Page 5 of 21
DR3.2 | Grattage Test Technique — SDL Guide
Learning Objectives
- State the clinical indications and contraindications for performing the Grattage test.
- Explain the structural basis (parakeratotic scale, thinned suprapapillary epidermis, dilated dermal capillaries) underlying each grattage sign.
- Demonstrate the graded scraping technique that sequentially elicits the candle-grease sign, the last (glistening) membrane, and the Auspitz sign.
- Interpret positive, partial, and negative grattage findings and use them to support or refute a diagnosis of psoriasis.
- Apply the test to worked clinical scenarios and recognise common technical errors.
INSTRUCTIONS
The Grattage test (Brocq's method) is a simple, instrument-light bedside skill that converts a vague 'scaly red plaque' into a confident diagnosis of psoriasis. Where the recognition module (DR3.1) taught you to read the plaque, this module teaches you to perform a defined procedure correctly — to scrape in a graded way, to observe three sequential endpoints, and to interpret what they mean. Done well it is diagnostic and reassuring; done carelessly (with a sharp blade, on the wrong skin, or stopping too early) it misleads. This is a hands-on skill SDL: master the sequence, the instrument, and the interpretation.
References
- IADVL Textbook of Dermatology, Section on Clinical Methods — Grattage / Brocq's method (textbook)
- Neena Khanna, Illustrated Synopsis of Dermatology & STD, Ch. on Psoriasis (bedside signs) (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
