Page 14 of 23
DR9.6 | Leprosy Complications Disability and Stigma Counselling — SDL Guide (Part 2)
Investigations and Triggers for Surgical/Specialist Referral
Investigations and Referral Triggers in Leprosy Disability
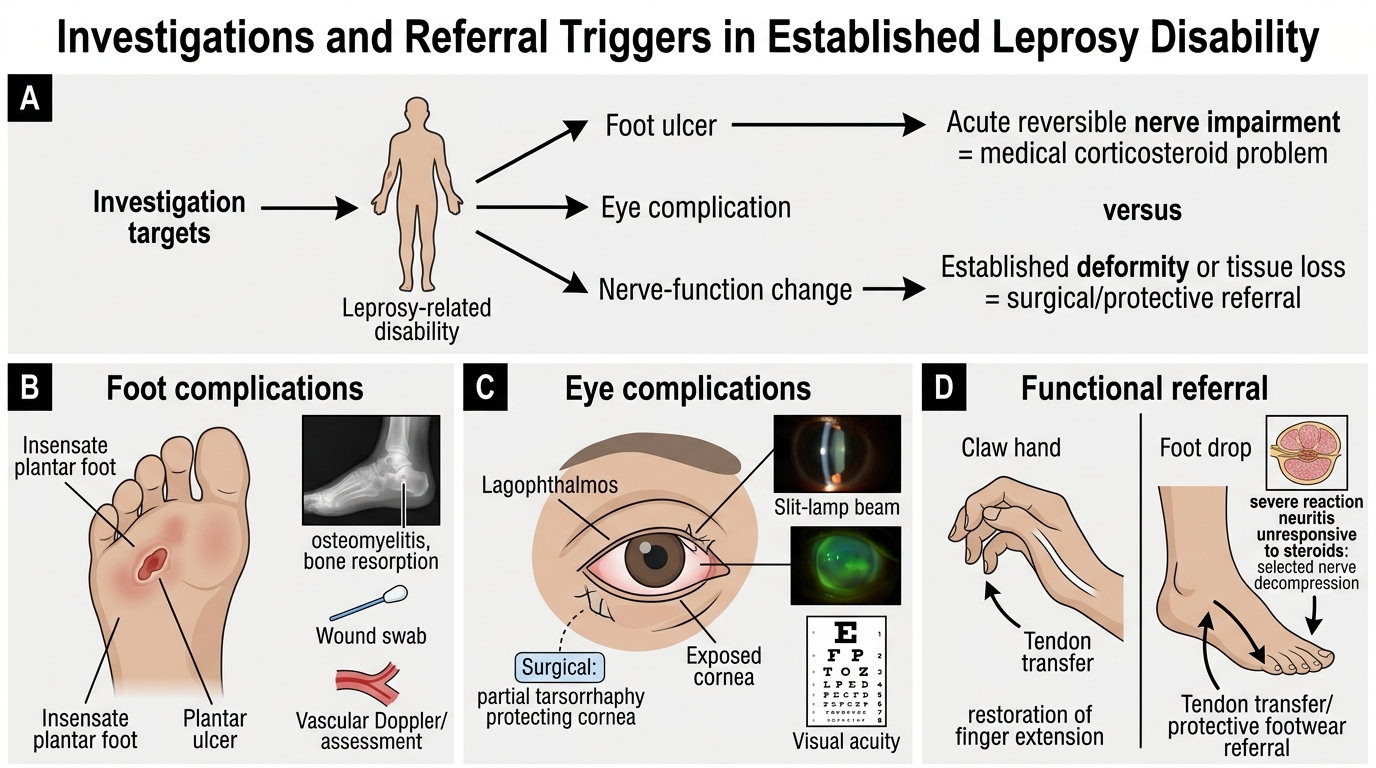
Investigations in established leprosy disability are targeted at the complications themselves, and recognising the triggers for specialist referral is what prevents a manageable problem from becoming a catastrophic one. For a plantar ulcer, a radiograph of the foot is the key investigation to detect underlying osteomyelitis or bone resorption, and a wound swab guides antibiotics if there is secondary infection; vascular assessment is occasionally needed to exclude an ischaemic component. For an eye complication, ophthalmology assessment (slit-lamp examination, corneal staining, acuity) determines the threat to sight. Nerve-function assessment continues throughout, because new or worsening impairment may still be reaction-driven and steroid-responsive.
