Page 6 of 20
DR12.3 | Erythroderma Stabilization Before Referral — SDL Guide (Part 2)
Working Up the Underlying Cause
Working Up the Cause of Erythroderma
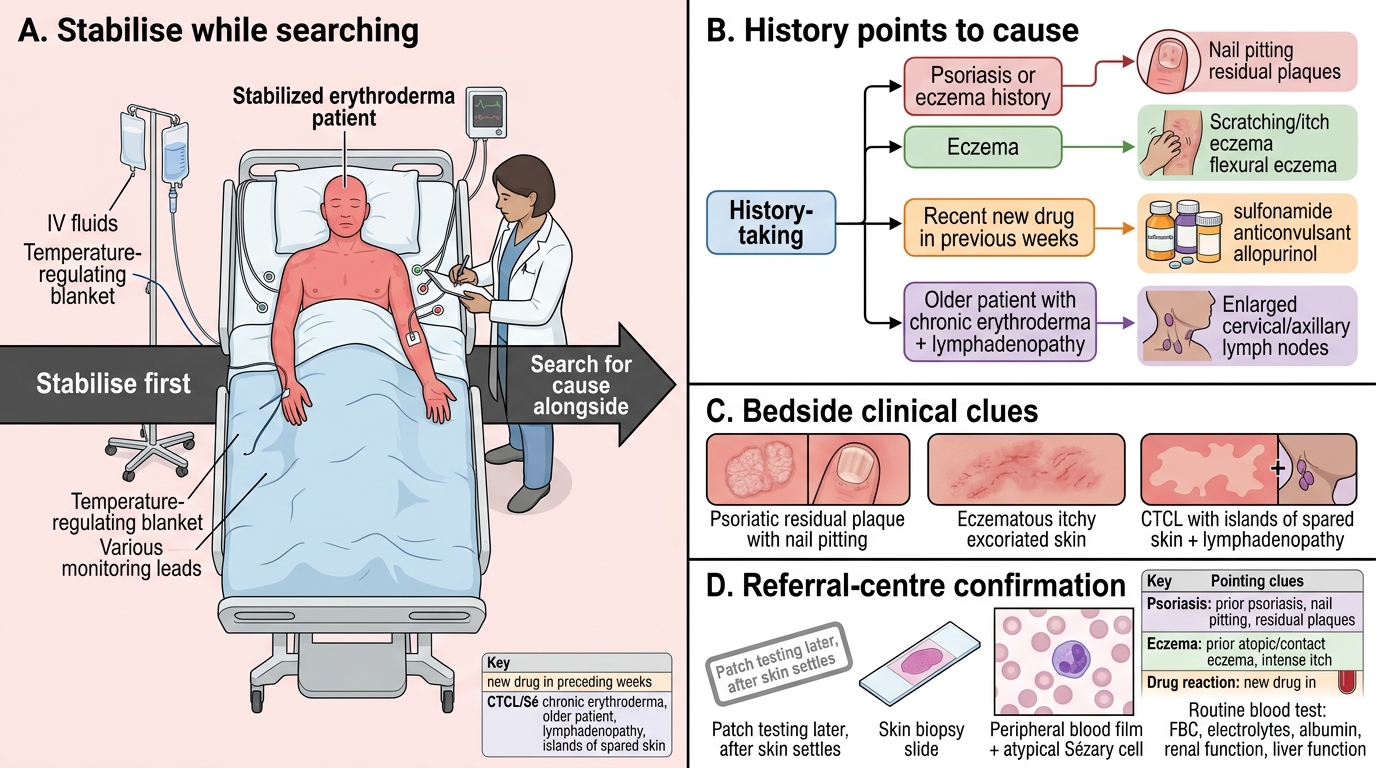
Once the patient is recognised and stabilisation has begun, the next task is to seek the underlying cause, because the eventual definitive treatment depends on it — though this work-up never delays the life-saving stabilisation. The most useful first step is the history: a known history of psoriasis or eczema points to a dermatosis flare, a recent new drug (especially sulfonamides, anticonvulsants or allopurinol started in the preceding weeks) points to a drug reaction, and chronic erythroderma with prominent lymphadenopathy in an older patient raises suspicion of cutaneous T-cell lymphoma. Clinical clues such as residual psoriatic plaques, nail pitting, or the islands of spared skin sometimes seen in CTCL help point the way.
