Page 13 of 23
DR9.6 | Leprosy Complications Disability and Stigma Counselling — SDL Guide
Learning Objectives
- Recognise the visible complications of leprosy and link each deformity to the nerve whose damage causes it
- Grade leprosy disability using the WHO 0-1-2 scale for the eye, hand, and foot
- Plan the management of common complications, including plantar ulcer care, lagophthalmos, and indications for reconstructive surgery and physiotherapy
- Counsel a patient about disability prevention, the curability and non-infectivity of treated leprosy, and the stigma associated with the disease
INSTRUCTIONS
The tragedy of leprosy is not the infection — which is curable — but the disability and stigma that follow nerve damage. The visible deformities of leprosy, and the social rejection they provoke, are what destroy livelihoods, marriages, and dignity. A clinician who can prevent, grade, and manage these complications, and who can counsel a patient and family with knowledge and compassion, changes the entire trajectory of a person's life. This module teaches you to recognise the complications and trace each to its responsible nerve, to grade disability on the WHO scale, to manage plantar ulcers and eye complications and know when to refer for surgery, and — crucially — to counsel patients about disability prevention and the deeply rooted stigma that still surrounds this disease.
References
- Neena Khanna. Illustrated Synopsis of Dermatology and Sexually Transmitted Diseases, 5th ed. Ch: Leprosy — Deformities, Disability and Rehabilitation (textbook)
- National Leprosy Eradication Programme (NLEP) — Disability Prevention and Medical Rehabilitation (DPMR) Guidelines; WHO disability grading (guideline)
- IADVL Textbook of Dermatology, 4th ed. Section: Leprosy — Complications, Reconstructive Surgery and Stigma (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 40-year-old man, cured of leprosy three years ago, comes to you not for his skin but because he has lost his job and his wife has left him. He cannot fully close his right eye, his right hand has clawed, and there is a painless ulcer on the sole of his foot that he never noticed forming because the skin there feels nothing. None of these is the infection — the bacilli are long dead. They are the legacy of nerve damage that was never prevented, and the social catastrophe around him is the legacy of stigma. He tells you, quietly, that his neighbours believe leprosy is a curse and a punishment, and that he believes it too. In this single patient you can see the two faces of leprosy's true burden: the physical deformities that follow damaged nerves, and the crushing stigma that no antibiotic can treat. Managing him means treating his ulcer and his eye — but it also means giving him back the truth that he is cured, not cursed, and not infectious.
WHY THIS MATTERS
This module matters because the lasting harm of leprosy comes from its complications and its stigma, not from the infection you have already learned to cure. As a clinician you will meet patients whose nerve damage has produced clawed hands, foot drop, plantar ulcers, and eye complications, and your ability to grade, manage, and prevent these directly determines whether they keep their hands, feet, and sight. Just as importantly, you will be the person who must counsel them and their families — to explain that treated leprosy is cured and non-infectious, to dismantle the myths of curse and contagion that drive social rejection, and to connect them with rehabilitation and their legal rights. Compassionate, knowledgeable counselling is a clinical skill with as much impact on a leprosy patient's life as any drug, and it is a skill this module builds deliberately.
RECALL
Before beginning, recall from the neurological-examination module the map of nerves to deformities: the ulnar nerve (claw hand of the ring and little fingers), the median nerve (clawing of the index and middle fingers and thenar wasting), the common peroneal nerve (foot drop), and the posterior tibial nerve (anaesthesia of the sole, predisposing to plantar ulcers, with clawing of the toes). Recall from Anatomy that the facial nerve (its zygomatic branch) supplies the orbicularis oculi, so its damage prevents full eye closure — lagophthalmos. Recall the WHO disability grading scale (Grade 0 = no anaesthesia or deformity; Grade 1 = anaesthesia only; Grade 2 = visible deformity/damage), applied separately to each eye, hand, and foot. These foundations let you trace every complication back to its cause and grade it consistently.