Knowing when to refer is a core competency. Reconstructive and protective surgery has defined roles: tarsorrhaphy (partial lid closure) for lagophthalmos threatening the cornea; tendon transfer to correct established claw hand or foot drop and restore function; nerve decompression in selected cases of severe reaction neuritis unresponsive to steroids; and procedures such as flap cover for recalcitrant plantar ulcers. Physiotherapy and protective footwear referral are indicated for any insensate or deformed foot to prevent (further) ulceration. The general principle is that acute, reversible nerve impairment is a medical (corticosteroid) problem, whereas established fixed deformity is a surgical and rehabilitative one — and recognising which you are facing directs the referral.
Investigations and referral triggers:
- Plantar ulcer: X-ray (osteomyelitis/resorption), wound swab (infection); refer for surgery if deep/non-healing.
- Eye: ophthalmology assessment; tarsorrhaphy if lagophthalmos threatens the cornea.
- Fixed deformity (claw hand, foot drop): tendon transfer; nerve decompression for selected steroid-resistant neuritis.
- Any insensate/deformed foot: physiotherapy + protective (MCR) footwear.
Management of Complications and Stigma Counselling
Provided image
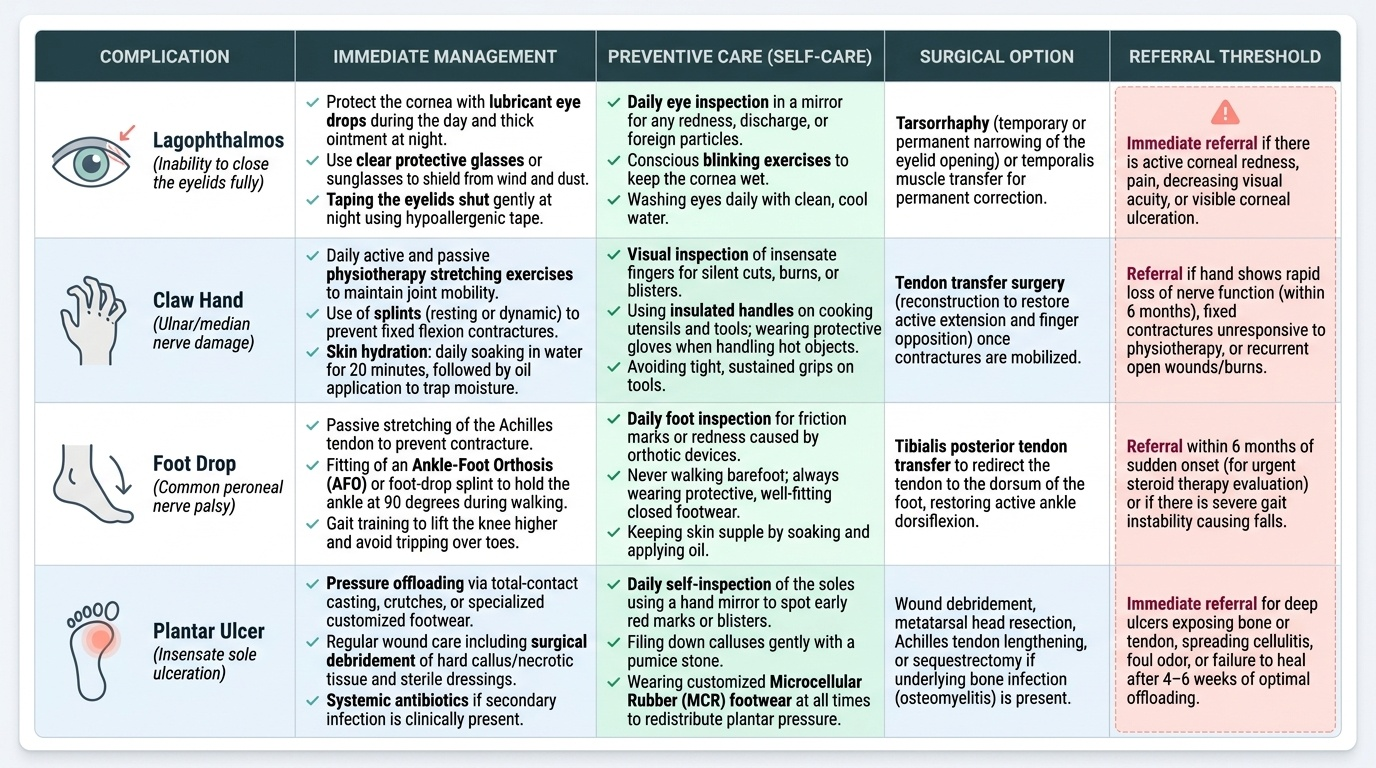
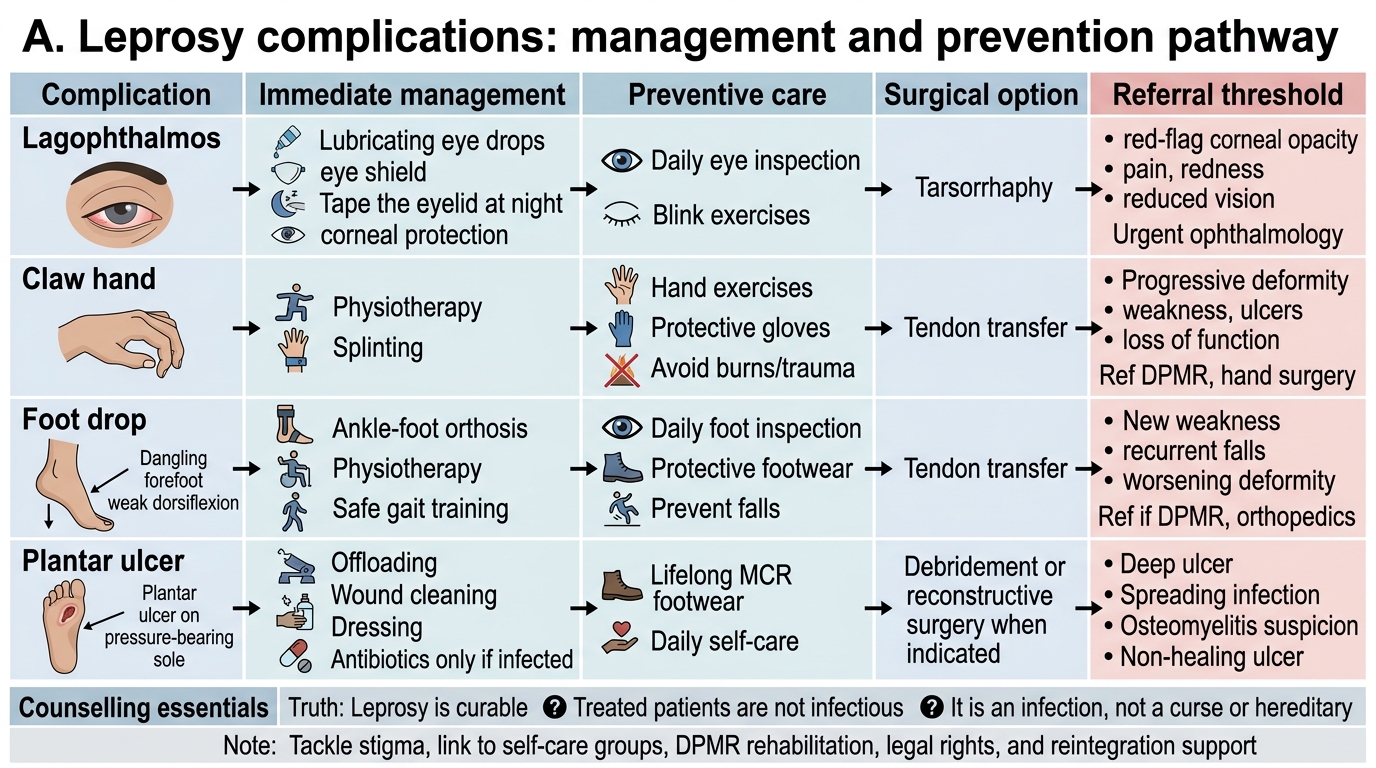
Managing leprosy complications combines practical wound and deformity care with something no surgery can provide — informed, compassionate counselling that addresses the stigma at the heart of the disease's burden. On the physical side, a plantar ulcer is managed by offloading (rest, total-contact casting or protective footwear to remove pressure from the ulcer), wound care with debridement and dressings, antibiotics if secondarily infected, and long-term microcellular rubber (MCR) footwear to redistribute plantar pressure and prevent recurrence. Lagophthalmos is managed by protecting the cornea (lubricant drops, protective glasses, taping at night) and surgical tarsorrhaphy when needed. A claw hand is managed with physiotherapy, splinting to prevent contracture, and tendon transfer for established deformity, while foot drop may also be corrected surgically. Underlying all of this is the prevention message: daily self-care — inspecting insensate hands and feet, protecting them from injury and burns, and keeping skin supple — empowers patients to prevent the ulcers they can no longer feel forming.
