Page 2 of 11
DR11.1 | Dermatologic Manifestations of HIV — SDL Guide (Part 2)
Differential Diagnosis and Laboratory Investigations
Differential Diagnosis and Laboratory Work-up in HIV Dermatology
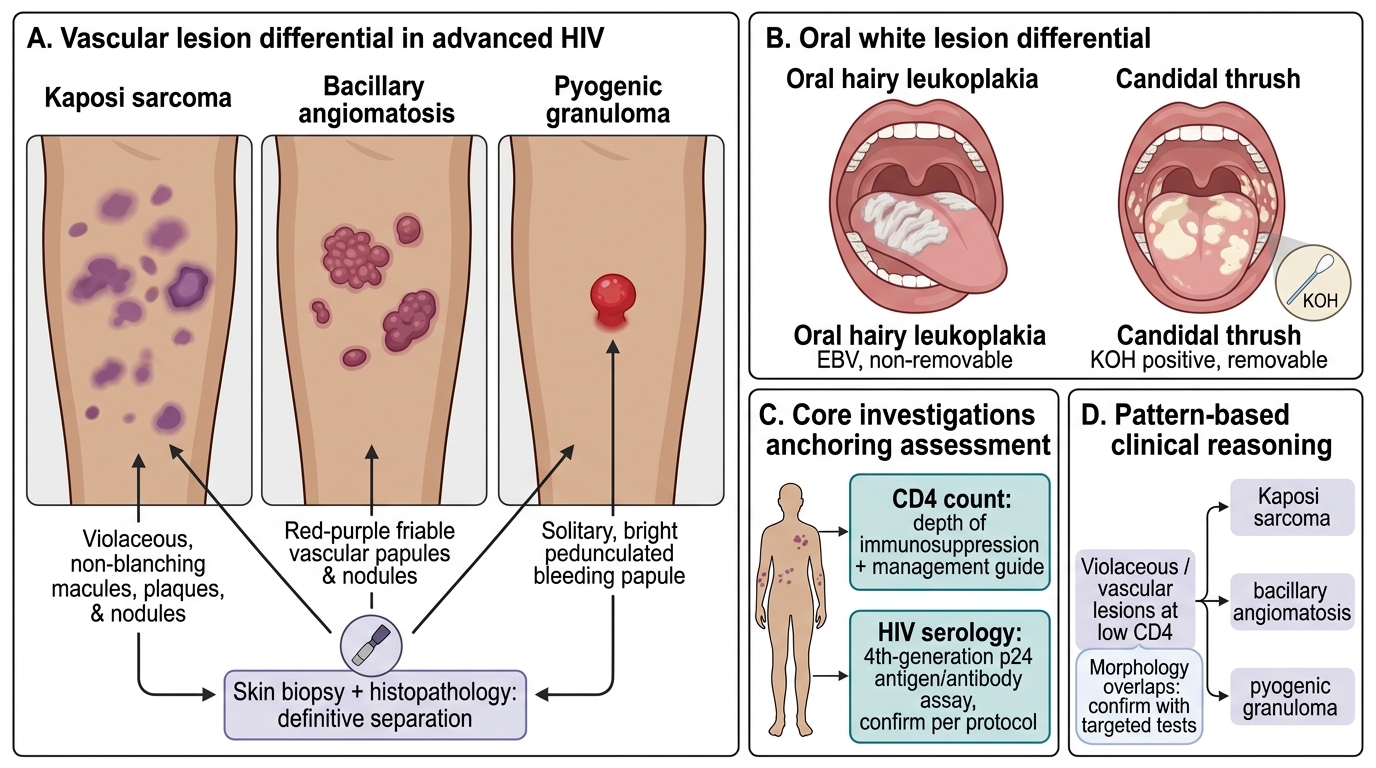
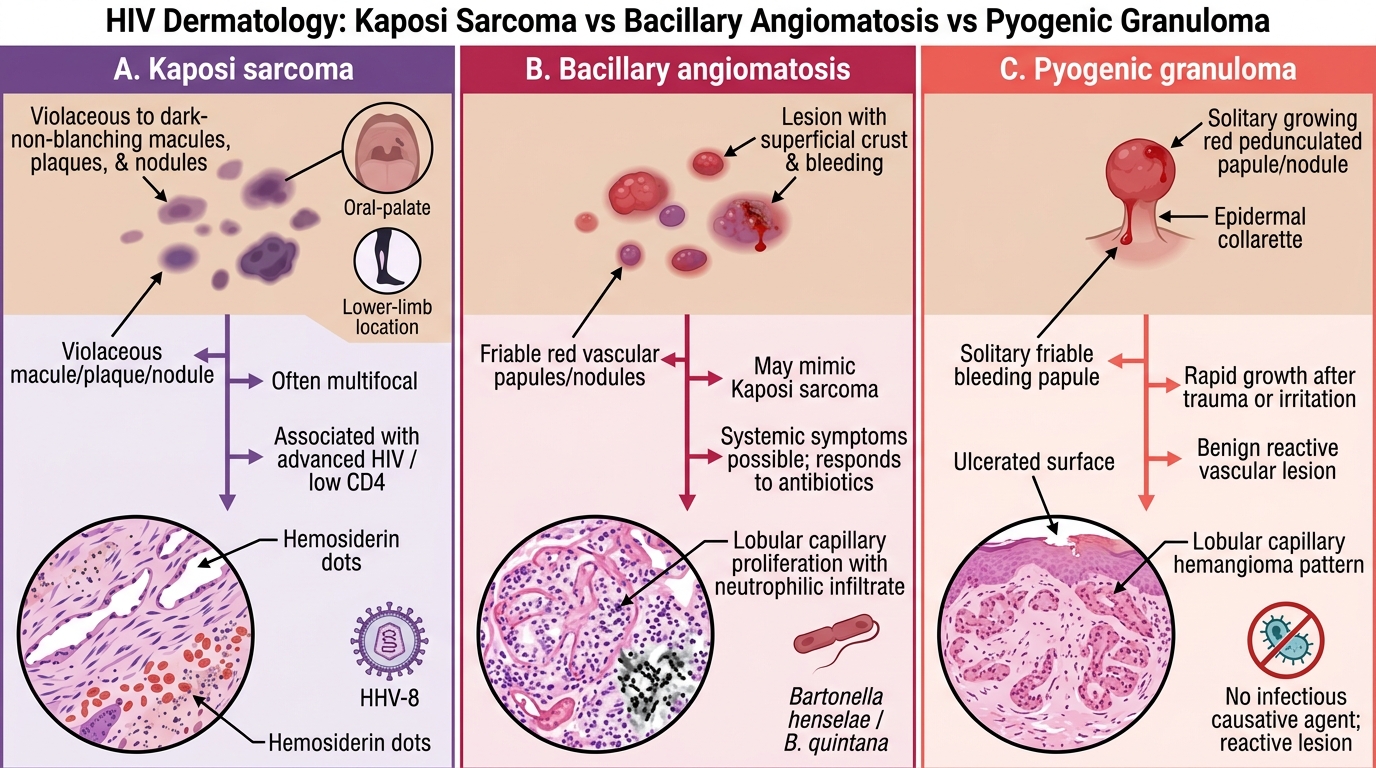
Because several HIV dermatoses mimic one another and because the morphology overlaps with non-HIV conditions, accurate diagnosis rests on combining the clinical pattern with targeted investigations. The most clinically important differential is that of violaceous or vascular lesions at low CD4 counts: Kaposi sarcoma (HHV-8 driven, a true vascular neoplasm), bacillary angiomatosis (Bartonella, bacterial and antibiotic-curable), and pyogenic granuloma (a benign reactive vascular proliferation) can all look similar, and a skin biopsy with histopathology is the definitive way to separate them. Oral white lesions require distinguishing oral hairy leukoplakia (EBV, non-removable) from candidal thrush (removable, KOH-positive). Beyond morphology, the two investigations that anchor every HIV dermatology assessment are the CD4 count, which both confirms the depth of immunosuppression suggested by the skin and guides management, and HIV serology — in current practice a fourth-generation combined p24 antigen/antibody assay, with confirmation per laboratory protocol. Additional, condition-specific tests round out the work-up.
