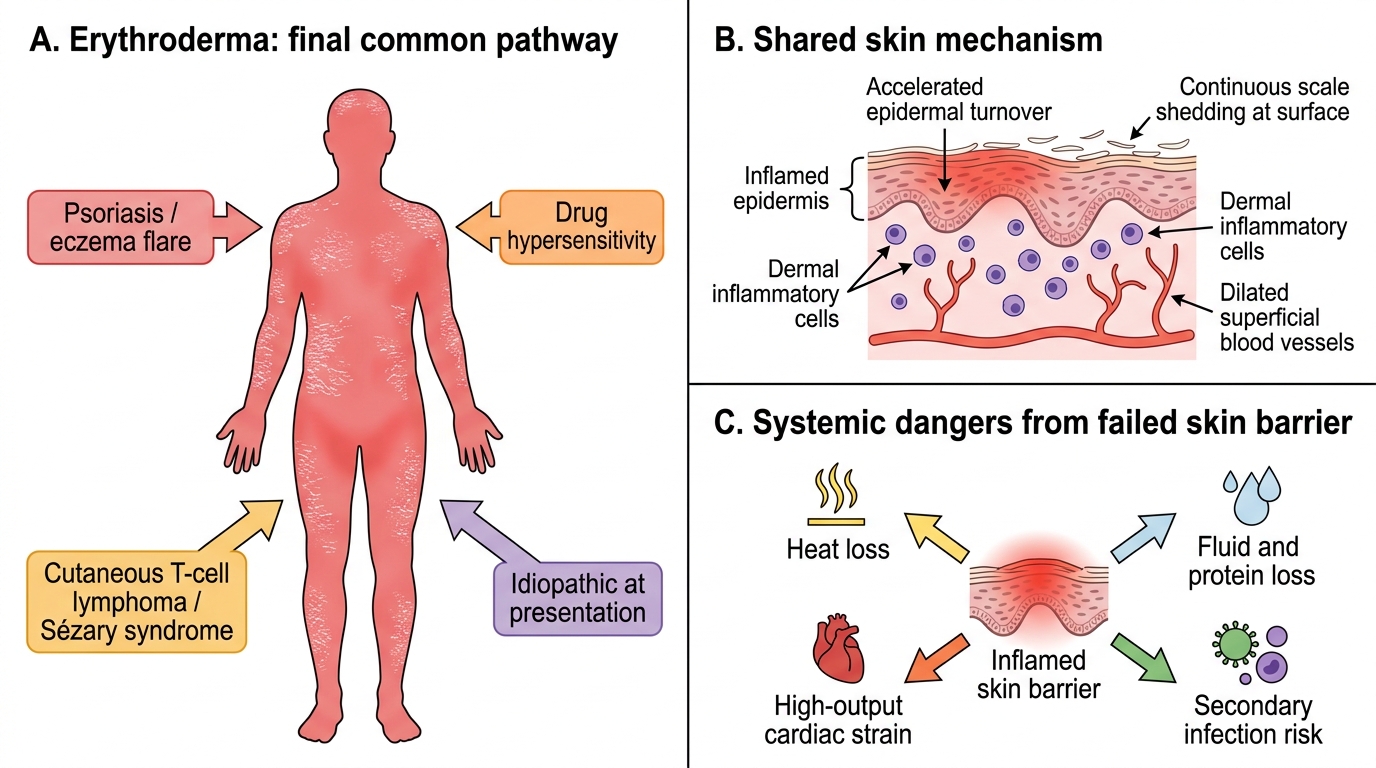
Erythroderma is not a diagnosis in itself but the final common pathway of several underlying conditions, and knowing the causes shapes both the work-up and the eventual specialist treatment. The four major causes are psoriasis and eczema (together the commonest, accounting for the majority of adult cases when a pre-existing dermatosis flares or is provoked), drug reactions (a severe hypersensitivity response to drugs such as sulfonamides, anticonvulsants, allopurinol or gold), and cutaneous T-cell lymphoma (CTCL), particularly the leukaemic form known as Sézary syndrome. In roughly a quarter of cases no cause is found at presentation and the erythroderma is labelled idiopathic until a cause declares itself.
The mechanism, whatever the trigger, converges on the same destructive physiology: a massive inflammatory drive accelerates epidermal turnover so that scale is shed continuously, while widespread cutaneous vasodilation opens the skin's vascular bed. This combination is precisely what produces the systemic dangers — heat escapes through the dilated vessels, fluid and protein leak through the inflamed barrier, the heart strains to supply the dilated skin, and the breached barrier admits infection. Understanding this convergence explains why the stabilisation that follows is the same regardless of the underlying cause.