Investigations confirm the cause but are largely the referral centre's task. A skin biopsy may show features of the underlying disease, a peripheral blood film is examined for atypical circulating Sézary cells when lymphoma is suspected, and routine bloods (full blood count, electrolytes, albumin, renal and liver function) assess both cause and complications. Patch testing for a contact cause is deferred until the skin has settled. The key principle is that the search for a cause runs alongside, and never ahead of, keeping the patient alive.
| Cause | Pointing clues | Confirmatory clue |
|---|---|---|
| Psoriasis | Prior psoriasis, nail pitting, residual plaques | Biopsy; history |
| Eczema | Prior atopic/contact eczema, intense itch | Biopsy; history |
| Drug reaction | New drug in preceding weeks (sulfonamide, anticonvulsant, allopurinol) | Drug history; resolves on stopping drug |
| CTCL / Sézary | Chronic course, lymphadenopathy, elderly | Biopsy; Sézary cells on blood film |
SELF-CHECK
An elderly man has had erythroderma for several months with prominent generalised lymphadenopathy. Which investigation specifically helps identify a malignant (cutaneous T-cell lymphoma) cause?
A. KOH mount of skin scraping
B. Peripheral blood film looking for atypical Sézary cells
C. Random blood glucose
D. Chest X-ray for tuberculosis
Reveal Answer
Answer: B. Peripheral blood film looking for atypical Sézary cells
