Page 11 of 21
DR4.1 | Lichen Planus Diagnosis and Management — SDL Guide
Learning Objectives
- Describe the cardinal morphology of lichen planus using the classic 'P' features and Wickham striae.
- Outline the etiopathogenesis of lichen planus as a T-cell-mediated lichenoid reaction and list its drug and viral associations.
- Recognise the clinical patterns of cutaneous, oral, nail, and scalp lichen planus and their histological correlates.
- Differentiate lichen planus from psoriasis and other mimics at the bedside and by investigation.
- Devise a management plan for lichen planus, including the appropriate (and permitted) use of systemic corticosteroids.
INSTRUCTIONS
Lichen planus is the second great papulosquamous disease you must master, and it is the natural counterpart to psoriasis: both are common, both itch, both Koebnerise — but they look different, behave differently, and are treated differently. This module teaches you to recognise lichen planus on the skin, in the mouth, on the nails, and on the scalp; to understand why it looks the way it does; to separate it confidently from psoriasis; and to plan its treatment. A key teaching point distinguishes it sharply from psoriasis: in lichen planus, unlike psoriasis, systemic corticosteroids are a legitimate and useful treatment.
References
- IADVL Textbook of Dermatology, Section on Papulosquamous Disorders — Lichen Planus (textbook)
- Neena Khanna, Illustrated Synopsis of Dermatology & STD, Ch. on Lichen Planus (textbook)
Version 2.0 | NMC CBME 2024
CLINICAL SCENARIO
A 45-year-old woman complains of intensely itchy purple bumps on her wrists and ankles that have appeared over the past two months, along with a painful, rough sensation in her mouth when she eats spicy food. A relative told her it was 'the same skin disease as the neighbour' — who in fact has psoriasis — and she has been using a leftover psoriasis cream without benefit. When you examine her, the lesions are not red silvery-scaled plaques at all; they are flat-topped, violaceous, polygonal papules, and on close inspection their surface carries a fine, white, lacy network. Inside her cheeks you find a similar lacy white pattern. This is lichen planus, a different disease entirely, and its recognition turns on reading these distinctive features — the violaceous colour, the flat top, and the white striae — rather than assuming every itchy papular rash is psoriasis.
WHY THIS MATTERS
Lichen planus is common enough that you will meet it repeatedly, and its tendency to involve mucosa, nails, and scalp means it can present to dentists, physicians, and surgeons as well as dermatologists. Recognising it matters because it is frequently confused with psoriasis, lichenoid drug reactions, and — in the mouth — with leukoplakia and candidiasis, each of which is managed differently. Oral lichen planus in particular carries a small but real risk of malignant transformation, so identifying it commits you to surveillance, not just symptom relief. And because some cases are triggered by drugs or associated with hepatitis C, recognising lichen planus prompts a search for a reversible cause. Distinguishing it from psoriasis is also clinically consequential, since the two diseases differ in their safe use of systemic steroids.
RECALL
Recall from DR3.1 the features of psoriasis — erythematous silvery-scaled plaques, the Auspitz sign, extensor distribution — because lichen planus will be defined largely by contrast with these. Recall, too, from your immunology the concept of a T-cell-mediated (type IV, cell-mediated) cytotoxic reaction, in which CD8+ lymphocytes attack target cells and trigger their apoptosis. Hold on to one shared feature you have already met: the Koebner phenomenon, the appearance of new lesions at sites of trauma, occurs in lichen planus just as it does in psoriasis and vitiligo, so it cannot be used to tell these diseases apart. With these anchors in place — the psoriasis picture for contrast, the cytotoxic mechanism for pathogenesis, and the shared Koebner caveat — the distinctive picture of lichen planus will fall into place clearly.
