Page 1 of 11
DR11.1 | Dermatologic Manifestations of HIV — SDL Guide
Learning Objectives
- Describe the morphological spectrum of HIV-associated dermatoses and recognise the skin as an early indicator of underlying immunosuppression
- Correlate specific dermatoses and opportunistic infections with the depth of immunosuppression as measured by CD4 count
- Diagnose common HIV-related skin conditions from their clinical features and select appropriate laboratory investigations (CD4 count, HIV serology, skin biopsy, KOH mount, Tzanck smear)
- Outline the principles of management, including antiretroviral therapy as the cornerstone, condition-specific treatment, and recognition of immune reconstitution inflammatory syndrome (IRIS)
INSTRUCTIONS
Skin and mucosal disease is among the earliest, most visible, and most diagnostically useful manifestations of HIV infection. More than 90% of people living with HIV develop a cutaneous disorder during the course of their illness, and the pattern of dermatoses tracks closely with the degree of immune compromise. For the clinician, the skin is therefore a readable window into a patient's immune status — a single examination can suggest the diagnosis of HIV, estimate the depth of immunosuppression, and signal the need for CD4 testing and antiretroviral therapy. This SDL equips you to read that window: to recognise the characteristic dermatoses, link them to CD4 strata, investigate appropriately, and manage them within the framework of HIV care.
References
- Sacchidanand S, et al. (eds). IADVL Textbook of Dermatology, 4th ed. Ch: Cutaneous Manifestations of HIV/AIDS (textbook)
- Khanna N. Illustrated Synopsis of Dermatology and Sexually Transmitted Diseases, 5th ed. Ch: HIV Infection and the Skin (textbook)
- National AIDS Control Organisation (NACO). National Guidelines for HIV Care and Treatment. Ministry of Health and Family Welfare, Government of India (policy)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 34-year-old man comes to the dermatology OPD complaining only of dandruff and an itchy scalp that has not responded to the medicated shampoos he has tried for several months. On examination you find greasy, erythematous scaling not just on the scalp but spreading across the eyebrows, nasolabial folds, and central chest — a strikingly extensive and refractory seborrhoeic dermatitis. You also notice a few scattered umbilicated papules on his face and a white, corrugated plaque on the lateral border of his tongue that does not scrape off. None of these findings on its own is alarming. Together, in a young adult, they tell a different story — one that begins not on the skin but in the immune system. A CD4 count and an HIV test are ordered, and both confirm what the skin has already suggested. This is how HIV frequently announces itself: not with fever or weight loss, but with the skin speaking first.
WHY THIS MATTERS
For the final-year MBBS student and intern, recognising the cutaneous manifestations of HIV is a practical, high-yield clinical skill. India has one of the largest populations of people living with HIV in the world, and many present first to general practitioners, dermatologists, or physicians with skin complaints rather than to an HIV clinic. The ability to recognise that an extensive seborrhoeic dermatitis, a stubborn oral thrush, an atypical zoster, or a cluster of molluscum in an adult may signal underlying immunosuppression allows you to initiate timely testing, counselling, and referral — often years earlier than the patient would otherwise be diagnosed. Because the dermatoses track CD4 count, the skin also lets you gauge how advanced the disease is and prioritise antiretroviral therapy and opportunistic-infection prophylaxis. This is competency DR11.1: diagnosing and managing common dermatologic manifestations of HIV from clinical features and appropriate laboratory tests.
RECALL
Before we proceed, recall from your Microbiology and Immunology teaching that HIV is a retrovirus that selectively infects and progressively depletes CD4+ T-helper lymphocytes, the central coordinators of cell-mediated immunity. As the CD4 count falls, cell-mediated immunity fails first, which is why the earliest opportunistic problems are those normally held in check by T cells — reactivation of latent herpesviruses, dermatophyte and candidal overgrowth, and impaired control of intracellular organisms. Recall also that many of the agents responsible for HIV dermatoses are latent viruses already present in most adults: herpes simplex virus, varicella-zoster virus, Epstein-Barr virus, and human herpesvirus-8. In a healthy host these are controlled; in immunosuppression they reactivate and behave atypically. Finally, recall the simple bedside tests you have already learned — the KOH mount for fungi and the Tzanck smear for herpetic vesicles — because they remain central to diagnosing these conditions.