A chronic erythroderma with lymphadenopathy in an elderly patient raises suspicion of cutaneous T-cell lymphoma (Sézary syndrome). A peripheral blood film examined for atypical circulating Sézary cells (along with skin biopsy) helps identify this malignant cause.
Primary Care Stabilisation Before Referral
Provided image
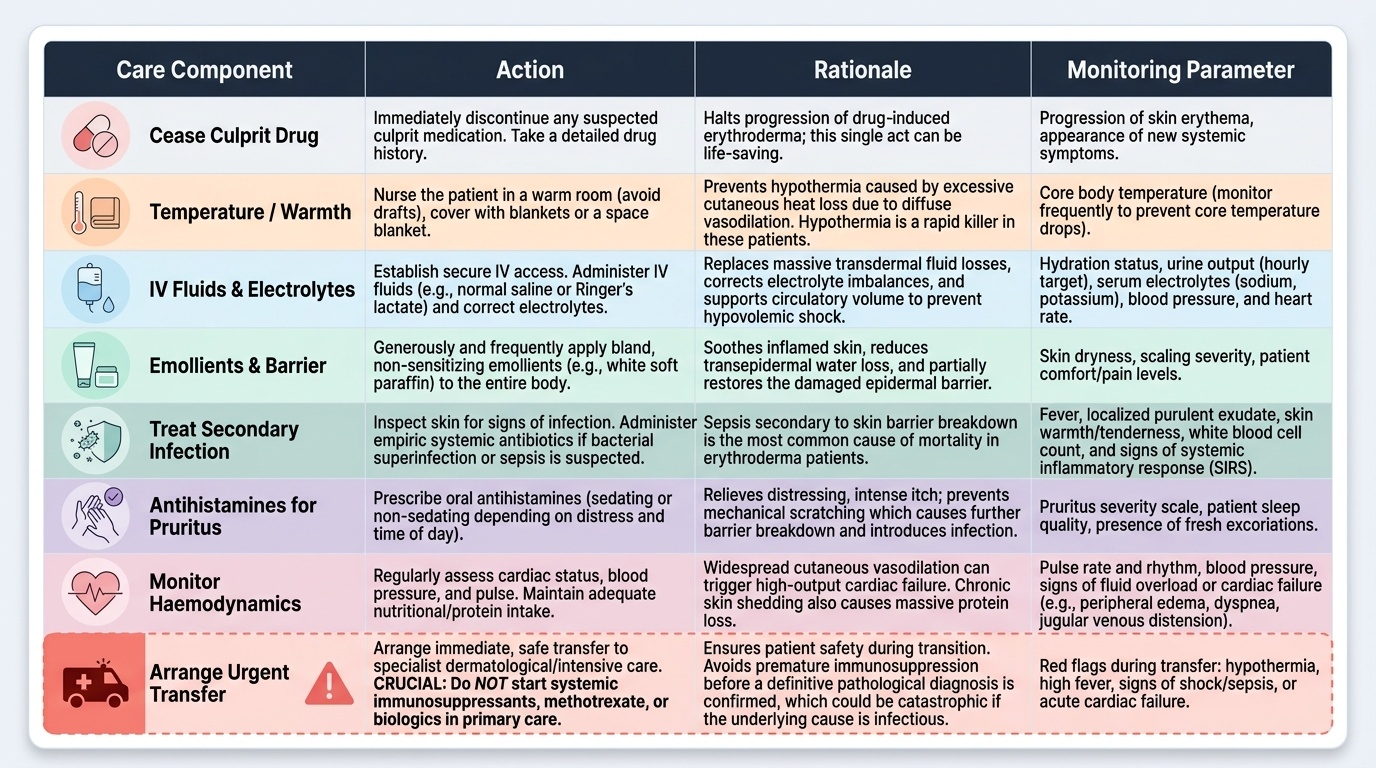
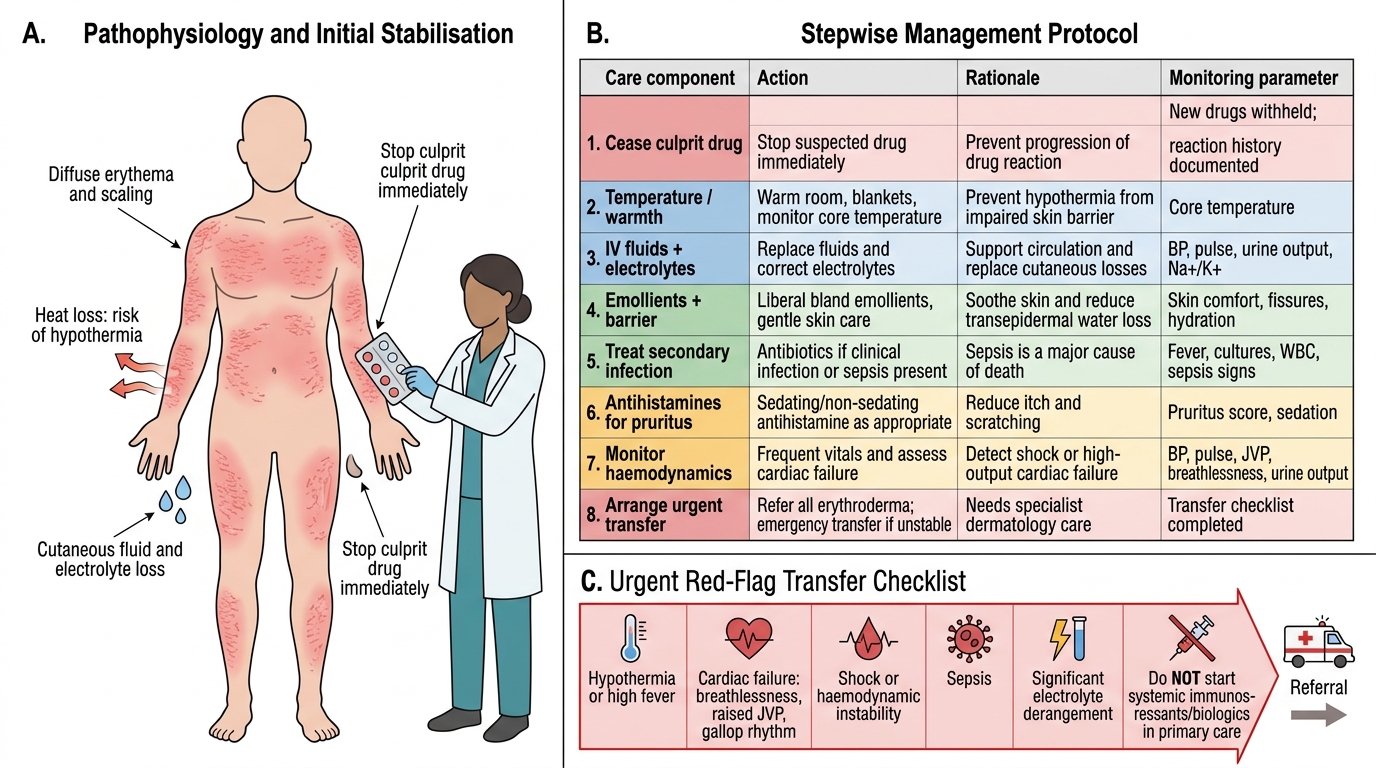
This is the heart of competency DR12.3: whatever the cause, the primary-care doctor's job is to stabilise the failing systems before the patient reaches specialist care, and the steps follow directly from the complications. First, if a drug reaction is suspected, stop the suspected culprit drug immediately — this single act can be life-saving and halts progression. Restore warmth: nurse the patient in a warm room, cover with blankets or a space blanket and monitor core temperature, because hypothermia is an immediate killer. Establish intravenous access and give fluids and correct electrolytes, guided by hydration status, to counter the losses through the skin and support the circulation. Apply bland emollients generously to soothe the skin, reduce water loss and restore some barrier function.
The remaining measures protect against the other complications. Look for and treat secondary infection with appropriate antibiotics if there is evidence of bacterial superinfection, since sepsis is the commonest cause of death. Give antihistamines for distressing itch, ensure adequate nutrition and protein intake, and monitor the pulse and signs of cardiac failure, treating as needed. Crucially, the primary-care doctor does not start