Page 6 of 21
DR3.2 | Grattage Test Technique — SDL Guide (Part 2)
Interpretation of Grattage Findings
Interpreting Grattage Findings
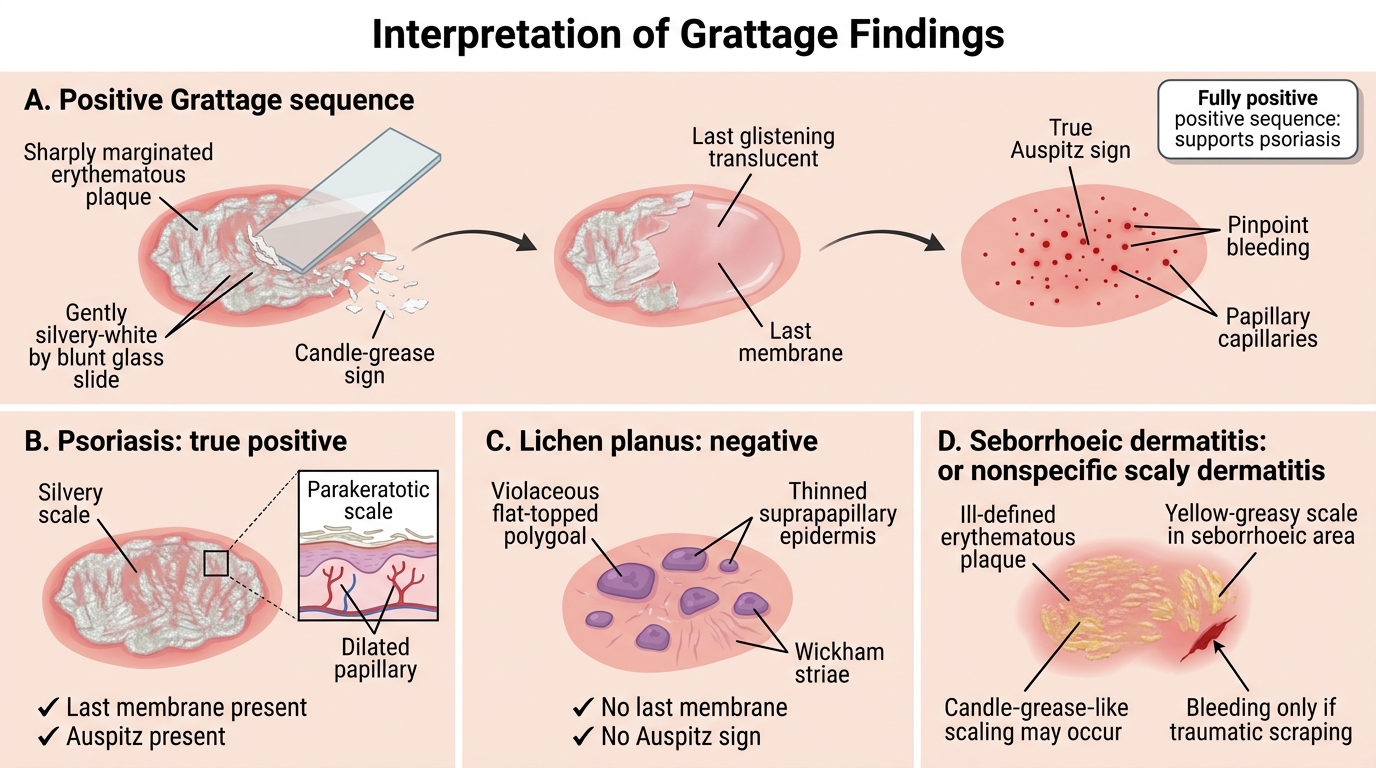
Eliciting the signs is only half the skill; interpreting them correctly is what makes the test diagnostically useful, and this requires distinguishing a true positive from misleading partial results. A fully positive Grattage test — candle-grease sign, then a glistening last membrane, then a true Auspitz sign, appearing in that sequence — strongly supports psoriasis, because the whole sequence reflects the specific psoriatic architecture of loose parakeratotic scale over a thinned suprapapillary epidermis and dilated papillary capillaries. Partial or isolated findings must be read with caution: the candle-grease sign alone is non-specific, because any thick scaly lesion can shed flakes, and pinpoint bleeding produced without the orderly preceding layers may simply be traumatic bleeding from too-vigorous or sharp scraping rather than a genuine Auspitz sign. A negative test — absence of a last membrane and absence of Auspitz bleeding — argues against psoriasis and should prompt you to reconsider the differential.