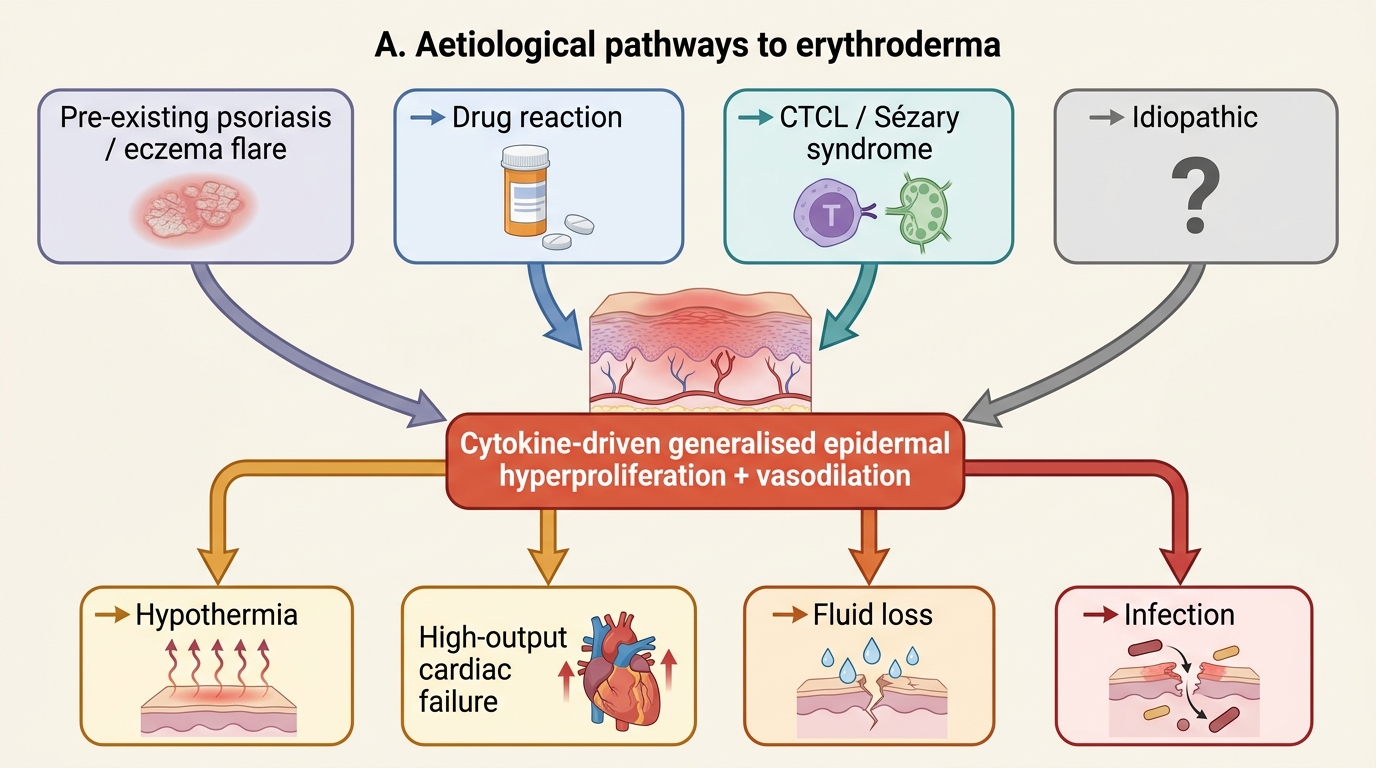
Aetiological Pathways to Erythroderma
- Psoriasis & eczema: commonest causes; a known dermatosis flares into erythroderma.
- Drug reaction: severe hypersensitivity (sulfonamides, anticonvulsants, allopurinol, gold).
- CTCL / Sézary syndrome: malignant T-cell cause; suspect in chronic erythroderma with lymphadenopathy.
- Idiopathic: about a quarter, until a cause emerges.
SELF-CHECK
Which two conditions together account for the majority of cases of erythroderma in adults?
A. Scabies and tinea
B. Psoriasis and eczema
C. Vitiligo and melasma
D. Acne and rosacea
Reveal Answer
Answer: B. Psoriasis and eczema
A flare of a pre-existing PSORIASIS or ECZEMA is the commonest route to erythroderma in adults. Drug reactions and cutaneous T-cell lymphoma (Sézary syndrome) are the other major causes, with about a quarter of cases idiopathic at presentation.