The Skin as a Window into HIV Status
Skin Clues to HIV-Related Immunosuppression
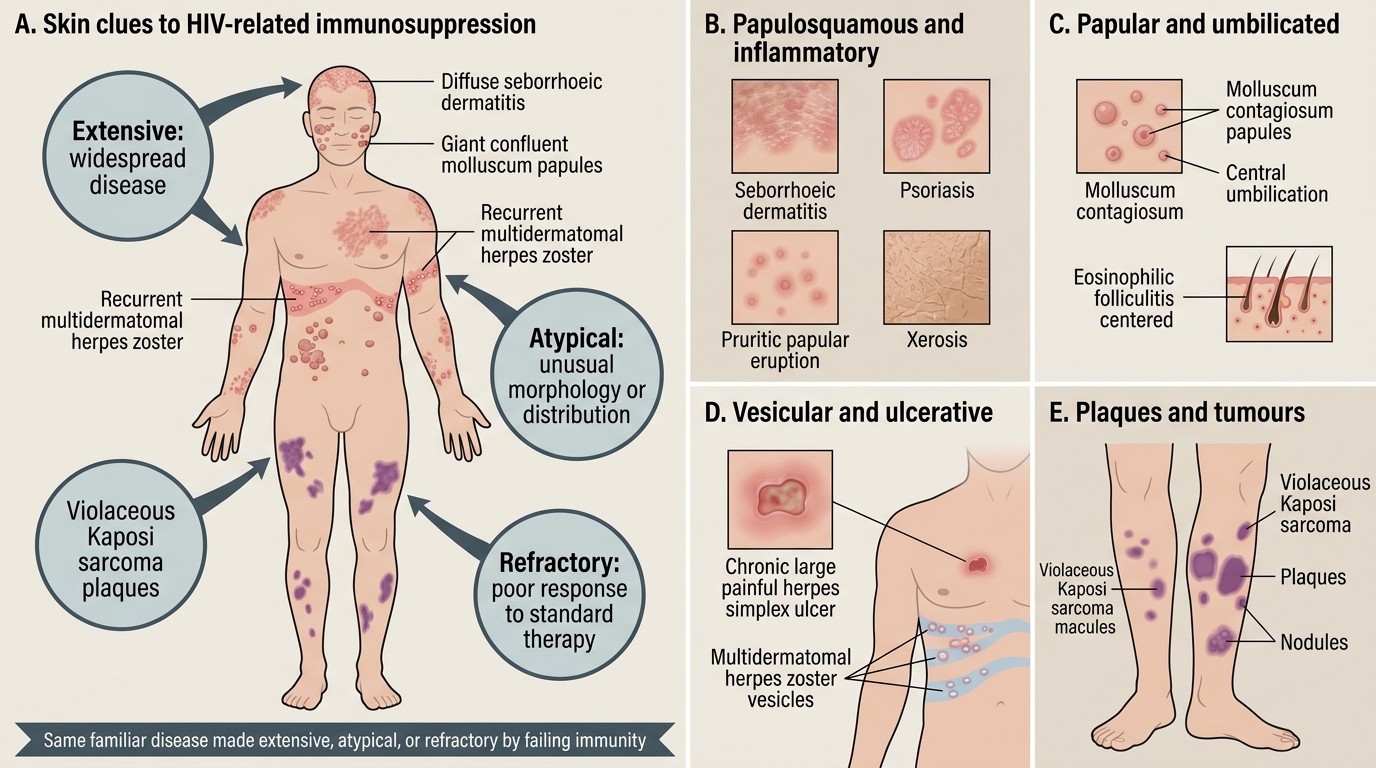
The cutaneous manifestations of HIV are remarkable for their breadth: a single patient may, over the course of their illness, develop inflammatory dermatoses, viral and fungal infections, neoplasms, and drug reactions, often simultaneously. Three features distinguish HIV-related skin disease from the same conditions in immunocompetent people and should always raise suspicion: lesions are frequently more extensive (widespread rather than localised), more atypical (in morphology, distribution, or behaviour), and more refractory (poorly responsive to standard therapy). A seborrhoeic dermatitis that covers the chest and back rather than just the scalp, a herpes zoster that crosses multiple dermatomes or recurs, or a molluscum that produces giant confluent lesions — each pattern is the same familiar disease made unfamiliar by failing immunity. Morphologically, HIV dermatoses span the full vocabulary of dermatology, and learning to scan for them systematically is the first diagnostic step.