The counselling dimension is equally clinical and arguably more transformative. Patients and families must be told, clearly and repeatedly, three liberating truths: that leprosy is curable, that a patient on or after MDT is not infectious (the first rifampicin dose renders them rapidly non-contagious), and that the disease is an infection, not a curse, a punishment, or a hereditary taint. Addressing the stigma directly — within the family, the workplace, and the patient's own internalised shame — is essential, because stigma drives late presentation, treatment default, social isolation, and depression. The clinician should connect patients to self-care groups, to rehabilitation (DPMR) services, and to their legal rights and protections (including disability entitlements and anti-discrimination provisions), and should work toward the patient's reintegration into family, work, and community life.
Leprosy Complications: Management Pathway
Management and counselling essentials:
- Plantar ulcer: offloading + wound care + antibiotics if infected + lifelong MCR footwear; daily self-care to prevent recurrence.
- Lagophthalmos: corneal protection + tarsorrhaphy; claw hand/foot drop: physiotherapy, splinting, tendon transfer.
- Counsel three truths: leprosy is curable, treated patients are not infectious, and it is an infection — not a curse or hereditary.
- Tackle stigma directly; link to self-care groups, DPMR rehabilitation, legal rights, and support reintegration.
SELF-CHECK
When counselling a newly diagnosed leprosy patient and their family, which set of messages is correct and most important for reducing stigma and ensuring adherence?
A. Leprosy is hereditary, so other family members should be isolated as a precaution
B. Leprosy is curable with treatment, a patient on MDT quickly becomes non-infectious, and it is an infection — not a curse or a punishment
C. The patient should be kept separate from the family until all skin lesions have completely disappeared
D. Leprosy cannot be cured but can be controlled lifelong, so the patient must accept permanent isolation
Reveal Answer
Answer: B. Leprosy is curable with treatment, a patient on MDT quickly becomes non-infectious, and it is an infection — not a curse or a punishment
The core counselling messages are that leprosy is CURABLE with multidrug therapy, that a patient becomes rapidly NON-INFECTIOUS once treatment begins (the first rifampicin dose kills the great majority of viable bacilli), and that it is an infectious disease — NOT a curse, a punishment, or a hereditary condition. These truths directly counter the stigma and myths that drive late presentation, isolation, and treatment default. The other options perpetuate harmful, false beliefs (heredity, the need for isolation, incurability) that worsen stigma and are factually wrong.
Self-Assessment — Leprosy Disability and Counselling
Consolidate this module by reasoning from a patient's deformities to a complete management and counselling plan, because real leprosy care demands that you handle the physical and the psychosocial together. For each scenario, work through a consistent sequence: identify the deformity and the nerve responsible, assign the WHO disability grade to the affected part, decide the immediate management and whether specialist or surgical referral is indicated, and then frame the counselling messages the patient and family need. Hold two anchors firmly: the WHO grading scale (0 = normal, 1 = anaesthesia only, 2 = visible deformity/damage) applied separately to eye, hand, and foot; and the three liberating counselling truths — curable, non-infectious on treatment, and an infection rather than a curse.
Test yourself on these:
- A patient with clawing of the ring and little fingers: name the nerve, grade the hand, and state the management options including when surgery is considered.
- A foot with a painless ulcer on an anaesthetic sole: name the responsible nerve, outline ulcer management, and state how recurrence is prevented.
- An eye that will not fully close: name the nerve, grade the eye, and give the immediate corneal-protection and referral plan.
- A cured patient who believes his disease is a family curse and whose community shuns him: outline the key counselling points and the support and rehabilitation services you would mobilise.
If you can move from deformity to nerve, to grade, to management, and to compassionate, accurate counselling for each, you have met the objective of this module — and grasped the true burden of leprosy.
CLINICAL PEARL
In leprosy, motor nerve loss deforms and sensory nerve loss ulcerates — and the patient with an anaesthetic sole will not feel the ulcer forming, so you must teach daily self-inspection and prescribe protective (MCR) footwear before the first ulcer appears. Grade every patient's eye, hand, and foot on the WHO 0-1-2 scale at each visit so deterioration is caught early; remember lagophthalmos (facial nerve) is sight-threatening and needs corneal protection and tarsorrhaphy. But the most powerful intervention you have is counselling: tell every patient and family, clearly and repeatedly, that leprosy is curable, that treatment makes them non-infectious within days, and that it is an infection — not a curse, a punishment, or a hereditary taint. Stigma, not the bacillus, is what most often destroys a cured patient's life; dismantling it with truth, and linking the patient to rehabilitation and their legal rights, is core clinical work.