Grattage Findings in Papulosquamous Disorders
Key interpretive distinctions:
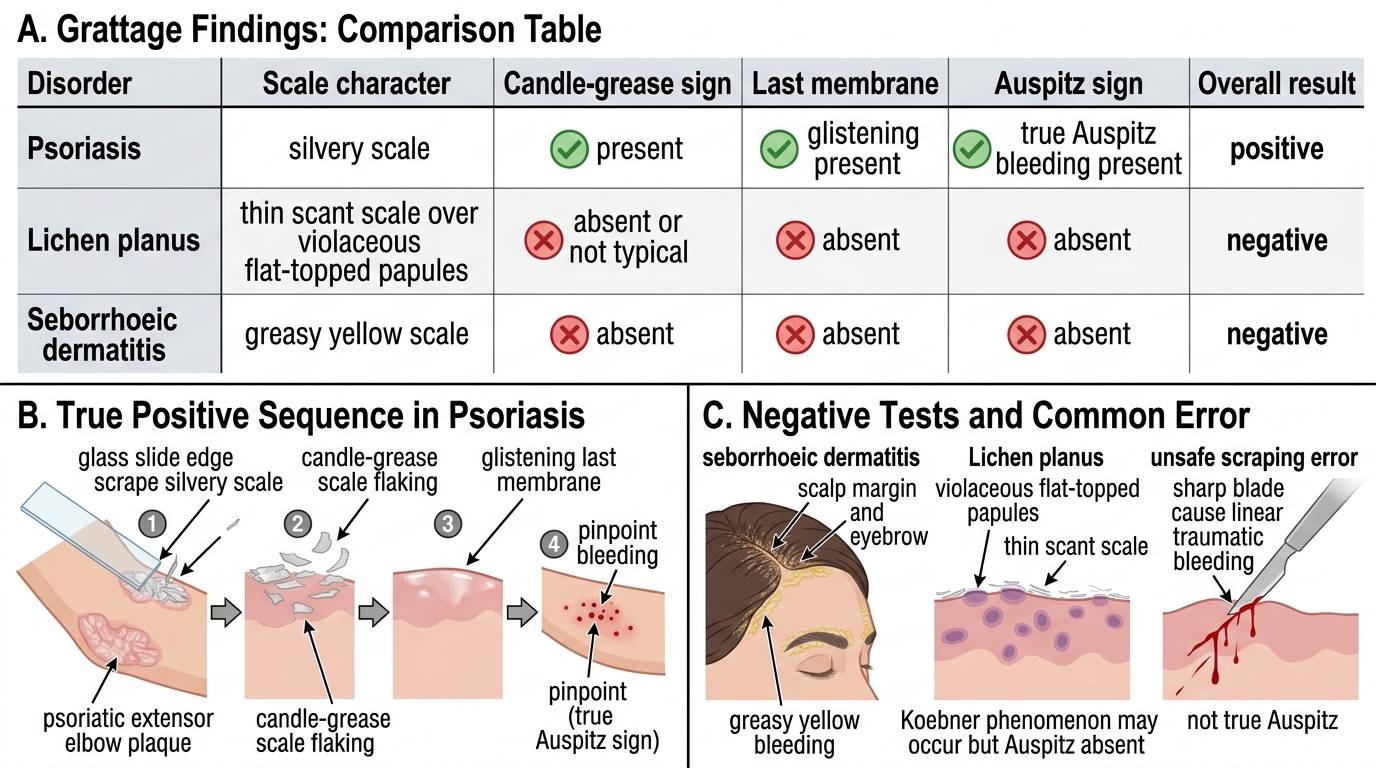
- Psoriasis — silvery scale; candle-grease, last membrane, and true Auspitz all present → positive.