The morphological categories you will encounter include:
- Papulosquamous and inflammatory: seborrhoeic dermatitis, psoriasis (new onset or sudden worsening), pruritic papular eruption (PPE), xerosis
- Papular and umbilicated: molluscum contagiosum (often giant or numerous), eosinophilic folliculitis
- Vesicular and ulcerative: herpes simplex (chronic, large, painful ulcers), herpes zoster (multidermatomal, recurrent)
- Plaques and tumours: Kaposi sarcoma (violaceous plaques and nodules), bacillary angiomatosis
- Mucosal: oral candidiasis (thrush), oral hairy leukoplakia, angular cheilitis
The rest of this module organises these conditions by the level of immunosuppression at which they typically appear, because that correlation is what makes the skin diagnostically powerful.
Immunopathogenesis: CD4 Strata and Dermatological Risk
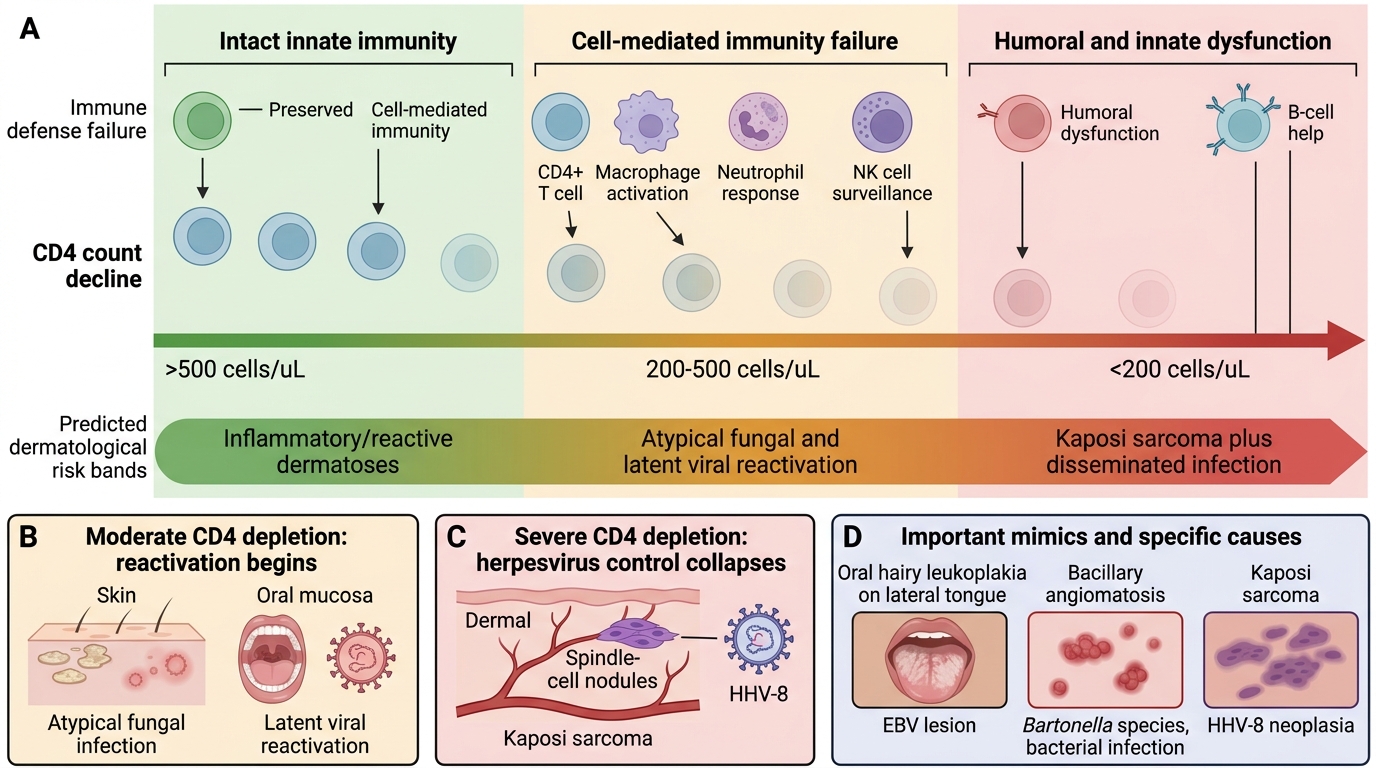
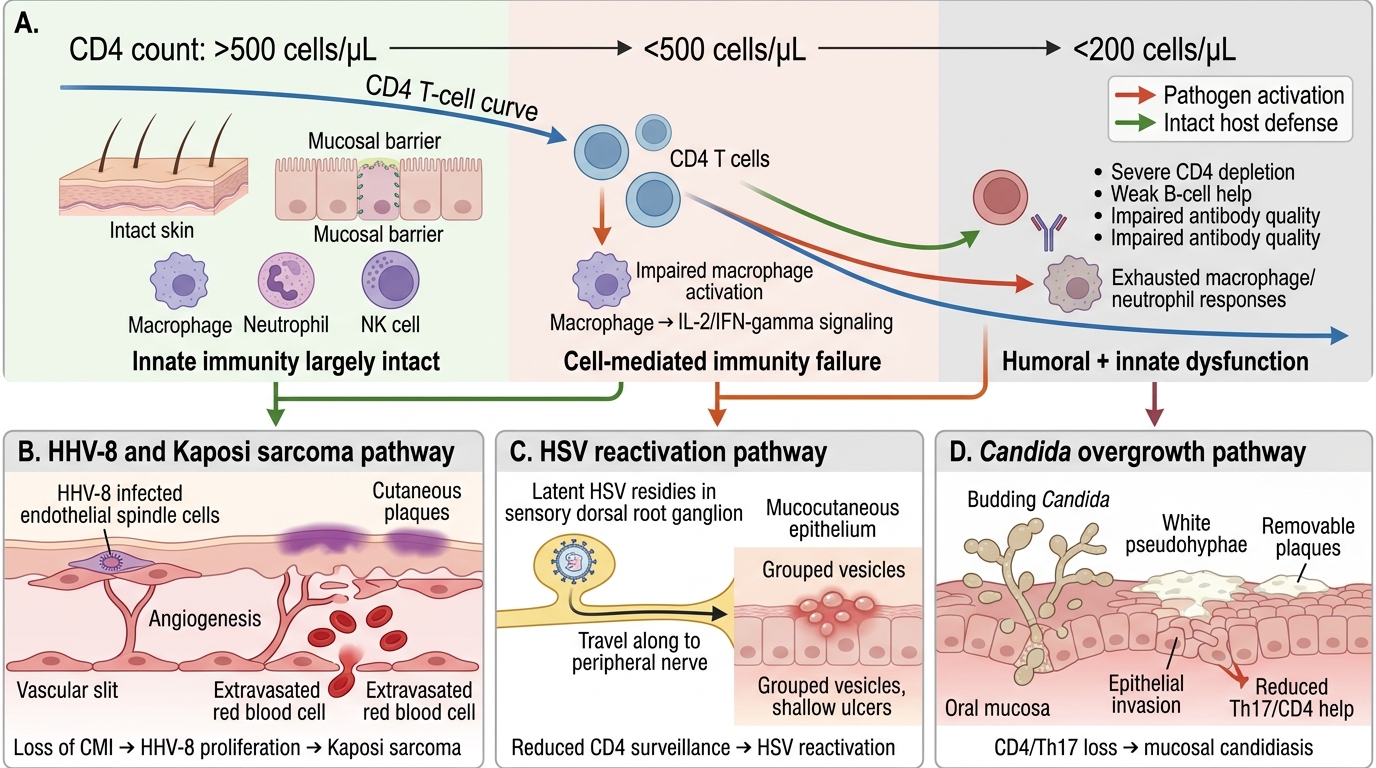
CD4 Strata and Dermatological Risk in HIV
The single most useful organising principle in HIV dermatology is that different dermatoses appear at predictable depths of immunosuppression, mirrored by the CD4 count. As CD4+ T cells are depleted, the immune defences fail in a roughly ordered sequence, and each new layer of failure unmasks a new set of opportunistic conditions. At relatively preserved counts the problems are largely inflammatory and reactive; at moderate depletion latent viruses and fungi begin to reactivate and behave atypically; at severe depletion the control of herpesviruses and other intracellular pathogens collapses, allowing neoplasia such as Kaposi sarcoma — driven by human herpesvirus-8 (HHV-8) — and disseminated, life-threatening infection. Some conditions are caused by specific reactivated viruses: oral hairy leukoplakia is an Epstein-Barr virus (EBV) lesion, and bacillary angiomatosis, an important mimic of Kaposi sarcoma at low counts, is in fact a bacterial infection caused by Bartonella species, not a virus. Understanding this graded immunopathology lets you reason from the skin to the likely CD4 stratum and back again.