Two patients sit in your OPD with almost identical complaints: a red, scaly patch on the scalp margin. One has psoriasis; the other has seborrhoeic dermatitis. They will receive entirely different treatment, yet at a glance they look the same. You have no biopsy result, no laboratory, and a queue of patients waiting. What you do have is a wooden spatula and the bedside skill to use it. You take the first patient's plaque, scrape it in a graded, controlled way, and watch: silvery flakes lift like candle wax, a glistening film appears, and then a row of tiny bleeding points wells up. The Grattage test has just told you this is psoriasis. You scrape the second patient's greasy yellow scale and nothing of the sort happens. In under a minute, a simple manual technique has separated two diseases — that is the power of doing this procedure well.
WHY THIS MATTERS
Bedside diagnostic skills matter most precisely where you will work as a young doctor — in district hospitals, PHCs, and busy clinics where histopathology and dermoscopy are not instantly available. The Grattage test costs nothing, takes a minute, and meaningfully shifts the probability of a psoriasis diagnosis, which in turn determines whether your patient is started on a topical, referred for phototherapy, or warned away from harmful systemic steroids. Equally, knowing how to perform it correctly protects your patient from harm: an over-vigorous or sharp-instrument 'test' can lacerate skin and produce false bleeding, while testing inflamed or erythrodermic skin can worsen the disease. Competence in this small procedure is therefore a genuine clinical asset and a marker of careful, safe practice.
RECALL
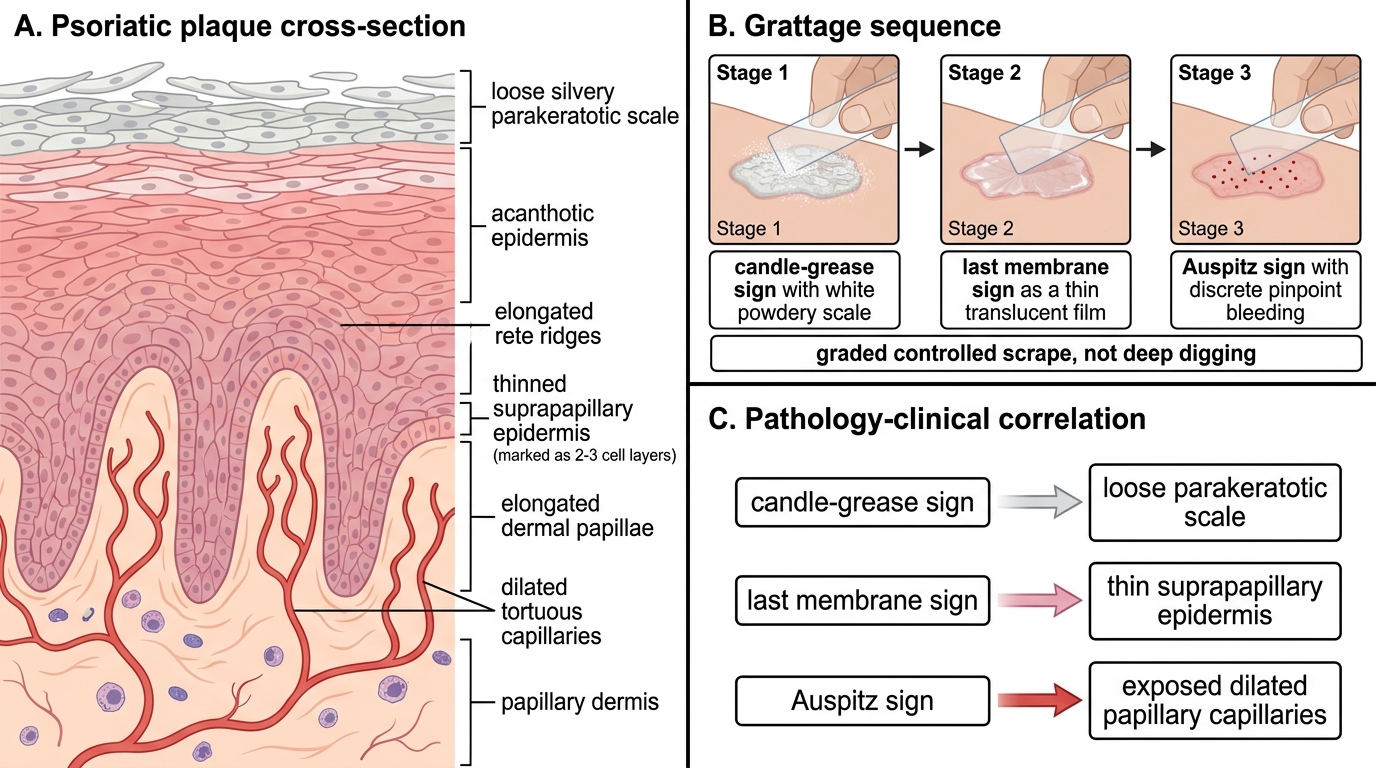
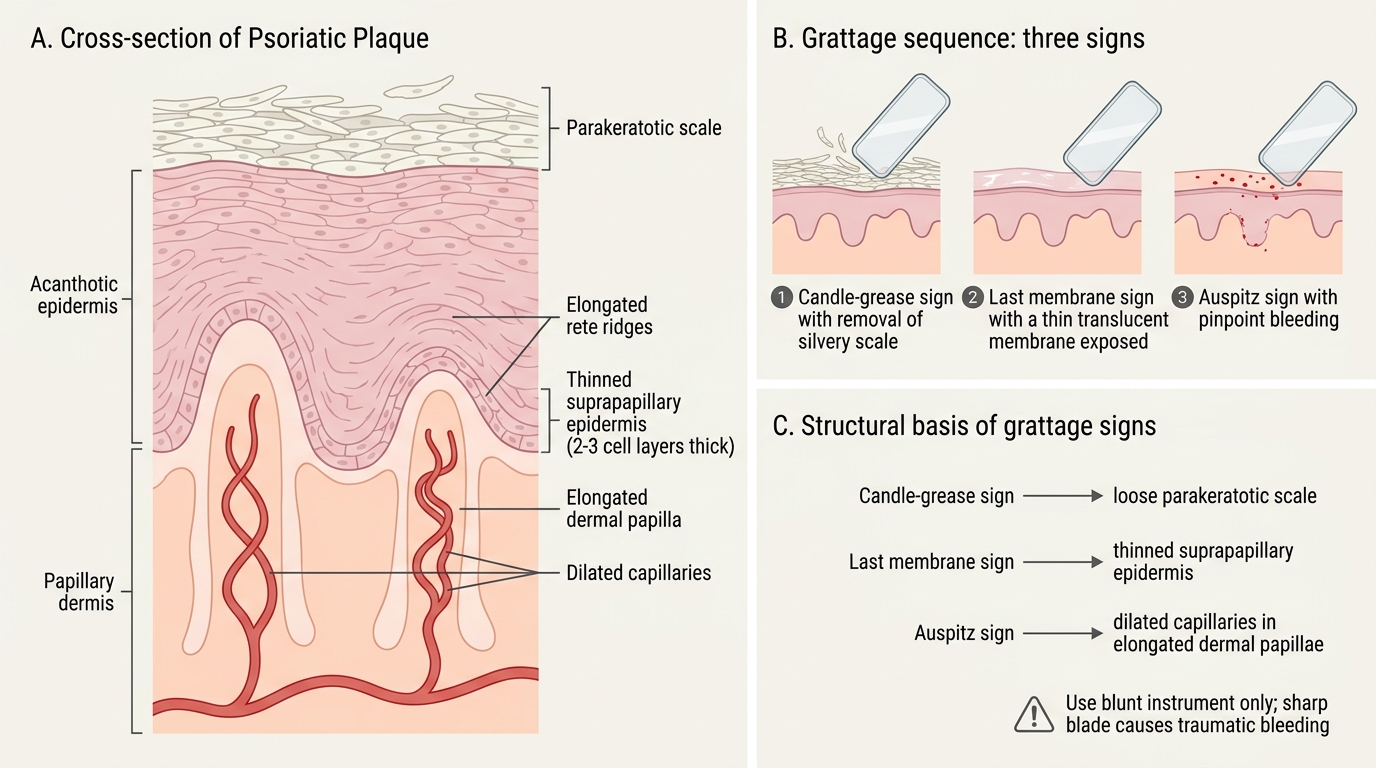