The Face of Leprosy — Visible Complications and Their Impact
Visible Complications of Leprosy
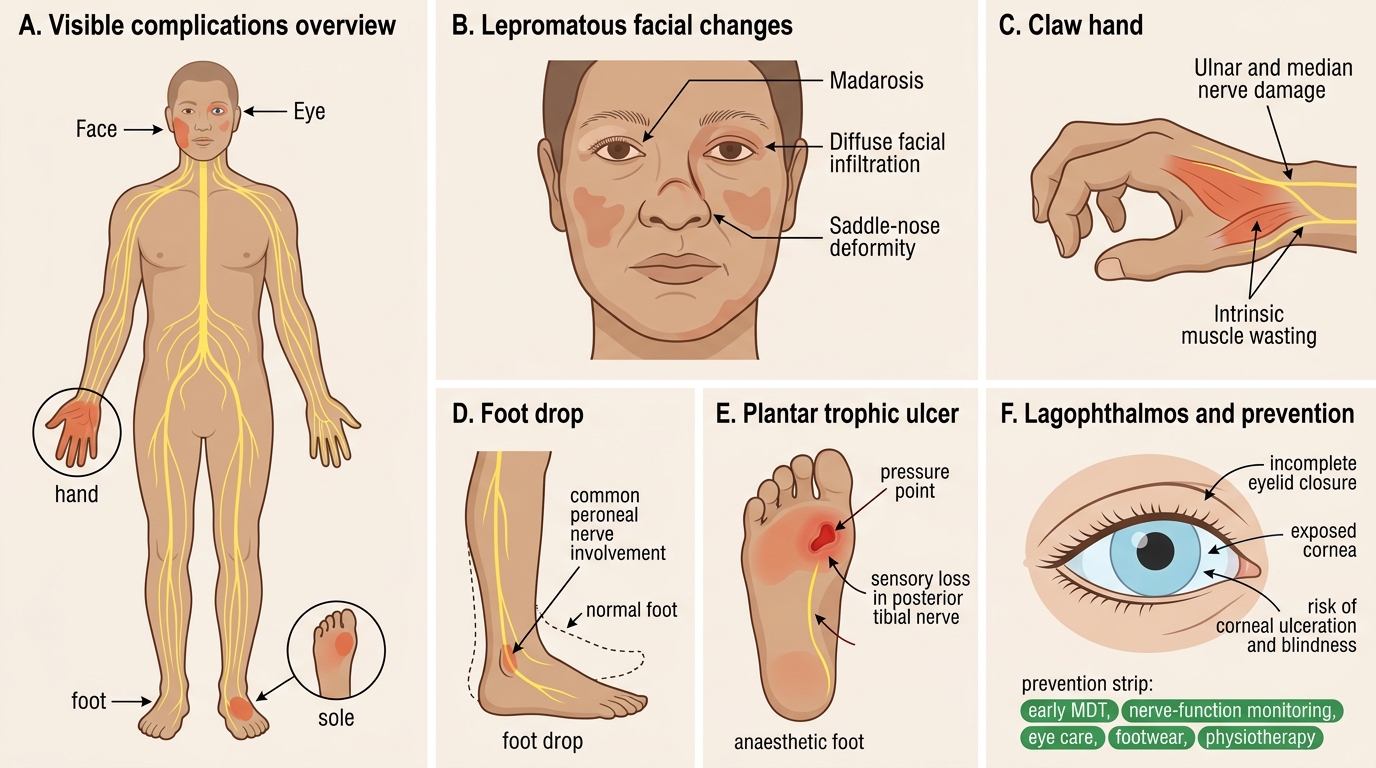
The complications of leprosy present as a recognisable set of visible deformities, and learning to read them is the first step in managing the disease's true burden. The most consequential are the consequences of peripheral nerve damage: claw hand (from ulnar and/or median nerve damage), foot drop (from common peroneal nerve damage), plantar (trophic) ulcers on the anaesthetic sole (from posterior tibial nerve damage), and lagophthalmos with its risk of corneal damage and blindness (from facial nerve damage). In addition, lepromatous disease can cause madarosis (loss of eyebrows), a depressed saddle-nose deformity from destruction of the nasal cartilage, and other features of diffuse infiltration. Each of these is a clinical sign you must be able to recognise at a glance.