Classic Lichen Planus — Morphology and the 6 P's
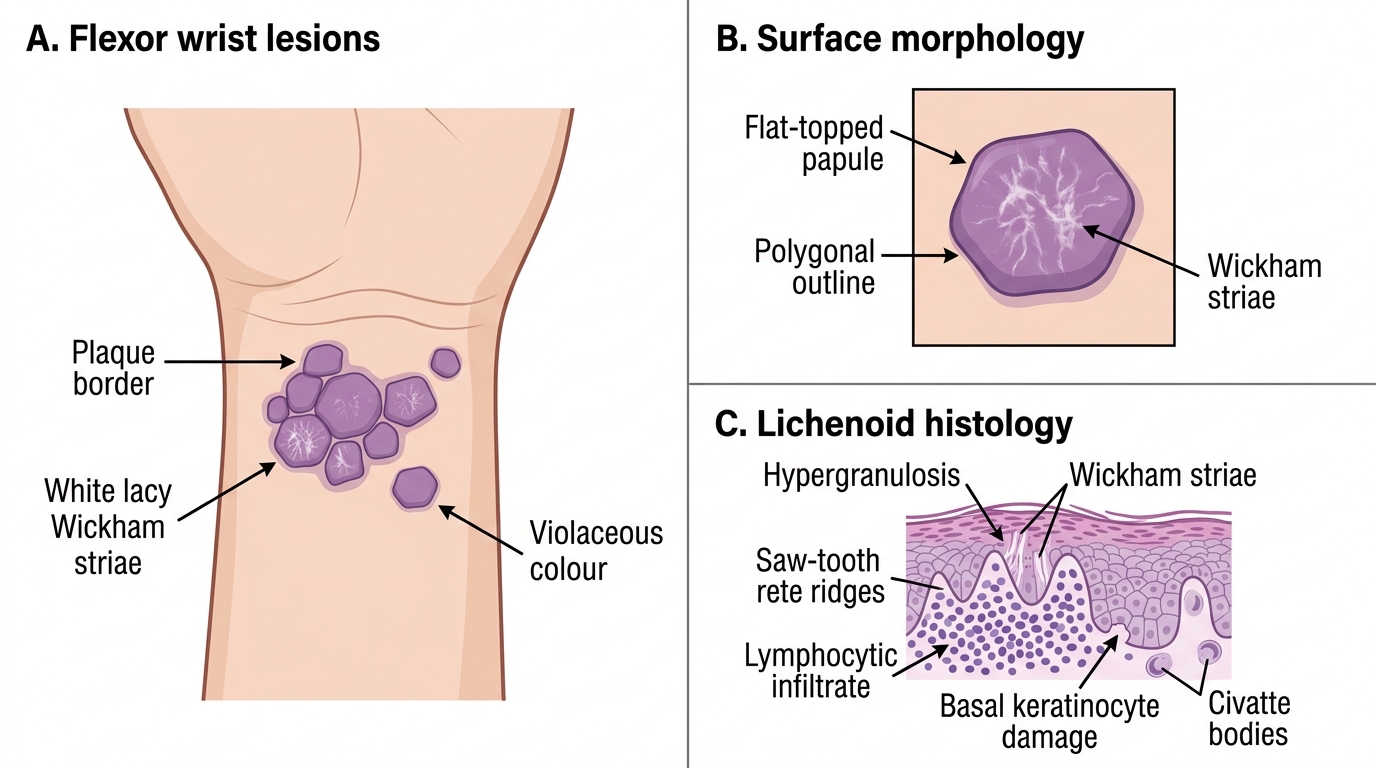
The recognition of lichen planus rests on a memorable cluster of morphological features traditionally summarised by a set of words beginning with 'P', and learning these precisely is the foundation of diagnosis. The classic lesion is a pruritic (itchy), purple (violaceous), polygonal (angular-bordered), planar (flat-topped), and papular lesion — five core P features that, taken together, are highly characteristic. To this list is conventionally added the diagnostic surface sign of fine white lacy lines called Wickham striae, which represent focal thickening of the granular layer and are best seen with a drop of oil or under dermoscopy. (Following Neena Khanna's synopsis, we treat the five clinical P's as the core mnemonic and Wickham striae as the additional defining surface feature, rather than forcing a contested sixth 'P'.) The lesions favour the flexor surfaces of the wrists and forearms, the ankles and shins, and the lumbar region — a flexural predilection that contrasts with the extensor preference of psoriasis.
Lichen Planus: Clinical Morphology and Histology
Several morphological variants exist and are worth recognising:
- Hypertrophic lichen planus — thick, warty, intensely itchy plaques, classically on the shins.
- Atrophic and annular variants — thinned or ring-shaped lesions.
- Linear lichen planus — lesions in a line, often along a scratch (Koebner).
- Post-inflammatory hyperpigmentation is common and prominent in Indian skin after lesions resolve.