HIV Vascular Lesion Differential
The core investigations to remember are:
- CD4 count — quantifies immunosuppression; correlates with the dermatosis pattern
- HIV serology — 4th-generation p24 antigen/antibody combination test, with confirmation per protocol
- Skin/mucosal biopsy with histopathology — definitive for Kaposi sarcoma vs bacillary angiomatosis vs pyogenic granuloma
- KOH mount — confirms Candida (pseudohyphae and budding yeast) and dermatophytes (septate hyphae)
- Tzanck smear — multinucleated giant cells in herpes simplex/zoster
- Syphilis serology (VDRL/TPHA) — co-infection is common and may alter morphology
Management Principles for HIV Dermatoses
Management Principles for HIV Dermatoses
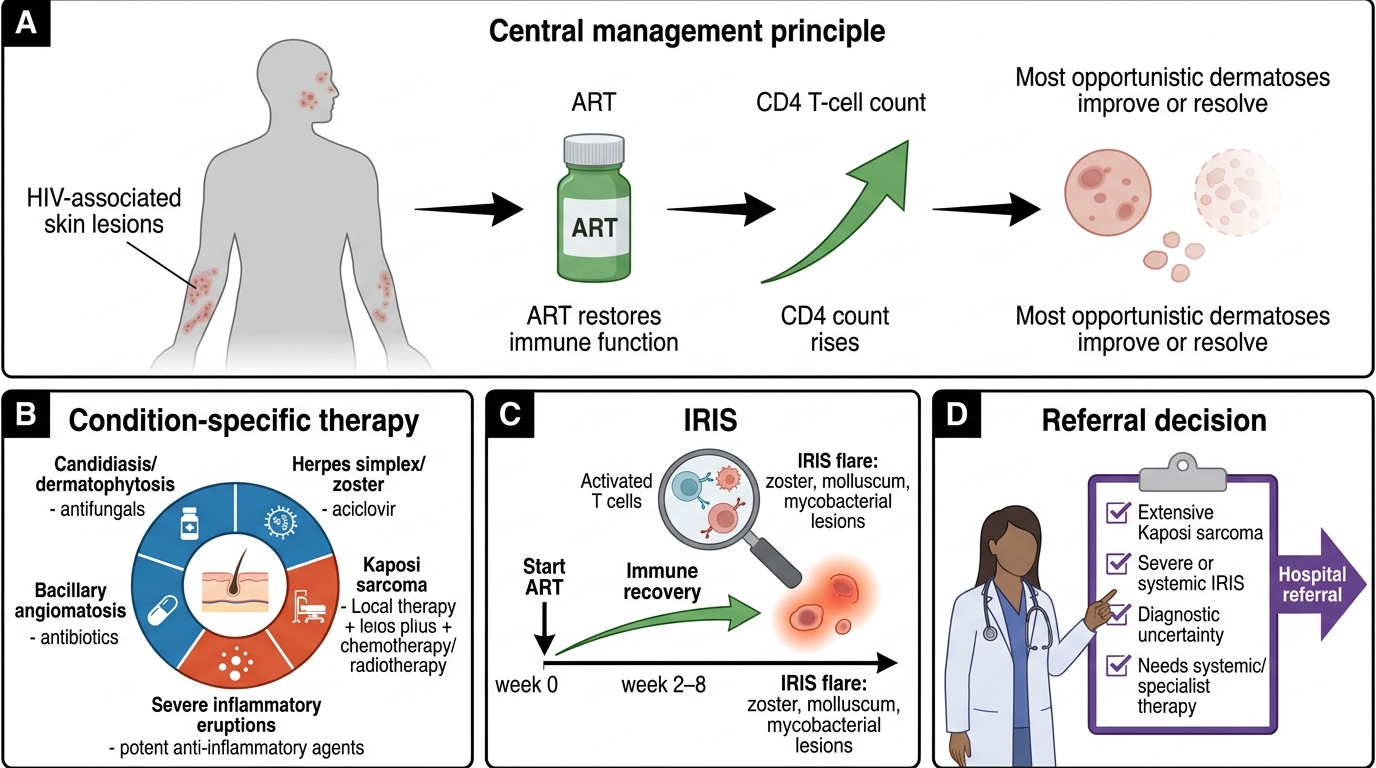
The single most important principle of managing HIV-associated dermatoses is that antiretroviral therapy (ART) is the cornerstone of treatment: by restoring CD4 counts and immune function, ART causes most opportunistic dermatoses to improve or resolve, and it prevents the progression to deeper, more dangerous conditions. Layered on top of ART is condition-specific therapy directed at the individual dermatosis — antifungals (topical or systemic) for candidiasis and dermatophytosis, antivirals such as aciclovir for herpes simplex and zoster, topical or intralesional therapy plus systemic chemotherapy or radiotherapy for Kaposi sarcoma, antibiotics for bacillary angiomatosis, and potent topical or systemic agents for severe inflammatory eruptions such as eosinophilic folliculitis and PPE. A crucial complication to anticipate is immune reconstitution inflammatory syndrome (IRIS): within weeks of starting ART, the recovering immune system can mount a vigorous inflammatory response against existing (sometimes subclinical) infections, paradoxically worsening conditions such as herpes zoster, molluscum, or mycobacterial lesions. IRIS is generally managed by continuing ART, treating the underlying infection, and adding anti-inflammatory therapy (corticosteroids) for severe flares — it is not a reason to stop ART. Finally, know when to refer: extensive Kaposi sarcoma, severe or systemic IRIS, diagnostic uncertainty, and any condition requiring biopsy, chemotherapy, or specialist HIV-care input should be referred to dermatology and the ART centre.