disease-specific treatment such as systemic immunosuppressants, methotrexate or biologics — these are specialist decisions made after the cause is confirmed. The goal is a warm, rehydrated, infection-protected patient, safely referred.
Erythroderma Stabilisation Before Referral
- Stop the culprit drug immediately if a drug reaction is suspected.
- Warmth: warm room, blankets, monitor core temperature (prevent hypothermia).
- IV fluids + electrolytes: replace cutaneous losses, support circulation.
- Emollients: soothe skin, reduce water loss, restore barrier.
- Treat secondary infection with antibiotics if present (sepsis is the leading cause of death).
- Antihistamines for itch; ensure nutrition/protein; monitor for cardiac failure.
- Do NOT start systemic immunosuppressants/biologics in primary care — refer.
Deciding to Refer: Red Flags and Transfer Checklist
Erythroderma Referral: Red Flags and Transfer Checklist
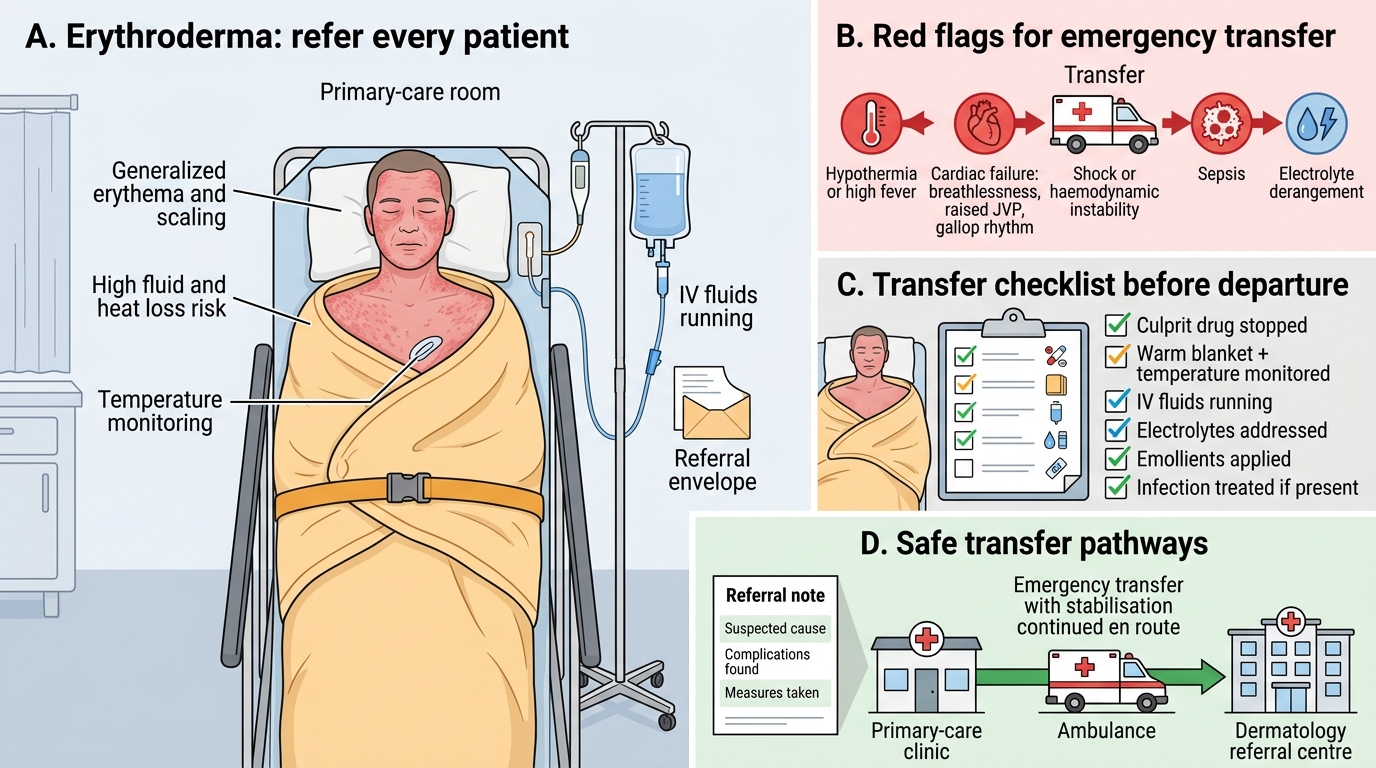
Every patient with erythroderma needs specialist dermatological care, so the question is not whether to refer but how to refer safely and how urgently. Red flags demanding the most urgent transfer include hypothermia or high fever, signs of cardiac failure (breathlessness, raised JVP, gallop rhythm), haemodynamic instability or shock, evidence of sepsis, and significant electrolyte derangement — any of these means the patient must travel as an emergency, with stabilisation continued en route. The primary-care doctor's final act is to mentally run through a transfer checklist confirming the stabilisation bundle is in place.
The checklist is simply the stabilisation steps, verified: the culprit drug stopped, the patient kept warm with temperature monitored, intravenous fluids running and electrolytes addressed, emollients applied, infection treated if present, and a clear referral note documenting the suspected cause, the complications found, and the measures taken. A patient who arrives at the referral centre warm, rehydrated, protected from infection and with a documented account of care is far more likely to survive than one sent off cold and shocked. Completing this bundle before transfer is the measurable outcome of competency DR12.3.
- Red flags for emergency transfer: hypothermia/high fever, cardiac failure, shock, sepsis, electrolyte derangement.
- Transfer checklist: culprit drug stopped; kept warm + temperature monitored; IV fluids/electrolytes; emollients applied; infection treated; referral note with cause, complications and care given.
- Continue stabilisation during transfer, never pause it to await diagnosis.
CLINICAL PEARL
Remember that in erythroderma the patient can die of the complications before anyone knows the underlying skin diagnosis. The two most immediate killers are hypothermia and high-output cardiac failure from the vast vasodilated skin surface, and the commonest ultimate cause of death is sepsis through the breached barrier. So lead with warmth, fluids and infection control — not with a search for the cause. Stabilise first; diagnose later.