Etiopathogenesis of Lichen Planus
Etiopathogenesis of Lichen Planus
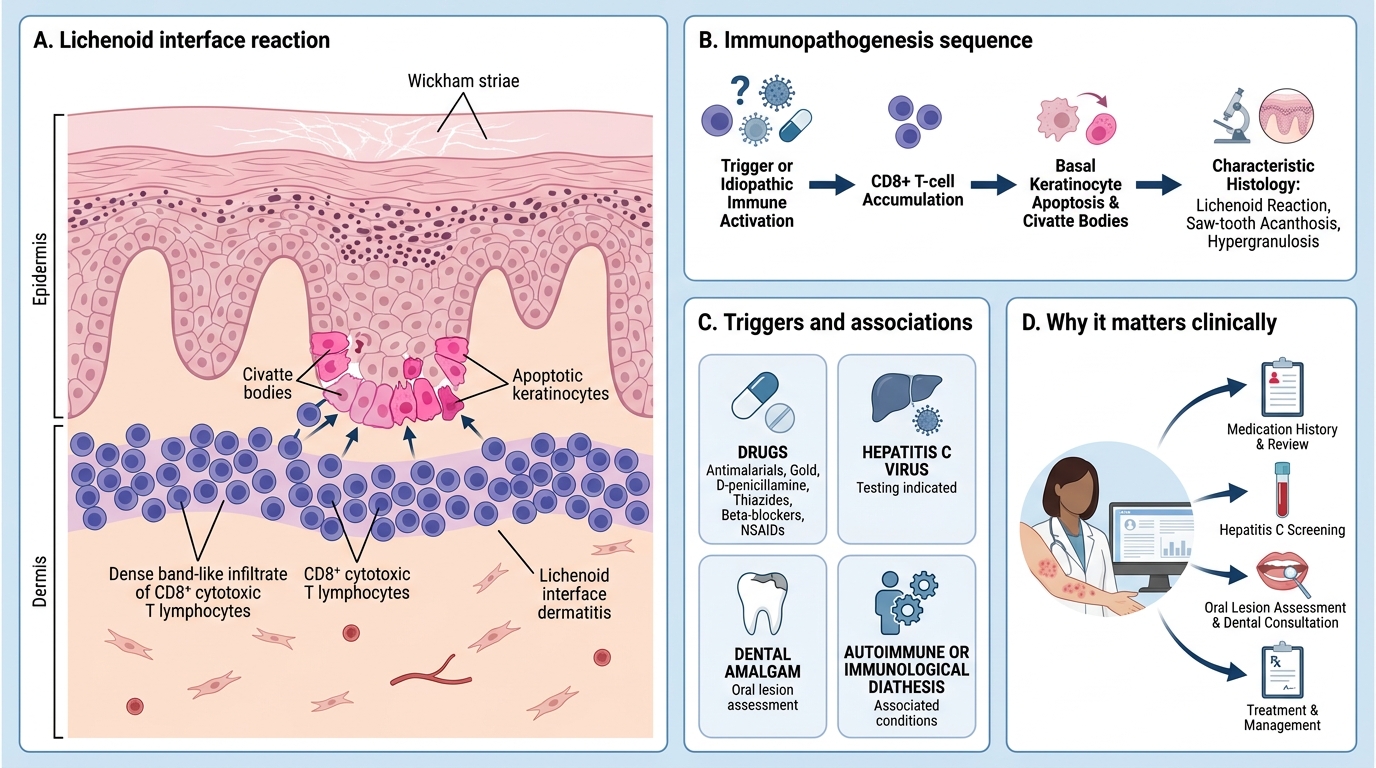
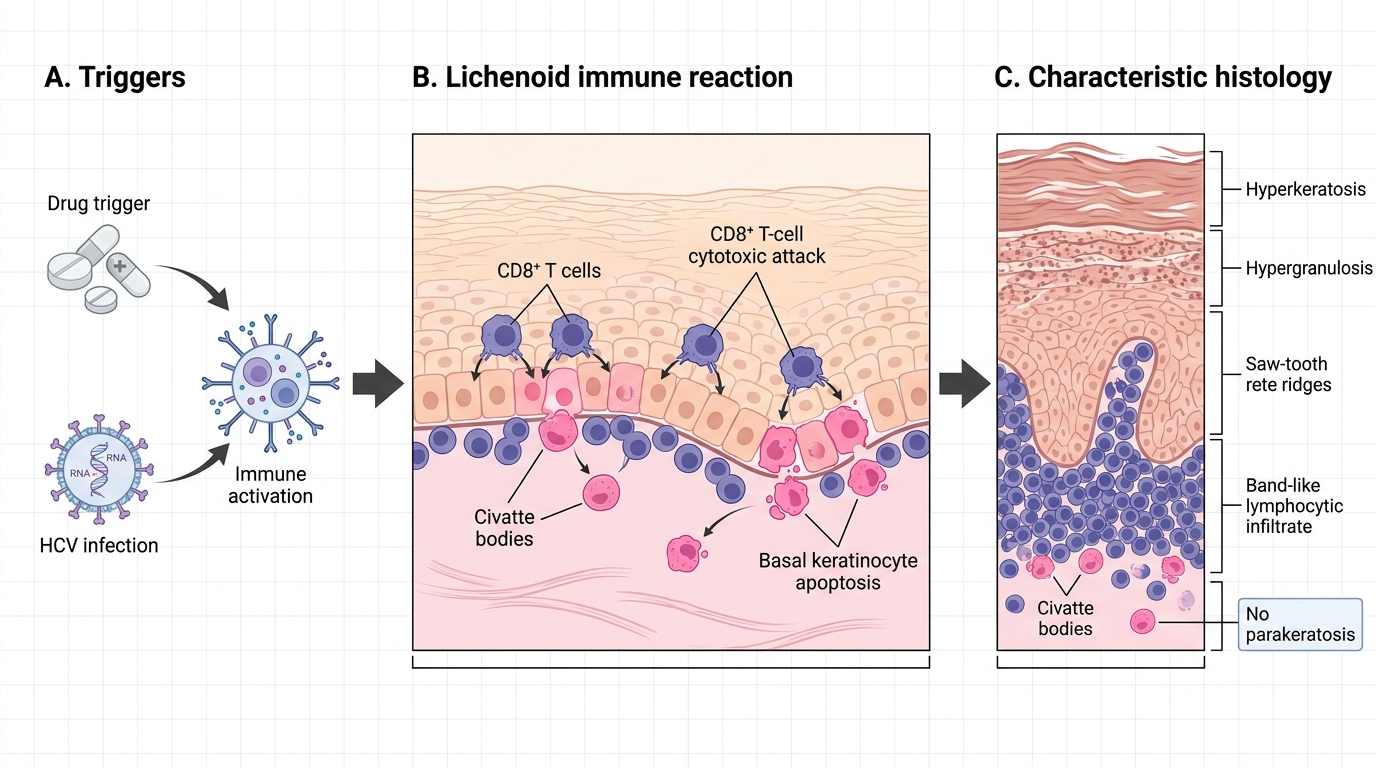
Understanding lichen planus as an immunological reaction at the dermoepidermal junction explains both its appearance and its associations, and gives a rational basis for the investigations you will order. Lichen planus is a T-cell-mediated lichenoid reaction: CD8+ cytotoxic lymphocytes accumulate in a dense band at the junction between epidermis and dermis and attack the basal keratinocytes, driving them into apoptosis. These dying keratinocytes are seen histologically as Civatte bodies (also called colloid or hyaline bodies), and the band-like lymphocytic infiltrate, together with a 'saw-tooth' irregular acanthosis of the rete ridges and hypergranulosis (which produces Wickham striae), constitutes the characteristic histology. In the majority of patients the trigger is unknown (idiopathic), but several recognised associations should be sought because some are reversible.
Known triggers and associations:
- Drugs — antimalarials, gold, D-penicillamine, thiazide diuretics, beta-blockers, and NSAIDs can produce a lichenoid drug reaction clinically resembling lichen planus, which resolves on stopping the drug.
- Hepatitis C virus — an established association in many populations; worth testing for, especially with widespread or oral disease.
- Dental amalgam — a contact trigger for oral lichenoid lesions adjacent to fillings.
- An immunological/autoimmune diathesis in idiopathic cases.