- Seborrhoeic dermatitis — greasy yellow scale; no last membrane, no Auspitz → negative.
- Lichen planus — thin, scant scale, violaceous papules; no Auspitz sign → negative (a key separator, since lichen planus shares the Koebner phenomenon but never gives Auspitz).
- Always ask: is this bleeding a true sequential Auspitz sign, or traumatic bleeding from over-scraping?
Applied Practice — Case Scenarios
Grattage Test and Auspitz Sign: Case-Based Interpretation
Bringing the technique and its interpretation together in worked scenarios is the best way to consolidate the skill and to anticipate the errors that trip up examiners and clinicians alike. Consider two patients who, on first glance, look similar but resolve differently under a correctly performed test, and then review the recurrent technical pitfalls that produce wrong answers. Working through these mentally — predicting what you would see and why — rehearses the clinical reasoning you will use at the bedside.
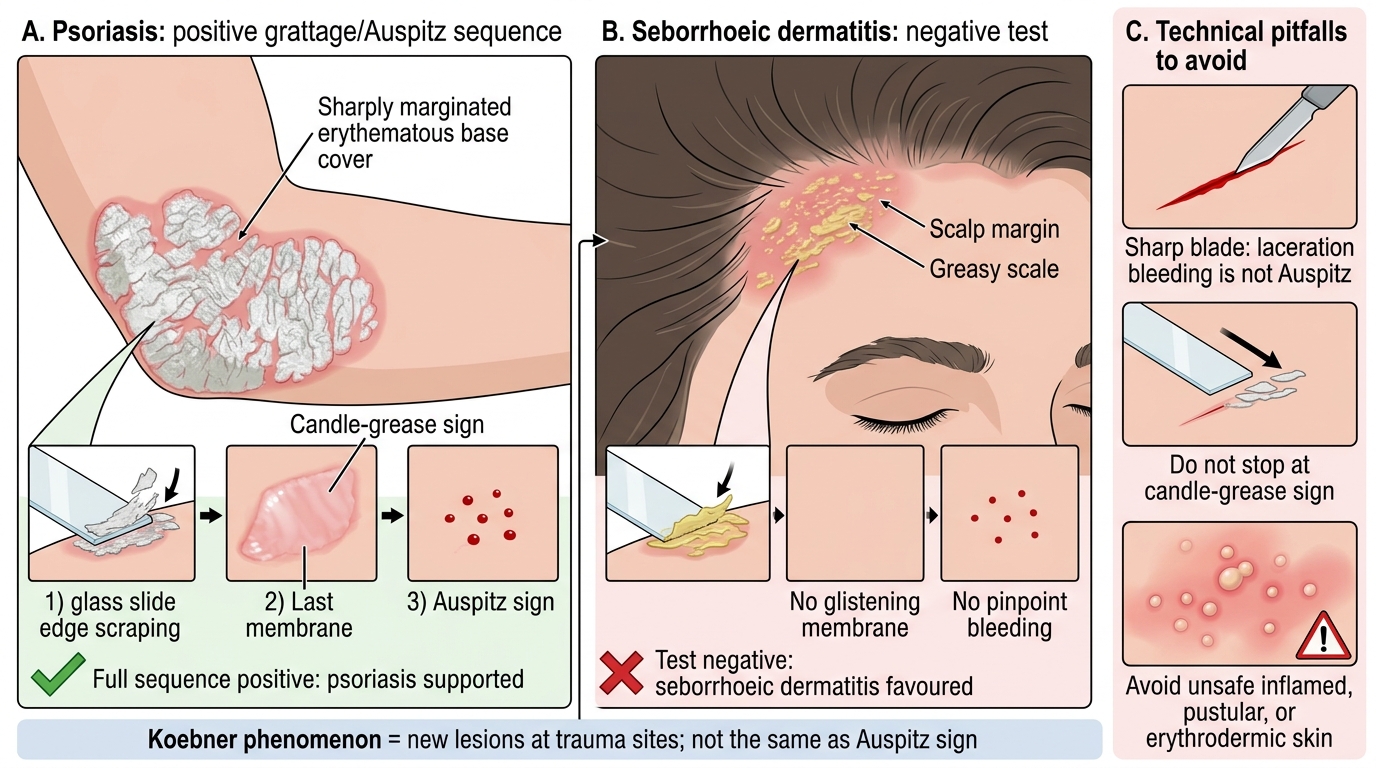
Scenario A: A 40-year-old man has a sharply marginated, silvery-scaled plaque on the extensor elbow. You scrape with a glass slide edge: silvery flakes lift (candle-grease), a glistening membrane appears, and gentle further scraping yields neat pinpoint bleeding (Auspitz). The full sequence is positive → diagnosis of psoriasis is strongly supported.