CD4 Decline and Opportunistic Skin Infections in HIV
A simplified stratification (CD4 thresholds are approximate and overlap; confirm CD4-based clinical decisions against current NACO guidance):
- CD4 >500 cells/µL (early): seborrhoeic dermatitis, pruritic papular eruption, psoriasis flare
- CD4 200–500 cells/µL (moderate): oral hairy leukoplakia, extensive molluscum contagiosum, recurrent herpes zoster, mucocutaneous candidiasis, eosinophilic folliculitis
- CD4 <200 cells/µL (advanced): Kaposi sarcoma, extensive/chronic atypical herpes simplex, bacillary angiomatosis, disseminated cryptococcosis, severe giant molluscum
SELF-CHECK
A young adult presents with widespread, treatment-resistant seborrhoeic dermatitis involving the scalp, face, and central chest. At which CD4 stratum does seborrhoeic dermatitis most characteristically first appear, and what does its severity suggest?
A. Only at CD4 <200 cells/µL; it is an AIDS-defining illness
B. It can appear at relatively preserved CD4 (>500), but extensive/refractory disease should prompt HIV testing
C. Exclusively in patients with a normal CD4 count and no relation to HIV
D. Only after starting antiretroviral therapy as an IRIS phenomenon
Reveal Answer
Answer: B. It can appear at relatively preserved CD4 (>500), but extensive/refractory disease should prompt HIV testing
Seborrhoeic dermatitis is one of the earliest HIV-associated dermatoses and can occur at relatively preserved CD4 counts. However, when it is unusually extensive, severe, or refractory in a young adult, it should prompt consideration of underlying HIV and a CD4 count plus HIV serology.
Clinical Features of Common HIV-Associated Dermatoses
Clinical Features of Common HIV-Associated Dermatoses
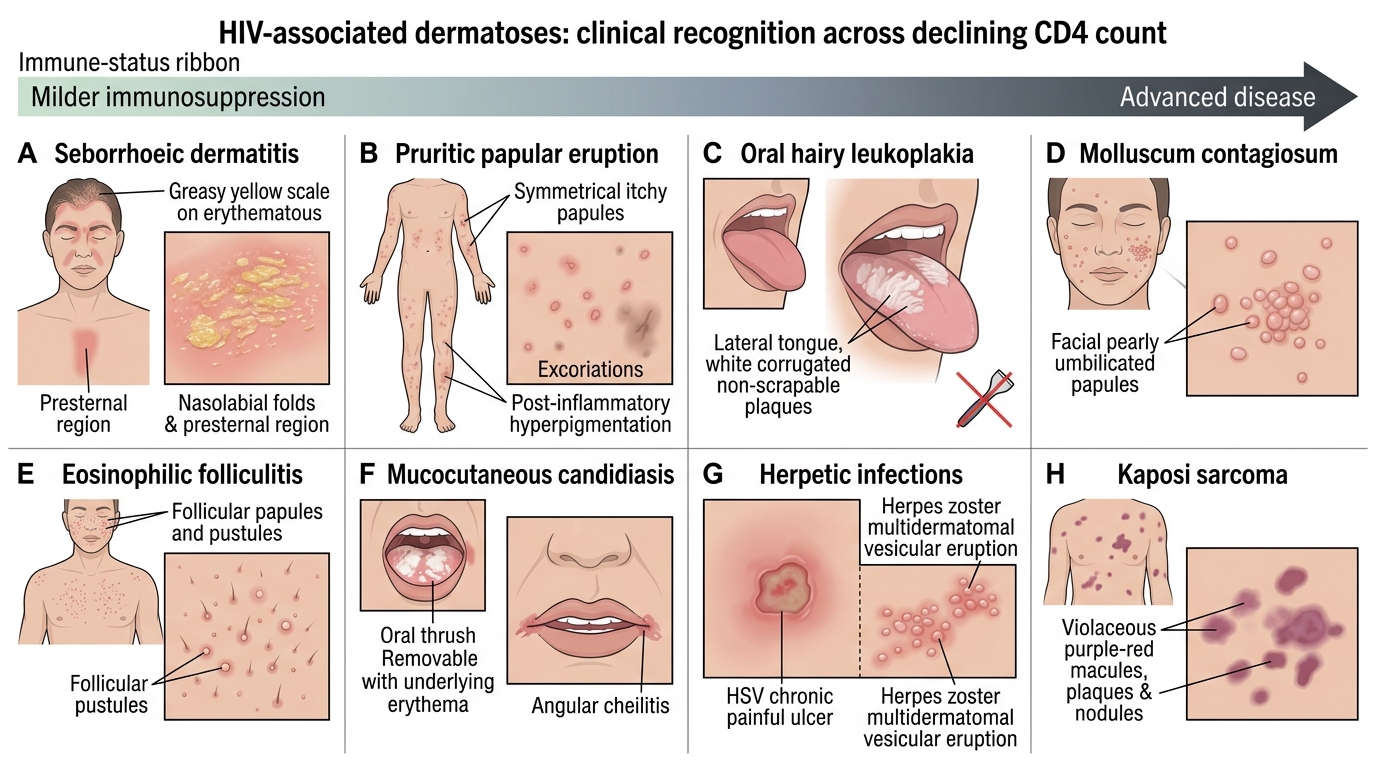
With the CD4 framework in mind, we can now describe the clinical features of the conditions you must be able to recognise, moving roughly from milder immunosuppression to more advanced disease. Seborrhoeic dermatitis presents as greasy, yellowish, erythematous scaling of the scalp, eyebrows, nasolabial folds, and presternal area, but in HIV it is more extensive and persistent. Pruritic papular eruption (PPE) is a common, intensely itchy, symmetrical eruption of small papules on the limbs and trunk, often with excoriations and post-inflammatory