Key management points:
- ART is the foundation — most dermatoses improve with immune reconstitution
- Treat the specific condition: antifungals (candidiasis), aciclovir (HSV/HZ), chemotherapy/radiotherapy (Kaposi sarcoma), antibiotics (bacillary angiomatosis)
- Anticipate IRIS after ART initiation — continue ART, treat the infection, add steroids for severe flares
- Refer for biopsy-requiring lesions, extensive Kaposi sarcoma, severe IRIS, or diagnostic uncertainty
SELF-CHECK
Three weeks after starting antiretroviral therapy, a patient develops a florid, painful herpes zoster eruption. What is the most likely explanation and the appropriate action?
A. ART failure; stop ART immediately
B. Immune reconstitution inflammatory syndrome (IRIS); continue ART, treat the zoster, and add steroids if severe
C. A new HIV infection; restart testing from baseline
D. Drug allergy to the antiretrovirals; switch the entire regimen
Reveal Answer
Answer: B. Immune reconstitution inflammatory syndrome (IRIS); continue ART, treat the zoster, and add steroids if severe
This is immune reconstitution inflammatory syndrome (IRIS): the recovering immune system mounts an inflammatory response against existing (latent or subclinical) infection, here varicella-zoster. ART should be CONTINUED; the zoster is treated with antivirals, and corticosteroids are added for severe inflammation. IRIS is not a reason to stop ART.
Self-Assessment: HIV and the Skin
⚑ AI image — pending faculty review (auto-QA score 6/10; best of 3 attempts)
HIV Dermatology Self-Assessment Map
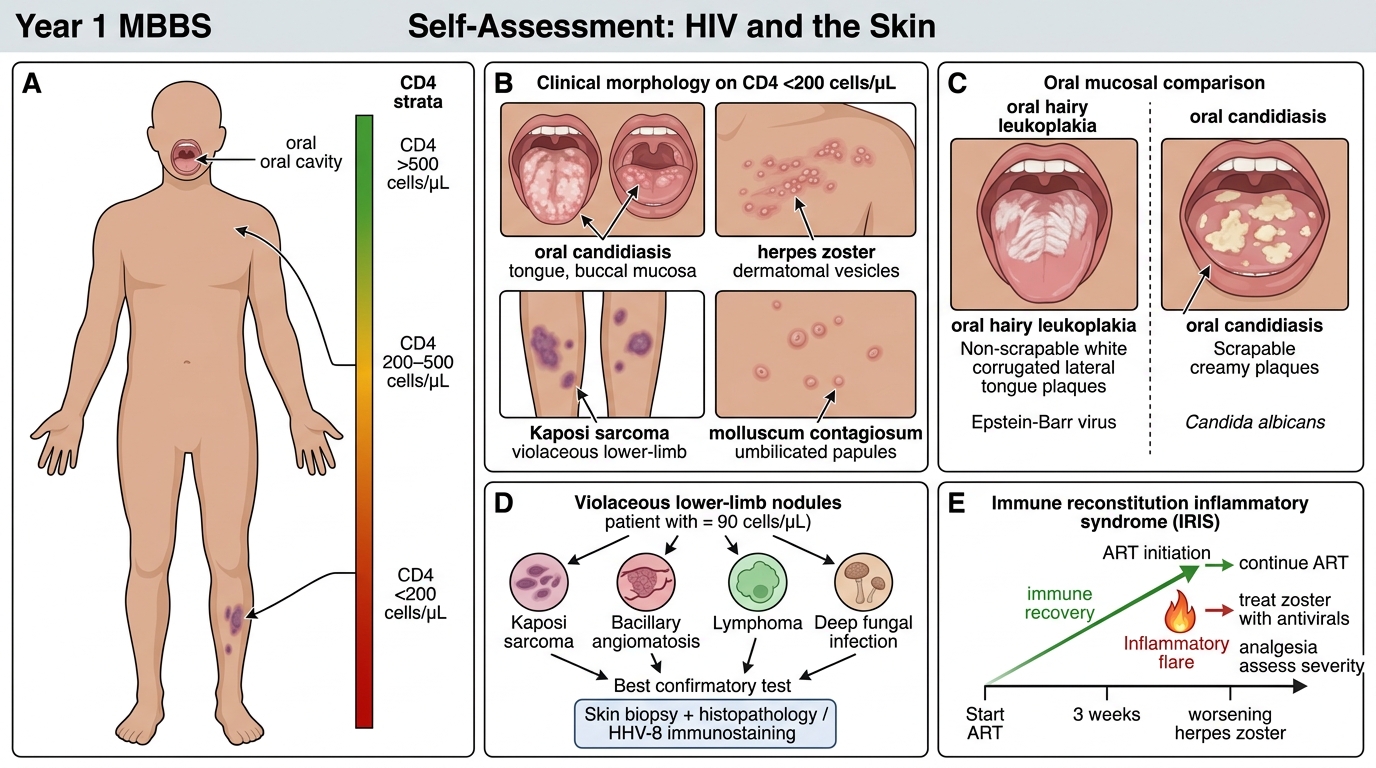