Clinical Features — Skin, Oral, Nail, and Scalp LP
Clinical Features of Lichen Planus
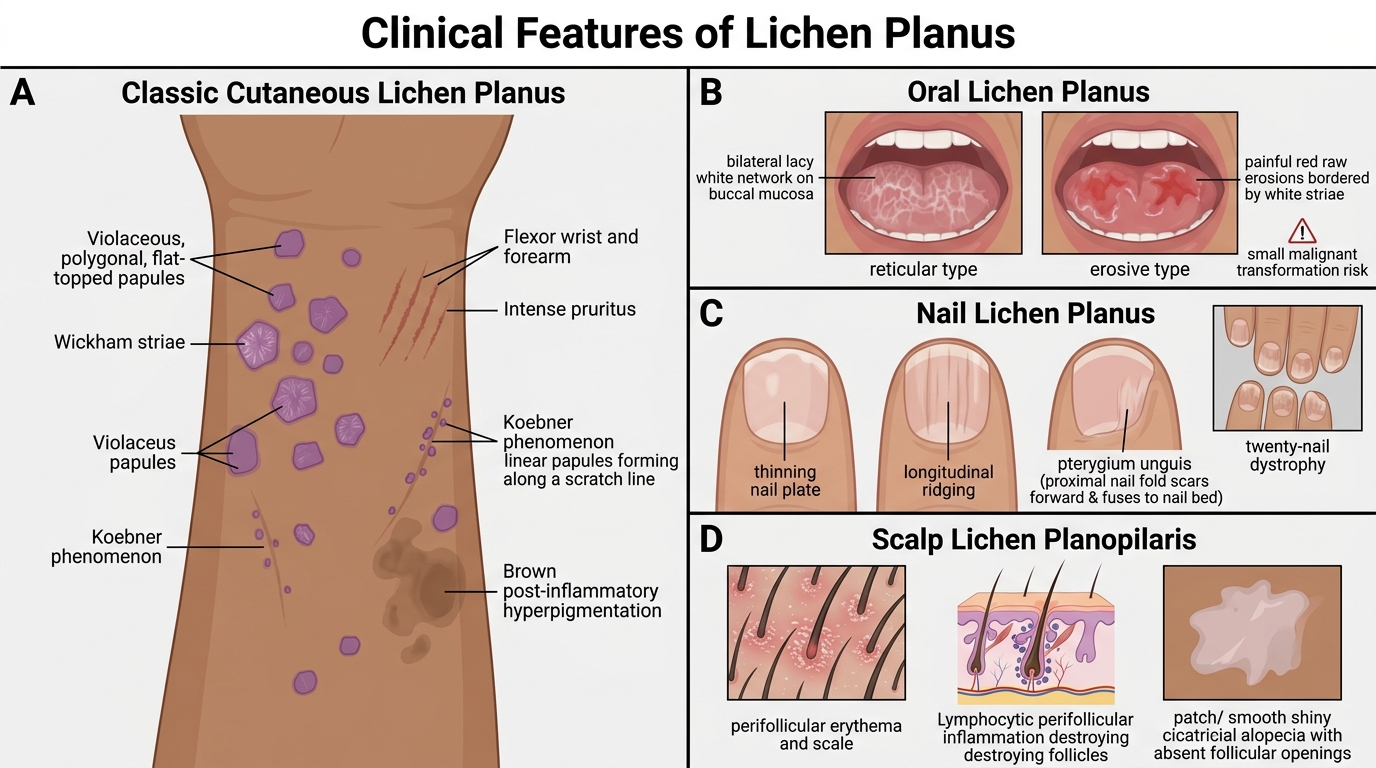
Lichen planus is not confined to the skin, and a complete assessment requires examining the mucosa, nails, and scalp, because involvement of these sites changes both the diagnosis and the prognosis. On the skin, the classic violaceous flat-topped papules with Wickham striae appear at flexural sites, are intensely itchy, demonstrate the Koebner phenomenon, and often leave marked post-inflammatory hyperpigmentation in pigmented skin. In the mouth, oral lichen planus is common and takes three main forms: the reticular type (the commonest, a bilateral lacy white network on the buccal mucosa, usually asymptomatic), the erosive type (painful raw erosions that carry a small risk of malignant transformation), and a less common plaque type. On the nails, lichen planus can cause thinning, longitudinal ridging, and the pathognomonic pterygium unguis — a scar that fuses the proximal nail fold to the nail bed — as well as a twenty-nail dystrophy. On the scalp, the follicular variant lichen planopilaris produces perifollicular inflammation that destroys hair follicles and results in permanent scarring (cicatricial) alopecia.
T-Cell-Mediated Lichenoid Reaction
The diagnosis is usually clinical but is confirmed where needed by skin biopsy showing the characteristic lichenoid histology — saw-tooth rete ridges, a band-like lymphocytic infiltrate, Civatte bodies, hypergranulosis, and hyperkeratosis without parakeratosis (a useful contrast with psoriasis, which shows parakeratosis).