hyperpigmentation, and is an important marker of HIV in resource-limited settings. Oral hairy leukoplakia, an EBV-driven lesion, forms white corrugated (hairy) plaques on the lateral tongue that — unlike candidal thrush — cannot be scraped off. Molluscum contagiosum produces pearly, umbilicated papules that in HIV may be numerous, giant, or confluent, especially on the face. Eosinophilic folliculitis causes intensely pruritic follicular papules and pustules on the upper trunk and face. Mucocutaneous candidiasis appears as removable white plaques (thrush) with underlying erythema, or as angular cheilitis. Herpetic infections are especially important: herpes simplex may cause chronic, large, painful ulcers persisting beyond a month, and herpes zoster is often multidermatomal, severe, or recurrent. Kaposi sarcoma presents as violaceous (purple-red) macules, plaques, and nodules, frequently on the lower limbs, oral mucosa, and trunk, and is the most important HIV-associated cutaneous malignancy. It is worth emphasising that at low CD4 counts bacillary angiomatosis — friable vascular papules and nodules caused by Bartonella — can closely mimic Kaposi sarcoma and must be distinguished, because it is curable with antibiotics.
⚑ AI image — pending faculty review (auto-QA score 3/10; best of 3 attempts)
HIV Dermatoses by CD4 Stratum
SELF-CHECK
A patient with HIV has a white plaque on the lateral border of the tongue. Which feature best distinguishes oral hairy leukoplakia from oral candidiasis (thrush)?
A. Oral hairy leukoplakia can be easily scraped off, while thrush cannot
B. Oral hairy leukoplakia is caused by Candida, while thrush is caused by EBV
C. Oral hairy leukoplakia is a corrugated plaque that CANNOT be scraped off and is caused by EBV; thrush is removable and caused by Candida
D. Both are identical and cannot be distinguished clinically
Reveal Answer
Answer: C. Oral hairy leukoplakia is a corrugated plaque that CANNOT be scraped off and is caused by EBV; thrush is removable and caused by Candida
Oral hairy leukoplakia is an Epstein-Barr virus (EBV) lesion producing white, vertically corrugated 'hairy' plaques on the lateral tongue that cannot be scraped off. Candidal thrush, by contrast, is a removable white plaque (caused by Candida) leaving an erythematous base, and responds to antifungals.