What makes these complications so devastating is their combined physical and social impact. A clawed, insensate hand cannot work; a dropped foot and an ulcerated sole cannot walk safely; an eye that will not close goes blind. Layered on top of the physical disability is the profound stigma that the visible deformities provoke — historically leprosy patients have been shunned, segregated, and abandoned, and the deformities are precisely what mark a person out for that rejection. This is why the entire thrust of modern leprosy care is to PREVENT these complications through early treatment and nerve-function monitoring, and to manage and rehabilitate them when they have occurred.
Complications to recognise:
- Claw hand (ulnar ± median nerve), foot drop (common peroneal nerve), plantar ulcer (posterior tibial nerve, anaesthetic sole), lagophthalmos (facial nerve → corneal risk).
- Madarosis and saddle nose in lepromatous disease.
- These visible deformities carry both physical disability and the heavy social stigma of the disease.
Pathomechanisms of Nerve Damage Leading to Disability
Leprosy Nerve Damage: From Bacillus to Disability
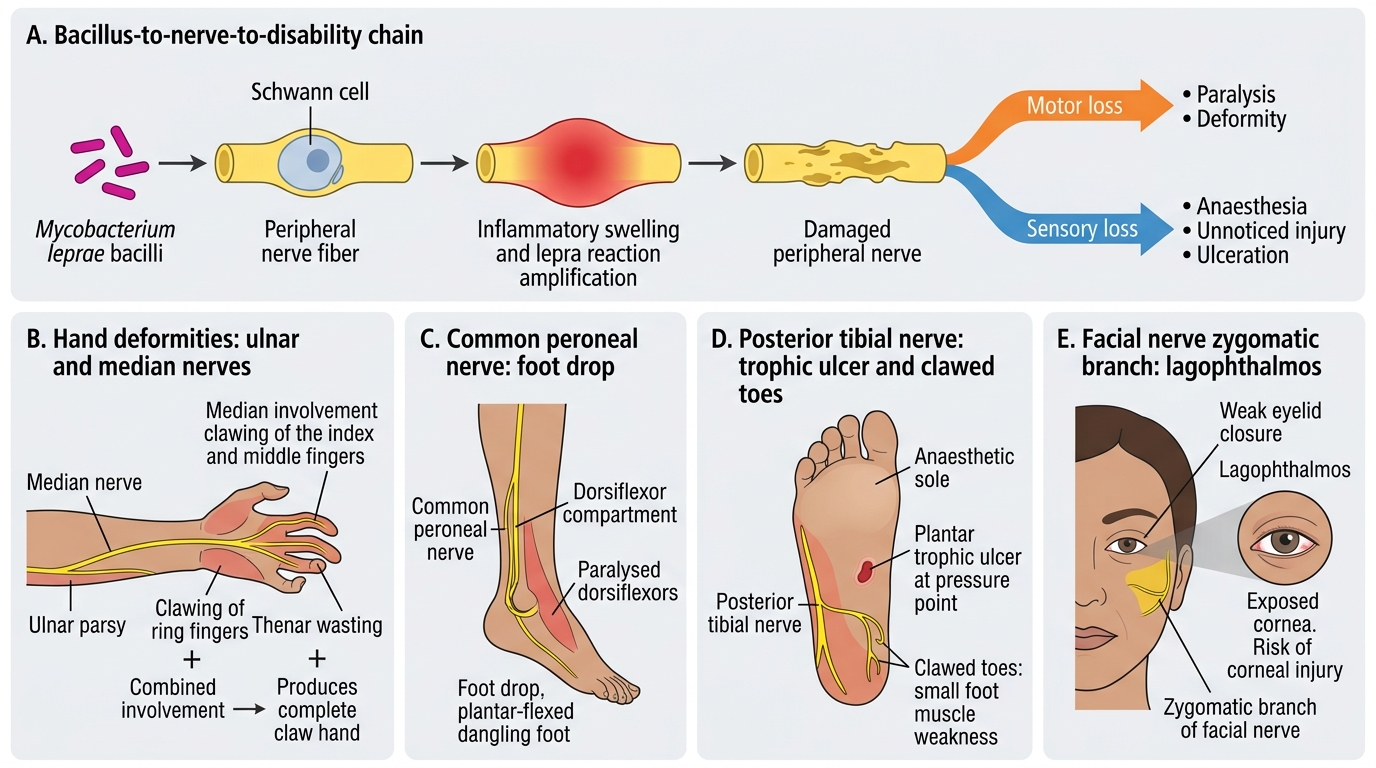
Every leprosy deformity can be traced to a specific damaged nerve, and understanding this chain — from bacillus to nerve to deformity — lets you predict, prevent, and rationally manage disability rather than merely cataloguing it. The underlying mechanism is that M. leprae invades Schwann cells, and the resulting inflammation (often amplified by lepra reactions) damages the nerve, producing both motor loss (paralysis of the muscles it supplies, which gives the visible deformity) and sensory loss (anaesthesia in its territory, which silently permits injury and ulceration). The two consequences are different and complementary: motor loss deforms, sensory loss ulcerates.