Clinical Features and Systemic Complications
Erythroderma: Clinical Features and Systemic Complications
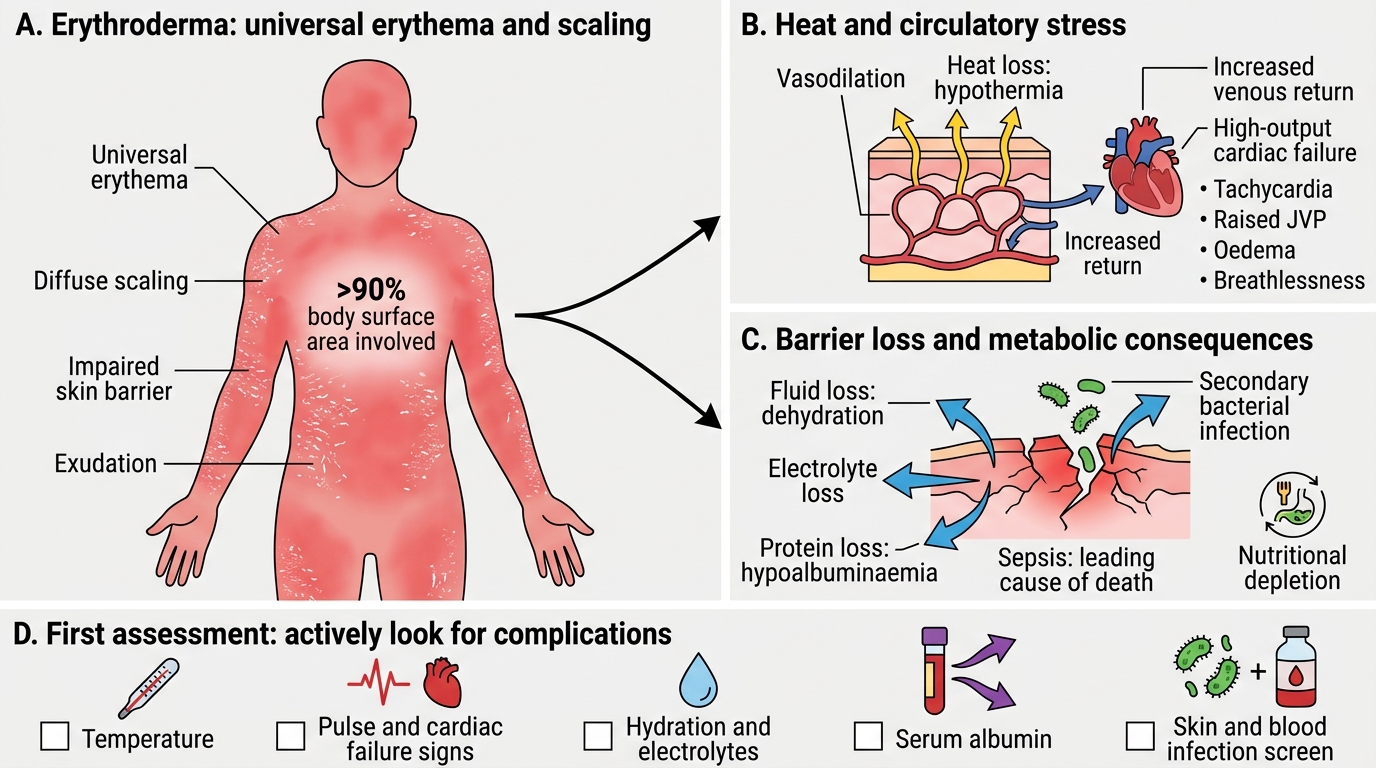
Diagnosing erythroderma clinically is straightforward — universal erythema and scaling over more than 90% of the body — but the clinical assessment must extend immediately to the systemic complications, because these are what threaten life. The breakdown of thermoregulation causes hypothermia (and sometimes swinging hyperthermia), as heat pours out through the vasodilated skin. The same vasodilation increases venous return and cardiac demand, precipitating high-output cardiac failure, recognised by tachycardia, raised jugular venous pressure, oedema and breathlessness — a particular danger in elderly patients or those with existing heart disease. Continuous exudation and scaling cause fluid and electrolyte loss leading to dehydration, and the loss of shed protein produces hypoalbuminaemia, worsening the oedema.
Two further hazards complete the picture. The breached barrier permits secondary bacterial infection, which can progress to sepsis — the leading cause of death in erythroderma. And the metabolic demand of the inflamed skin, together with poor intake, leads to nutritional depletion. Every one of these complications must be actively looked for at the first assessment: check the temperature, the pulse and signs of cardiac failure, the hydration and the serum albumin, and the skin and blood for infection. Naming the complications is what directs the stabilisation.
Erythroderma: Clinical Features and Systemic Complications
- Hypothermia / temperature dysregulation: heat lost through vasodilated skin.
- High-output cardiac failure: from widespread cutaneous vasodilation; tachycardia, raised JVP, oedema.
- Fluid & electrolyte loss: dehydration from continuous exudation and scaling.
- Protein loss / hypoalbuminaemia: from shed scale; worsens oedema.
- Secondary infection / sepsis: through the breached barrier; the leading cause of death.