Recall from DR3.1 the morphology of the psoriatic plaque — silvery scale, the candle-grease sign on scraping, and the pinpoint Auspitz bleeding — and from your anatomy and histology the layered structure of the epidermis sitting on the dermis below. Two structural facts are about to become the whole explanation of this test. First, psoriatic scale is parakeratotic and only loosely attached, so it strips off easily in layers. Second, in psoriasis the epidermis overlying the dermal papillae is markedly thinned (only two to three cell layers thick), and those dermal papillae carry dilated, tortuous capillaries brought close to the surface. Keep both facts in mind: each of the three signs you are about to elicit is a direct, predictable consequence of this altered architecture.
Clinical Indications for Grattage Testing
Clinical Indications and Cautions for Grattage Testing
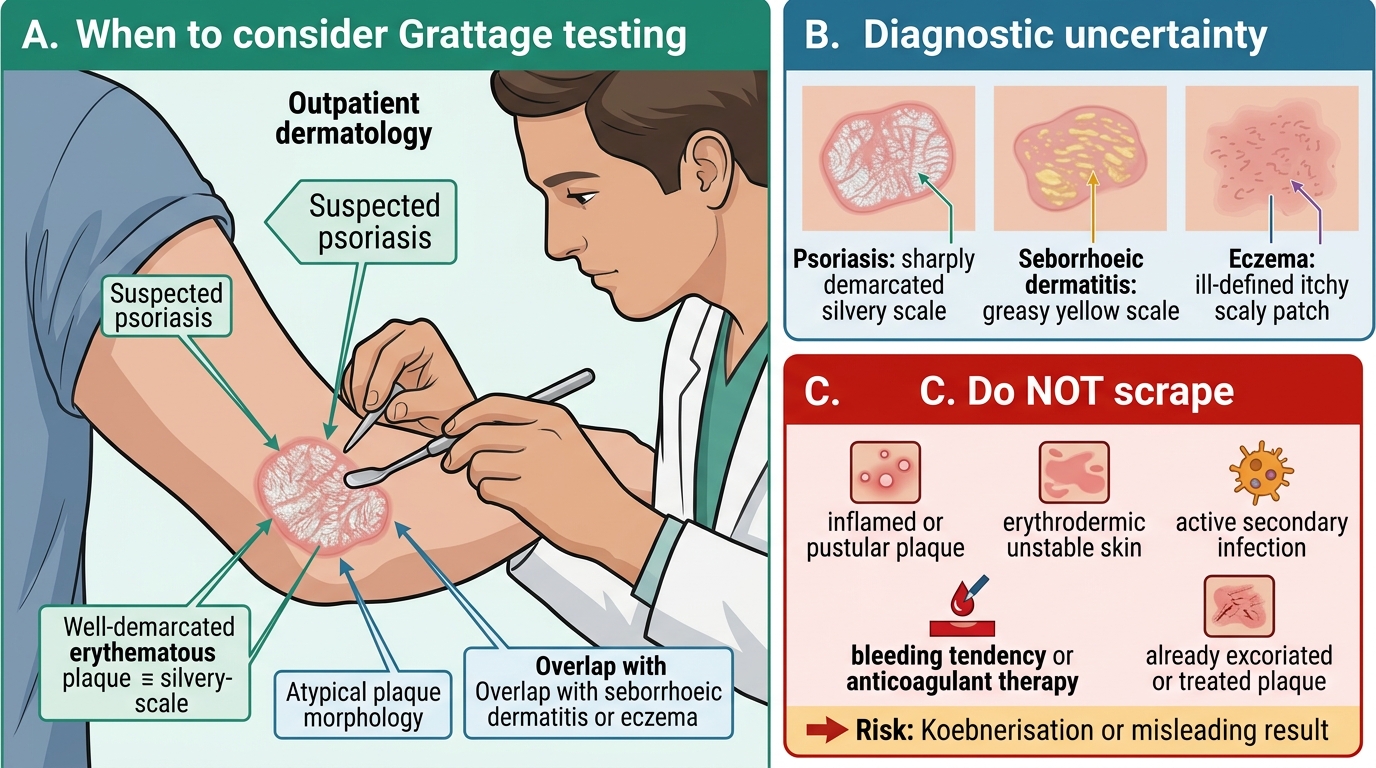
The Grattage test earns its place in clinical practice as a quick, low-cost way to resolve diagnostic uncertainty at the bedside, and knowing when to reach for it — and when not to — is the first part of competence. Its principal indication is the differentiation of suspected psoriasis from its erythematosquamous mimics, most often seborrhoeic dermatitis, but also from eczema or other scaly plaques where the diagnosis is not visually obvious. It is especially useful in the outpatient setting before committing a patient to a treatment pathway, and as a teaching demonstration of the elegant link between psoriatic histology and clinical signs. Just as important is recognising when the test is unsafe or unhelpful, because applying it indiscriminately can harm the patient or mislead you.
Indications:
- Suspected psoriasis where the plaque morphology is atypical or overlaps with seborrhoeic dermatitis or eczema.
- Confirmation of a clinical impression before starting treatment in the OPD.
Contraindications and cautions:
- Acute inflamed, pustular, or erythrodermic psoriasis — do not scrape inflamed or unstable skin, as it may aggravate the disease and provoke Koebnerisation.
- Active secondary infection of the lesion.
- Bleeding tendency or anticoagulant therapy (the Auspitz endpoint involves capillary bleeding).
- Already excoriated or treated plaques, where prior trauma or therapy invalidates the result.
Principle and Materials for Grattage
Principle of Grattage in Psoriasis
The whole test is an applied lesson in pathology, and understanding the principle is what lets you interpret the findings rather than merely produce them. In psoriasis, the surface scale is parakeratotic — keratinocytes have raced to the surface so fast that they retain their nuclei and pile up as loose, silvery, weakly adherent layers; these strip away cleanly to give the candle-grease sign. Beneath the scale lies a thin film, and below that the suprapapillary epidermis is reduced to just two or three cell layers, so that the dilated capillaries within the elongated dermal papillae sit abnormally close to the surface. Gentle removal of that final film exposes these vessels, which bleed as discrete points — the Auspitz sign. The principle therefore demands a graded, controlled scrape with a blunt instrument, because the diagnostic information lies in the sequence of layers, not in how hard you can dig.
Psoriatic Plaque Cross-Section and Grattage Signs
Materials required:
- A blunt instrument — a glass microscope-slide edge, a wooden spatula, or a blunt curette. A sharp blade is forbidden: it lacerates skin and produces traumatic bleeding that mimics — but is not — a true Auspitz sign.
- Good lighting and a magnifying lens if available.
- Clean gloves and gauze.
- A fresh, well-developed, untreated plaque to test on.