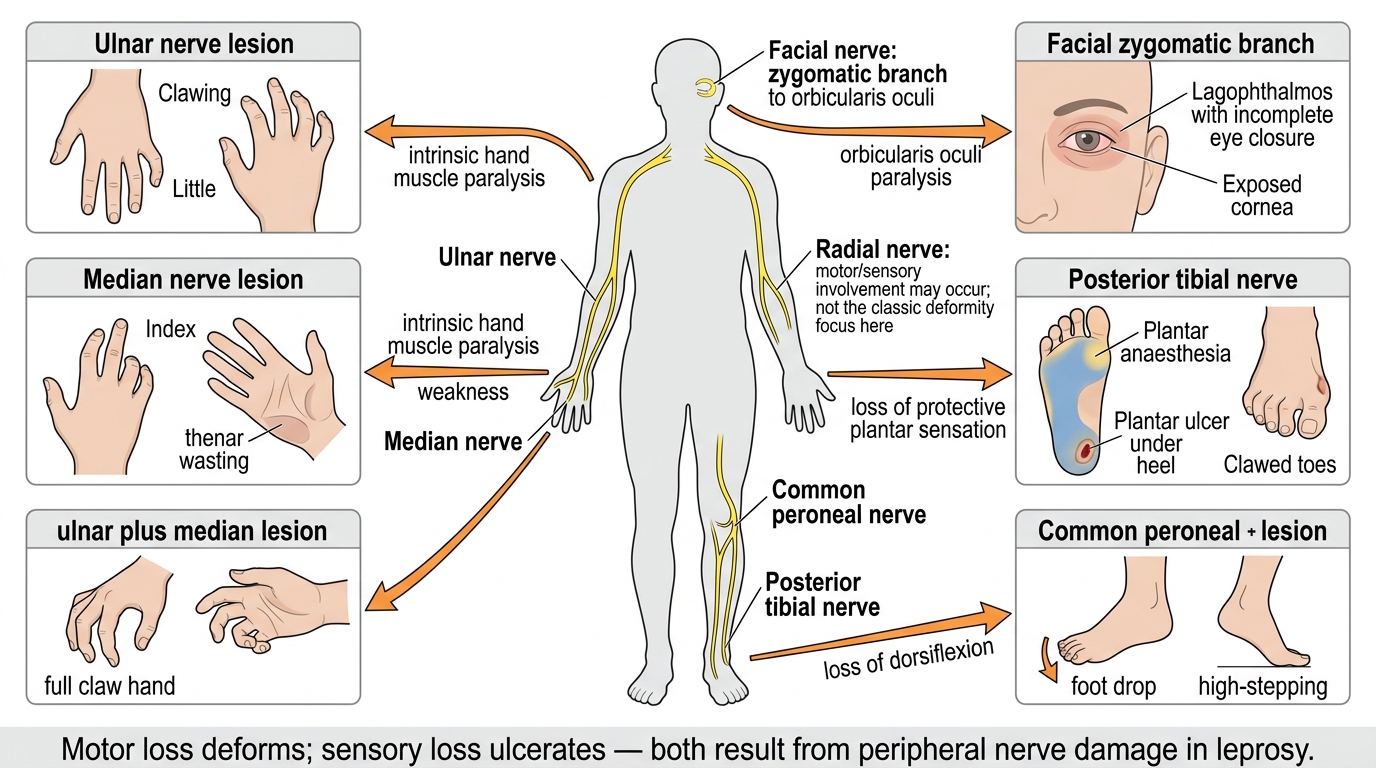
Mapping each nerve to its deformity makes the pattern memorable. Ulnar nerve damage paralyses the intrinsic muscles, clawing the ring and little fingers; median nerve damage adds clawing of the index and middle fingers and thenar wasting, and combined ulnar-median damage produces a complete claw hand. Common peroneal nerve damage paralyses the dorsiflexors, causing foot drop. Posterior tibial nerve damage anaesthetises the sole and weakens the small foot muscles, so that unnoticed pressure and injury produce a plantar (trophic) ulcer and clawed toes. Facial nerve (zygomatic branch) damage weakens eye closure, causing lagophthalmos and exposing the cornea. These findings are then graded with the WHO disability scale — Grade 0 (no anaesthesia or deformity), Grade 1 (anaesthesia only), Grade 2 (visible deformity or damage) — applied separately to each eye, hand, and foot.
Leprosy: Peripheral Nerve Lesions and Deformities
Nerve-to-deformity logic:
- Motor loss deforms; sensory loss ulcerates — both follow from the same nerve damage.
- Ulnar → claw (ring+little); median → claw (index+middle) + thenar wasting; peroneal → foot drop; posterior tibial → plantar ulcer + clawed toes; facial → lagophthalmos.
SELF-CHECK
A leprosy patient cannot fully close the right eye, leaving the cornea exposed. Which nerve is damaged, and what is the WHO disability grade for that eye?
A. Trigeminal nerve; WHO Grade 1
B. Facial nerve (zygomatic branch); WHO Grade 2, because there is visible deformity/damage (lagophthalmos)
C. Oculomotor nerve; WHO Grade 0
D. Posterior tibial nerve; WHO Grade 1