Having worked through the morphology, immunopathology, diagnosis, and management of HIV-associated dermatoses, it is worth consolidating the reasoning before moving on. The central skill you should now possess is the ability to look at a skin or mucosal finding, place it within a likely CD4 stratum, choose the right confirmatory investigation, and outline management with antiretroviral therapy at its centre. Test yourself against the following prompts, reasoning aloud from the clinical features to the diagnosis and then to the next step, rather than simply recalling lists. If any prompt leaves you uncertain, return to the relevant section above and re-examine the link between the dermatosis and the depth of immunosuppression it reflects, since that single correlation underpins almost every diagnostic and management decision in this domain.
Work through these self-check questions:
- Name four dermatoses that characteristically occur at CD4 <200 cells/µL, and state one investigation for each.
- A patient with HIV has violaceous nodules on the lower limb at a CD4 of 90 cells/µL — list your differential diagnosis and the single best confirmatory test.
- Distinguish oral hairy leukoplakia from oral candidiasis on clinical grounds and by causative organism.
- A patient develops worsening herpes zoster three weeks after starting ART — explain the mechanism and the correct management.
- Outline why antiretroviral therapy is described as the cornerstone of managing HIV dermatoses.
CLINICAL PEARL
The skin lets you estimate the CD4 count before the laboratory does. A young adult with extensive, refractory seborrhoeic dermatitis or pruritic papular eruption is likely in an early stratum (CD4 often >500), whereas the appearance of violaceous Kaposi plaques, giant molluscum, chronic herpetic ulcers, or bacillary angiomatosis signals advanced immunosuppression (CD4 <200) and an urgent need for ART and opportunistic-infection prophylaxis. Remember the two great mimics at low counts: Kaposi sarcoma (HHV-8, neoplastic) versus bacillary angiomatosis (Bartonella, bacterial and curable) — never treat a presumed Kaposi lesion without considering a biopsy, because mistaking a curable bacterial infection for an incurable tumour, or vice versa, changes the patient's life.