Step-by-Step Grattage Technique
Step-by-Step Grattage Technique in Psoriasis
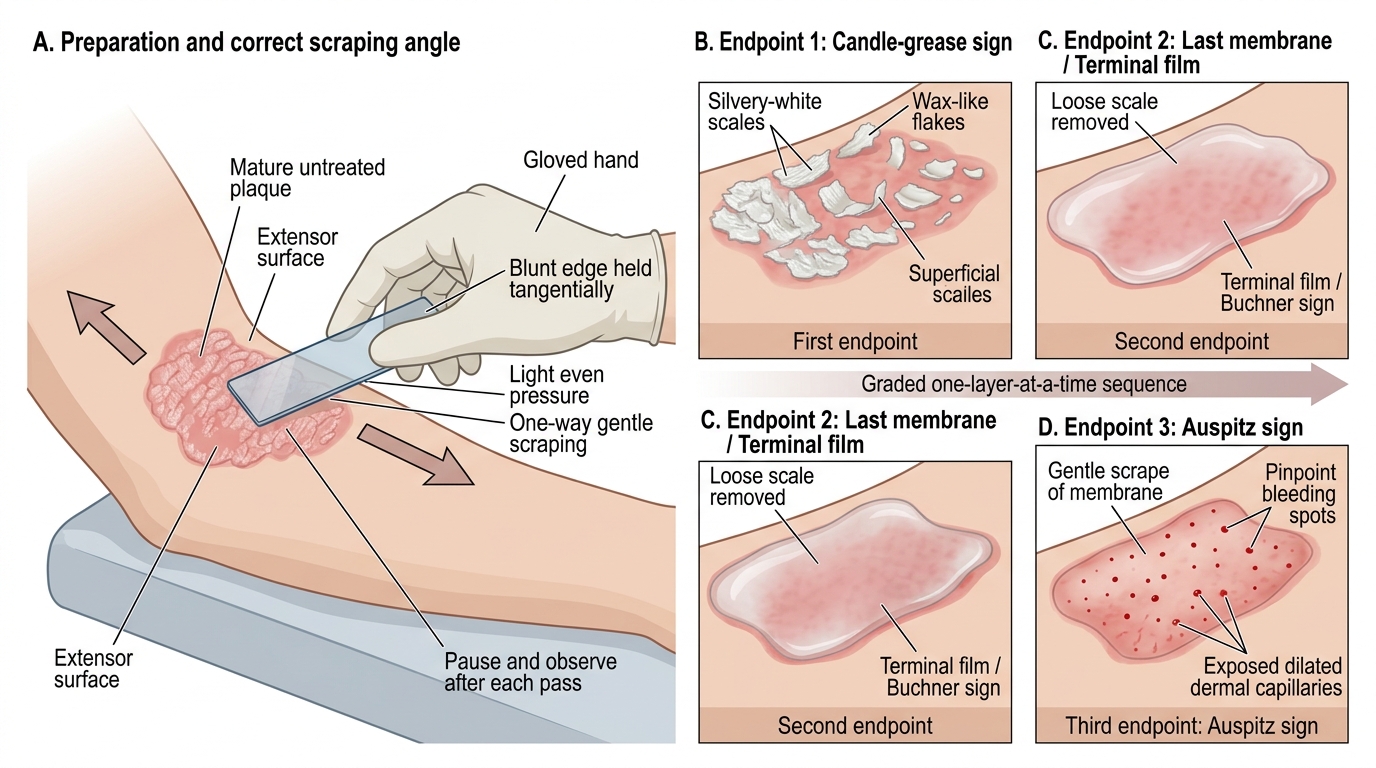
Performing the Grattage test well is about graded, patient scraping and disciplined observation at each layer, because the diagnosis is read from a sequence of three endpoints that must each be looked for in turn. Stopping after the first sign — as inexperienced examiners often do — misses the most specific finding, while scraping too hard skips the orderly layers and produces a wound rather than a sign. Select a mature, untreated plaque on an accessible extensor site such as the elbow or knee, position the patient comfortably, explain in plain language what you are about to do and obtain consent, and put on gloves. Hold your blunt instrument tangentially to the skin and decide in advance that you will pause and observe after each pass rather than scraping continuously to the point of injury. The discipline of advancing exactly one layer at a time, and looking before you scrape again, is what makes the test both diagnostic and safe.
The graded sequence:
- With the blunt edge held tangentially, scrape the scale in one direction using light, even pressure. Silvery-white flakes lift off like shavings of wax — this is the candle-grease sign (the first endpoint).
- Continue gentle scraping until the loose scale is fully removed, revealing a thin, smooth, glistening last membrane (also called the terminal film or Büchner sign) — the second endpoint.
- Now scrape this membrane very gently. Discrete pinpoint bleeding spots appear from the exposed dilated dermal papillary capillaries — the Auspitz sign, the third and most specific endpoint.
Look for all three, in order. Use only the pressure needed to advance one layer at a time; force converts a diagnostic test into a wound.