Reveal Answer
Answer: B. Facial nerve (zygomatic branch); WHO Grade 2, because there is visible deformity/damage (lagophthalmos)
Inability to close the eye (lagophthalmos) results from damage to the facial nerve (its zygomatic branch), which supplies the orbicularis oculi. Because there is now VISIBLE deformity/damage with corneal exposure, the WHO disability grade for that eye is Grade 2 (Grade 1 would be loss of corneal sensation without visible damage; Grade 0 is normal). The trigeminal nerve carries corneal sensation, not eyelid closure; the posterior tibial nerve is a foot nerve. Lagophthalmos is sight-threatening and warrants prompt eye protection and ophthalmology referral.
Clinical Assessment of Disability and Deformity
Provided image
Assessing disability systematically means examining the eye, the hand, and the foot in turn and converting your findings into a WHO grade for each, because consistent grading is what drives management decisions and tracks change over time. The assessment is built on the neurological examination you have already learned, now focused on the functional consequences. For the eye, test the ability to close the lids fully (look for lagophthalmos), assess corneal sensation, and check visual acuity — an eye that cannot close or has corneal damage is at risk of blindness. For the hand, look for clawing and wasting, map sensory loss (especially loss of protective sensation in the palm and fingertips), grade muscle power, and inspect for trophic ulcers or resorption of digits. For the foot, test protective sensation on the sole (a monofilament is ideal), look for foot drop, clawed toes, and — critically — examine the sole for plantar ulcers and assess their depth.