Scenario B: A 40-year-old man has a red, greasy-scaled patch at the scalp margin and eyebrows. You scrape: the scale is greasy and yellowish, there is no glistening last membrane, and no pinpoint bleeding appears. The test is negative → seborrhoeic dermatitis is favoured, not psoriasis.
Common technical errors to avoid:
- Using a sharp blade — causes laceration bleeding mistaken for Auspitz.
- Stopping after the candle-grease sign and never reaching the Auspitz endpoint.
- Performing the test on inflamed, pustular, or erythrodermic skin (unsafe).
- Confusing the Koebner phenomenon (new lesions at trauma sites) with a grattage endpoint — Koebner is NOT a grattage finding.
SELF-CHECK
A student elicits pinpoint bleeding on a scaly plaque but used a scalpel blade and scraped hard in one go, without first observing silvery flakes or a glistening membrane. How should this finding be interpreted?
A. A definite positive Auspitz sign confirming psoriasis
B. Unreliable — the bleeding may be traumatic from sharp, vigorous scraping rather than a true sequential Auspitz sign
C. A negative grattage test ruling out psoriasis
D. Diagnostic of lichen planus
Reveal Answer
Answer: B. Unreliable — the bleeding may be traumatic from sharp, vigorous scraping rather than a true sequential Auspitz sign
A true Auspitz sign appears only at the end of the graded sequence — after the candle-grease sign and the glistening last membrane — when the thinned suprapapillary epidermis is gently breached to expose dilated dermal capillaries. Bleeding produced by a sharp blade and forceful single scrape, without the preceding orderly layers, is most likely traumatic laceration bleeding and is unreliable. This is exactly why the test must use a blunt instrument and a graded technique.
Self-Assessment — Grattage Skill Check
Test your mastery of this procedural skill by rehearsing not only the facts but the reasoning behind each step, because in an OSCE or at the bedside you will be asked both to perform the test and to justify what you are doing. A competent examiner can state the indications and contraindications, name the correct instrument and explain precisely why a sharp blade is forbidden, demonstrate the graded sequence smoothly, name the three endpoints in their correct order, and interpret positive, partial, and negative results sensibly rather than over-reading a single sign. The most reliable way to consolidate a procedural skill is to verbalise it: explain each step aloud, predict what you expect to see, and account for the structural reason behind every sign. Run through the self-check prompts below as if teaching a junior colleague at the bedside; if you can explain it clearly and safely, you have genuinely understood it.
Self-check prompts:
- What instrument do you use for grattage, and why must it not be sharp?
- Name the three endpoints of the test in the order they appear.
- Why is the Auspitz sign a vascular (capillary) phenomenon rather than a traumatic one?
- Which condition gives greasy scale and a negative test, and which gives violaceous papules and no Auspitz?
- Name two situations in which you would NOT perform the test.
CLINICAL PEARL
Treat the Grattage test as a sequence, not a single scrape. The candle-grease sign alone proves little — almost any thick scale flakes — and bleeding produced by digging hard with a sharp instrument is a wound, not a sign. The diagnostic value lies in seeing all three endpoints in order: silvery flakes, then a glistening last membrane, then neat pinpoint Auspitz bleeding, produced with a blunt edge and the gentlest pressure that advances one layer at a time. And never scrape inflamed, pustular, or erythrodermic skin — you risk Koebnerising and worsening the disease you are trying to diagnose.