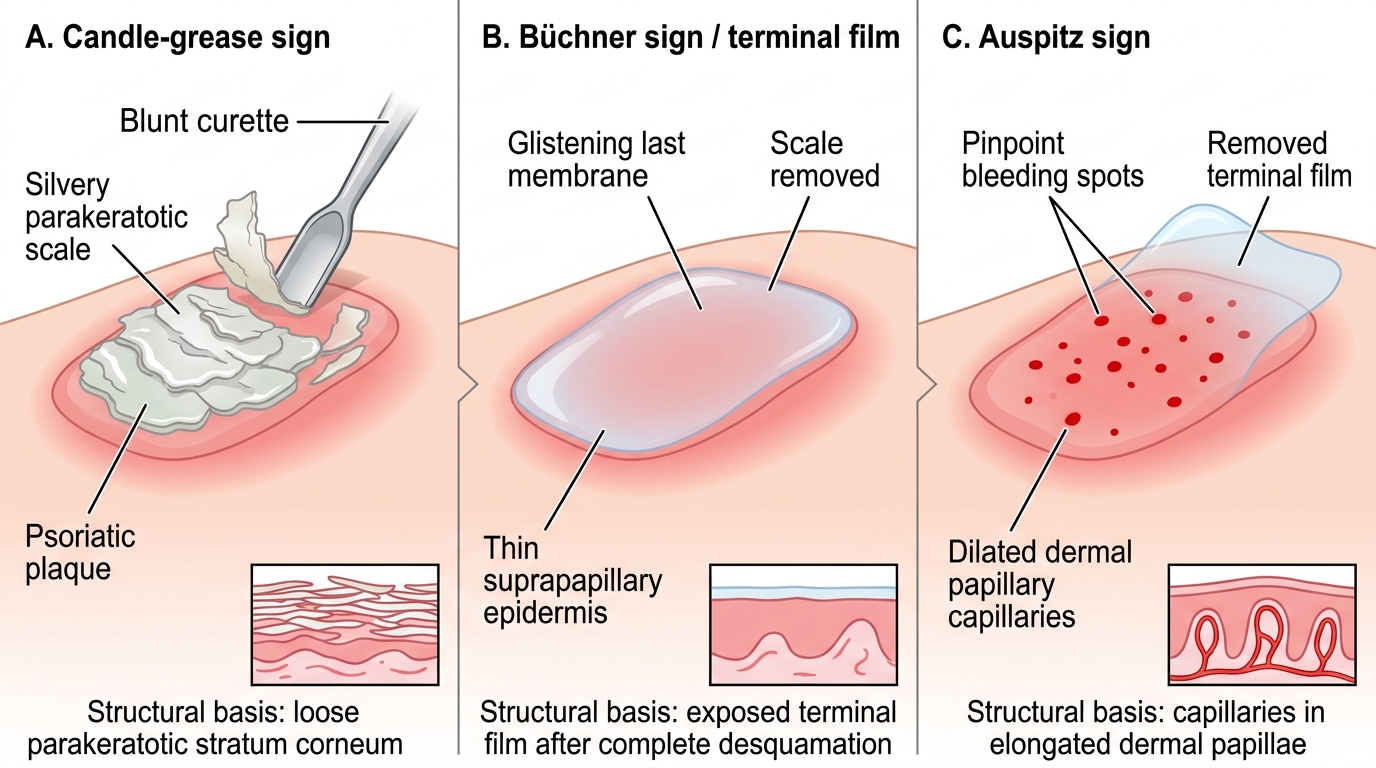
Grattage Test in Psoriasis: Candle-Grease, Büchner, and Auspitz Signs
SELF-CHECK
In which order do the three endpoints of the Grattage test appear as you scrape a psoriatic plaque?
A. Auspitz sign (pinpoint bleeding) → candle-grease sign → glistening last membrane
B. Candle-grease sign (silvery flakes) → glistening last membrane → Auspitz sign (pinpoint bleeding)
C. Glistening last membrane → Auspitz sign → candle-grease sign
D. Candle-grease sign → Auspitz sign → glistening last membrane
Reveal Answer
Answer: B. Candle-grease sign (silvery flakes) → glistening last membrane → Auspitz sign (pinpoint bleeding)
Graded scraping of a psoriatic plaque (Brocq's method) elicits the signs in a fixed sequence: first the candle-grease sign as the loose silvery parakeratotic scale flakes off, then the glistening last membrane (terminal film / Büchner sign) once the scale is fully removed, and finally the Auspitz sign — discrete pinpoint bleeding — when that membrane is gently scraped to expose the dilated dermal papillary capillaries. Stopping early (at candle-grease only) misses the most specific finding.