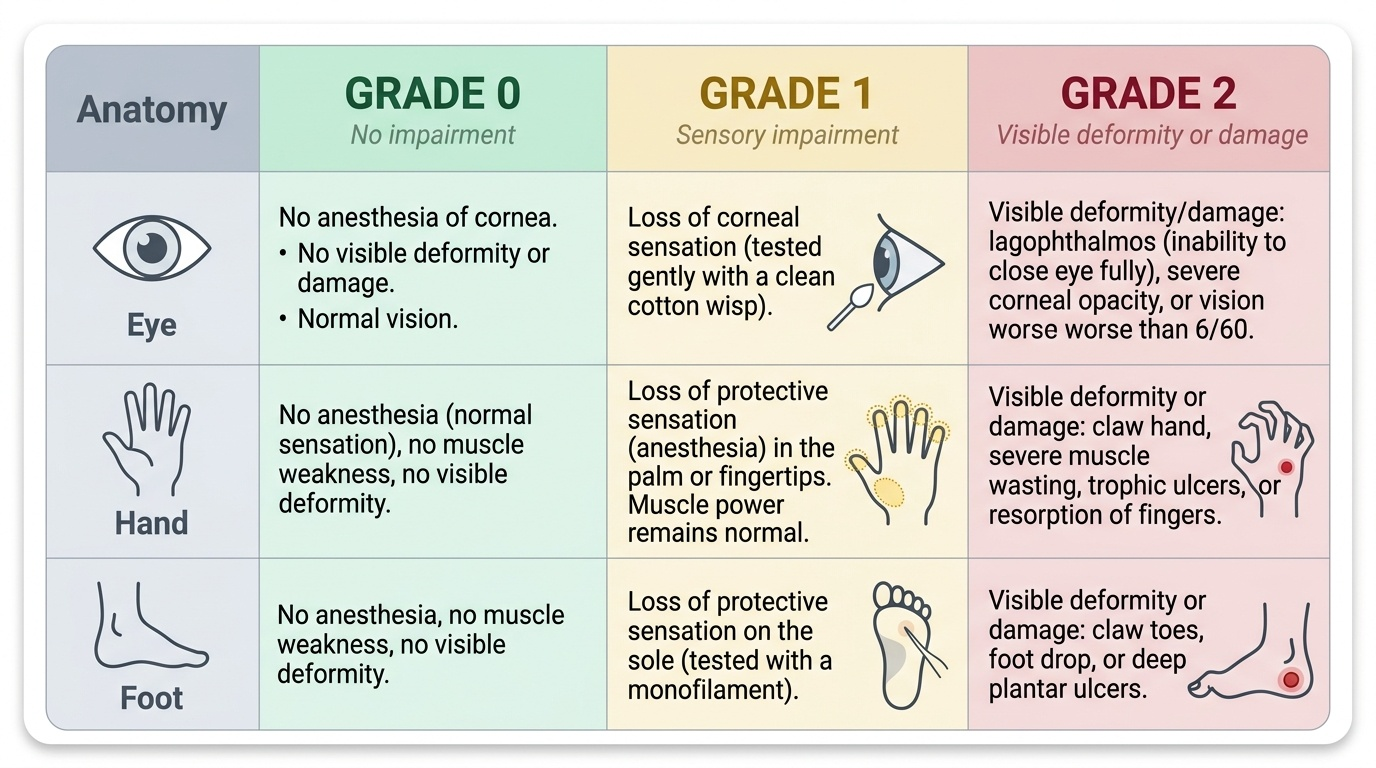
The WHO disability grade is then assigned separately to each eye, hand, and foot: Grade 0 = no anaesthesia and no visible deformity/damage; Grade 1 = loss of protective sensation (anaesthesia) only, without visible deformity; Grade 2 = visible deformity or damage present (lagophthalmos or corneal damage in the eye; claw, ulcer, or resorption in the hand; foot drop or plantar ulcer in the foot). Documenting these grades at baseline and at each visit lets you detect deterioration early and is the basis of the NLEP disability indicators. Plantar ulcers are additionally graded by depth (superficial, deep to tendon/joint, or with underlying osteomyelitis) to guide their management.
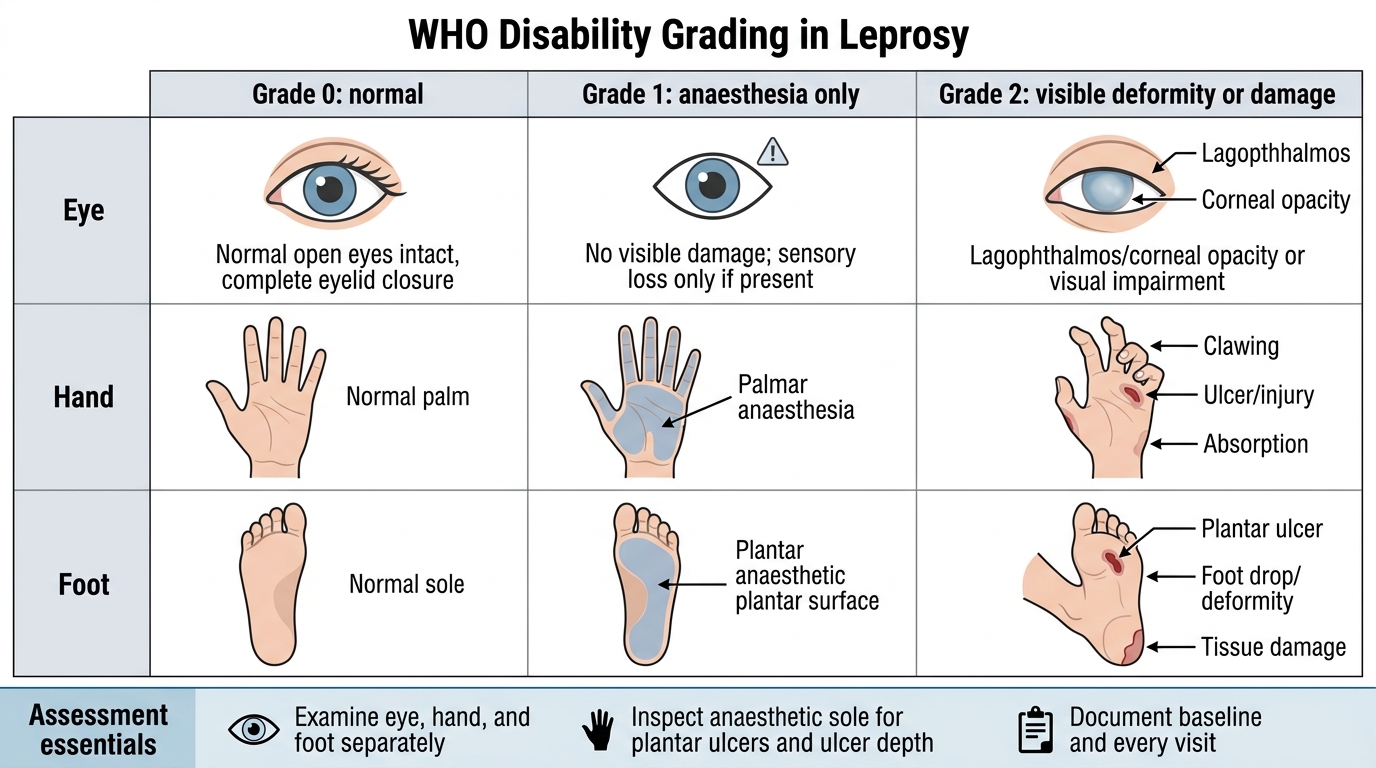
WHO Disability Grading in Leprosy
Assessment essentials:
- Examine eye, hand, and foot separately; grade each on the WHO 0-1-2 scale (0 normal; 1 anaesthesia only; 2 visible deformity/damage).
- Always inspect the anaesthetic sole for plantar ulcers and grade ulcer depth.
- Document grades at baseline and every visit to catch deterioration early.